
Abstract
Isolated primary sphenoid sinusitis is a rare occurrence, estimated to make up less than 3% of sinus infections. The posterior anatomic location of the sphenoid makes treatment challenging when it becomes infected. Complications involving intracranial extension to surrounding structures often result in cranial nerve deficits due to their proximity. A single case of chronic sphenoiditis with direct extracranial extension into the prevertebral space is reported with a discussion on clinical presentation, diagnosis, and management. A 46-year-old female patient with diffuse headaches radiating into the neck and throat was evaluated in the office. Computed tomography demonstrated sphenoiditis with direct extension into the prevertebral space. Imaging revealed a purported route of direct extension through the clinoid and directly into the clivus to form an abscess in the longus colli muscle. The patient underwent endoscopic surgical management including drainage of the prevertebral abscess and has since made a full recovery. This is the first reported case of direct extension of sphenoiditis into the prevertebral space. The findings highlight the importance of aggressive treatment of chronic sphenoid infections to prevent detrimental complications. Computed tomography imaging proved an advantageous imaging modality to demonstrate bony erosion and sinus tracts from the skull base to the deep neck space.
Introduction
Inflammation of any paranasal sinus, or sinusitis, is common and affects 16% of the population. 1 On the other hand, isolated primary sphenoid sinusitis is a rare occurrence, estimated to make up less than 3% of sinus infections. 2 Acute sinusitis is generally viral, while chronic (greater than 8 weeks) is more often bacterial, though the pathogenesis is ultimately multifactorial. Infrequency of sphenoid sinus involvement is attributed to its posterior location in the sinonasal tract, which removes it from direct contamination by the environment (ie, minimal airflow). Consequently, this location also makes treatment more challenging when the sinus does become infected.
The presenting symptoms of sphenoid sinusitis are nonlocalizing and potentially misleading on physical examination. A report of isolated sphenoiditis by Ruoppi et al documented vertex headache as the most common complaint followed by rhinitis, dizziness, eye symptoms from cranial nerve involvement, and fever. 3 These symptoms are best explained by the sinus’s critical anatomic location near the skull base and orbital apex. More significant complications such as cavernous sinus thrombosis and intracranial extension of sphenoid sinusitis are extremely rare but have been documented. 4,5 Moreover, Ruoppi et al reported that 21% of isolated sphenoiditis cases experience cranial nerve deficits. 3
Although sphenoiditis with involvement of these surrounding structures has been documented, no reports have identified direct extension of primary sphenoiditis into the deep neck spaces. Once breached, the deep neck planes are intricately connected, which allows infection to spread rapidly from space to space. In general, extension into deep neck spaces is more common with otologic and pharyngeal infections that extend into retropharyngeal spaces. 6
We report a case of sphenoiditis with extracranial extension, resulting in prevertebral abscess development. In this report, we discuss clinical presentation, diagnosis, management, and postulated mechanisms of extracranial extension of sphenoiditis into the prevertebral space.
Methods
This study was approved by the institutional review board of Rush University Medical Center. A single case of direct extension of sphenoiditis into the deep neck prevertebral space was reviewed. The clinical, diagnostic, and treatment details were collected through chart review to outline the treatment regimen and response. The patient underwent endoscopic sinus surgery with frameless stereotactic computer-assisted surgical navigation. Complete right ethmoidectomy, right maxillary sinusotomy, right frontal sinusotomy, right sphenoidotomy, and incision and drainage of prevertebral abscess were performed. Prior to surgery, there was concern that a possible dermoid cyst existed posteriorly; thus special attention was paid to biopsies of this area.
Case Presentation
A 46-year-old female with a history of chronic rhinosinusitis and a 5-year history of diffuse headaches presented to the head and neck surgery clinic for progression of pain into her neck and throat. She was scheduled for surgery by a local otolaryngologist but was referred to our facility due to bone erosion of the sphenoid and clinoid seen on computed tomography (CT) scan. Review of systems was positive for eye pressure, headache, nasal congestion, and purulent discharge. Physical examination was unremarkable with normal nasal and ear anatomy, no palpable neck masses, and intact neurological examination without cranial neuropathies.
