
Abstract
Gradenigo syndrome is a clinical triad of abducens nerve palsy, retro-orbital pain (trigeminal ganglionitis), and chronic otorrhea (otitis media). The etiology of Gradenigo syndrome results from apical petrositis secondary to suppurative otitis media. Although apical petrositis has gradually become uncommon in modern society due to the widespread use of antibiotics, Gradenigo syndrome should be considered in the differential diagnosis of a child’s diplopia.
A 5-year-old boy presented with left-sided diplopia and retro-orbital pain for 2 weeks. Previously, persistent otorrhea following a ventilation tube insertion for serous otitis media was noted. Otoscopy revealed a bulging, erythematous eardrum. Physical examination showed a normal extraocular movement when patient looked to right (Figure 1A). However, the left lateral rectus palsy was noted when he looked to left (Figure 1B).
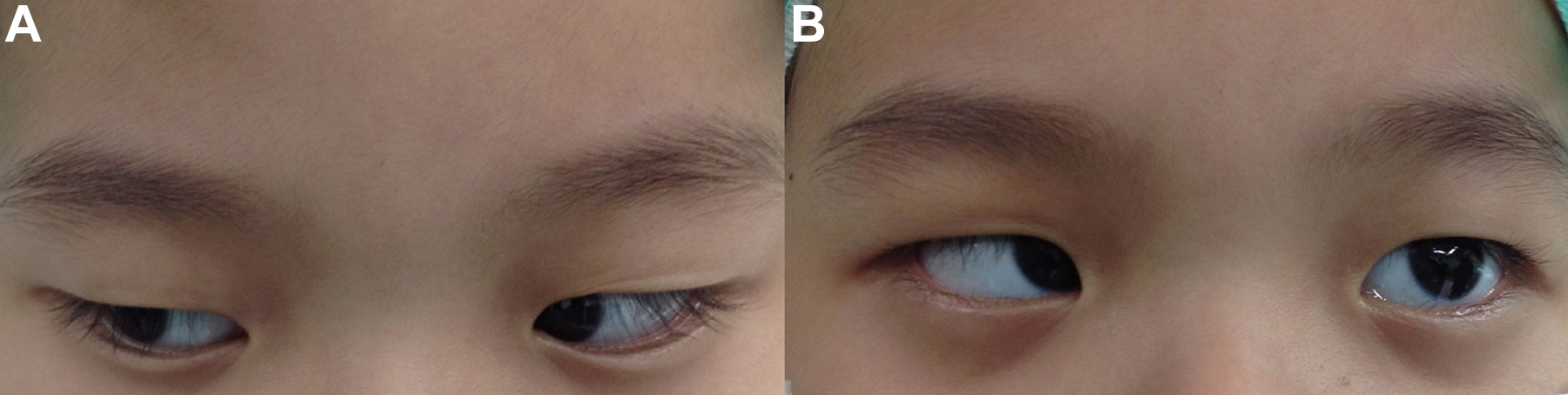
A, Normal movement of extraocular muscle when looking to right. B, Left lateral rectus muscle palsy (abducens nerve palsy) when looking to left.
Laboratory data revealed a mild elevated C-reactive protein level (15.19 mg/L; normal: <5 mg/L) without leukocytosis (4800/µL; normal: 3900-10 600/µL).
Computed tomography (Figure 2A) displayed a complete opacification of the left middle ear cavity and mastoid air cells, and the otomastoiditis was impressed. Magnetic resonance imaging (MRI; Figure 2B) showed a hyperintensity on T2 modality with heterogeneous enhancement pattern, extending to petrous bone apex, occipital condyle, and internal acoustic canal.
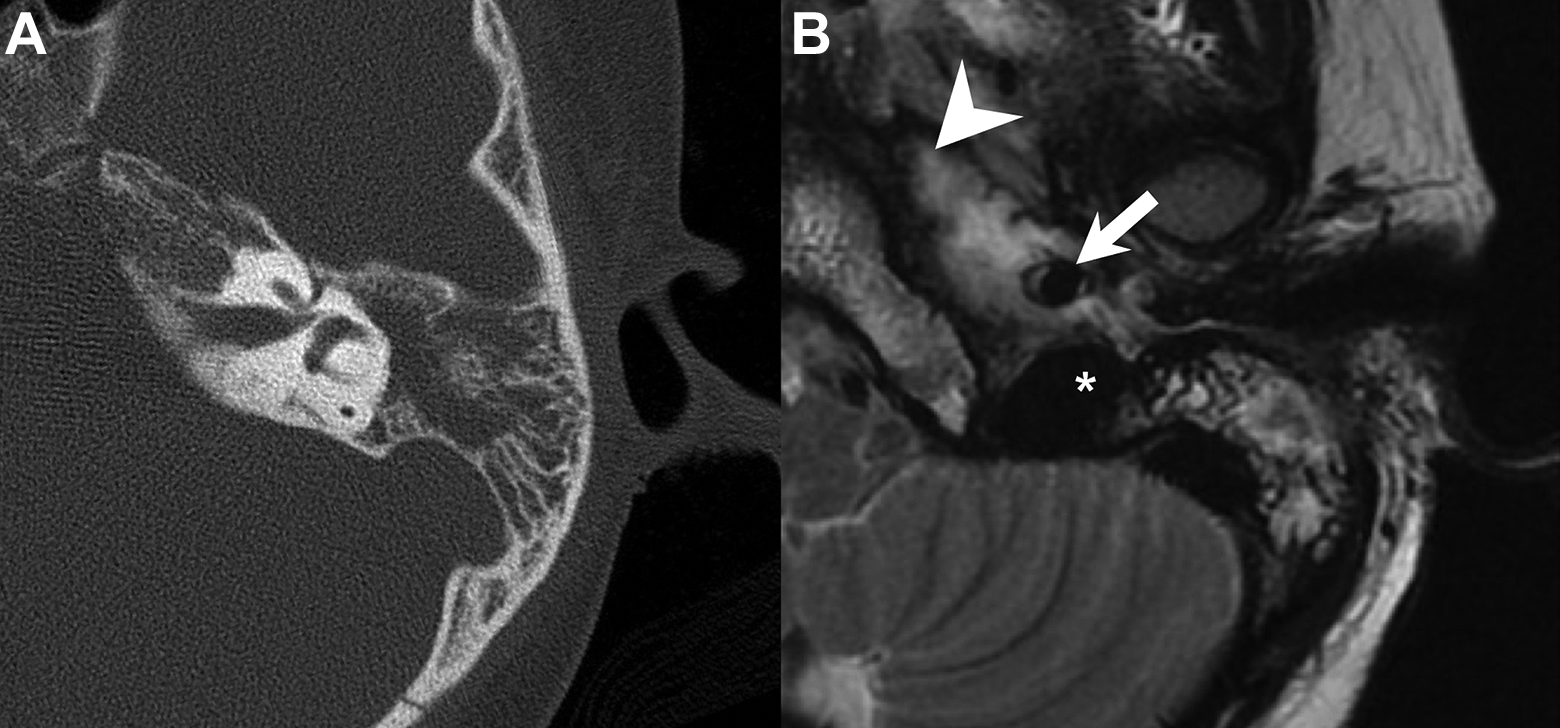
A, Opacification of middle ear and mastoid with involvement of the petrous apex in computed tomography. B, Left apical petrositis in T2-weighted magnetic resonance imaging. Apical petrositis (arrowhead), carotid artery (arrow), and jugular bulb (asterisk).
The diagnosis of Gradenigo syndrome was confirmed. Gallium(GA)-67 inflammation scan revealed multiple focal areas of increased uptake of fluorodeoxyglucose in the petrous portion of the left temporal bone and surrounding soft tissue with active inflammatory process.
Surgical management with myringotomy with ventilation tube and cortical mastoidectomy for pus culture were achieved because of poor response to empiric use of ceftriaxone. The causative pathogen yielded Pseudomonas aeruginosa, and the symptom gradually resolved with complete neurologic recovery following a 6-week course of intravenous cefepime administration postoperatively.
Gradenigo syndrome is a rare clinical symptom triad of diplopia (ipsilateral abducens nerve palsy), unilateral retro-orbital pain (trigeminal ganglionitis), and chronic otorrhea (otitis media).1,2
It could occur as a complication of acute or chronic otitis media. 3 Actually, Gradenigo syndrome was first described in 1907 by Guiseppe Gradenigo. 4
The etiology of Gradenigo syndrome results from apical petrositis secondary to suppurative otitis media. The extradural inflammation caused by apical petrositis would further involve trigeminal ganglion (the fifth cranial nerve) and abducens nerve (the six cranial nerve). 5 In fact, due to the widespread use of antibiotics for otitis media, apical petrositis has gradually become uncommon in modern society. 1 However, Gradenigo syndrome is different from apical petrositis because only 13% to 42% of patients would develop the classic symptom triad of Gradenigo syndrome.6,7 In addition to children, immunosuppressed patients are also more susceptible to developing this disease. 5
Computed tomography and MRI are required to detect deep petrous apex as the inflammatory site and are helpful tools to establish the diagnosis. 4 Computed tomography would show evidence of petromastoid air cell opacification and possible bony erosion. T2-weighted MRI would show hyperintensity over the middle ear, mastoid air cells, and petrous apex.
In our patient, the cultured pathogen was P aeruginosa. In previous literature, organisms reported associated with infection in Gradenigo syndrome included Staphylococcus, Group A Streptococcus, P aeruginosa, Klebsiella pneumoniae, and Mycobacterium tuberculosis. 2
The broad-spectrum and early antibiotics should be given before final pathogens are revealed. For potential morbidity, aggressive surgical intervention such as drainage of the middle ear, mastoidectomy, or apical petrosectomy should be conducted if the conservative medical management fails. 6 The possible sequelae of Gradenigo syndrome include meningitis, dural venous sinus thrombosis, labyrinthine fistula, intracranial abscess, inflammation of skull base, facial nerve palsy, and parapharyngeal abscess. 5
We reported a patient of Gradenigo syndrome caused by suppurative otitis media which was promptly diagnosed and treated. Gradenigo syndrome is a life-threatening disease. If clinicians encounter patients with diplopia, otitis media, and retro-orbital pain, Gradenigo syndrome is an ancient but unforgettable diagnosis.
Footnotes
Authors’ Note
Written informed consent was obtained from the patient for publication and any associated images. Approval of this case study was obtained from the Institutional Review Board of Chang Gung Medical Foundation (IRB No.202001955B0).
Acknowledgments
The authors thank all of the members of Department of Otolaryngology–Head and Neck Surgery, Chang Gung Memorial Hospital, Linkou.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.