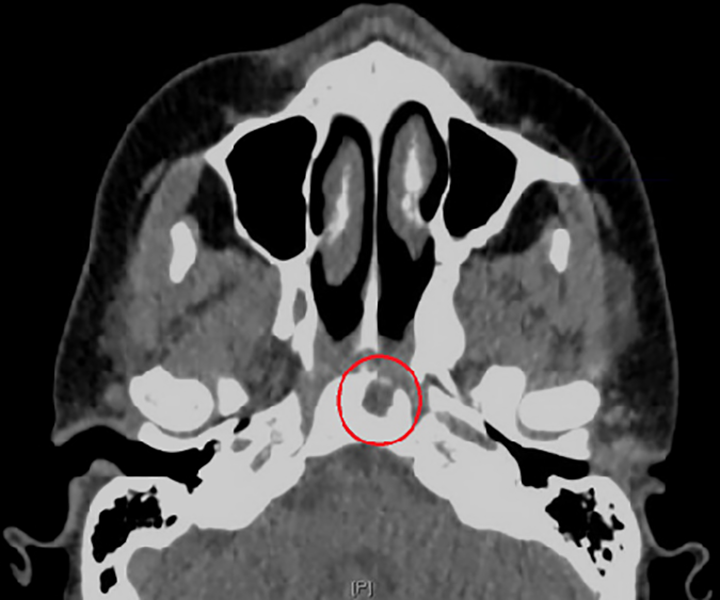
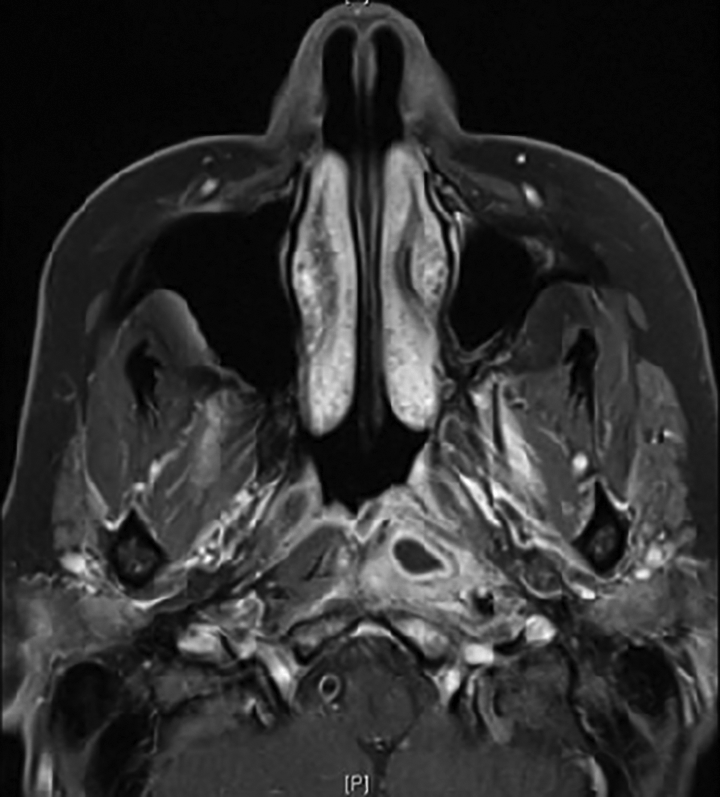
Nasal endoscopy, CT, and magnetic resonance imaging (MRI) and angiography were consistent with right sphenoiditis and left prevertebral abscess. Specifically, thin CT imaging revealed soft tissue opacification with sclerosis of the basisphenoid, lesser wing of the sphenoid, greater wing of the sphenoid, and pterygoid recess on the right side (Figure 1). The opacified soft tissue component extended into the upper clivus with an anteroinferior, well-circumscribed soft tissue mass without obvious bony invasion (Figure 2).

Erosion through the right posterior wall of sphenoid.
Erosion into clivus as infection moves posteriorly and crosses midline.
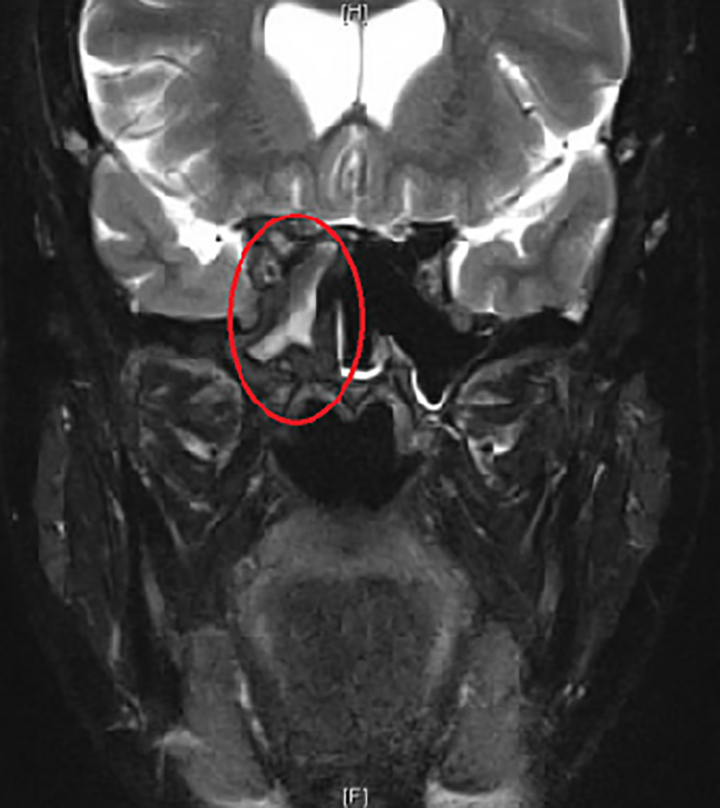
Magnetic resonance imaging redemonstrated the CT findings of an inflammatory tract extending from the posterior right sphenoid (Figure 1) into the clivus with adjacent dural enhancement inferiorly (Figure 2). The tract extended to the left prevertebral space with abnormal enhancement and edema reflecting myositis of the left longus colli muscle (Figure 3). The collection was confined to the prevertebral space without retropharyngeal space extension. A rim-enhancing abscess was embedded within the inflamed left longus colli muscle. An additional tract extended to the right vidian canal and two others formed opacified pneumatized areas of the right anterior clinoid process and superior to the foramen rotundum within the right greater wing of the sphenoid (Figure 4).
Abscess formation in the left longus colli muscle in the prevertebral space.
Anterior clinoid tract of infection.
Due to chronicity of symptoms and previously failed medical treatment of oral levofloxacin for 2 weeks, she was deemed an appropriate candidate for surgical intervention. She underwent endoscopic sinus surgery, and the deep neck prevertebral space abscess was evacuated transorally (Figure 5). No cerebrospinal (CSF) leak was noted. She tolerated the procedure well. She completed oral amoxicillin–clavulanate and prednisone postoperatively. Irrigation with budesonide and saline successfully maintained patent sinuses at 8-month follow-up without recurrence of disease.
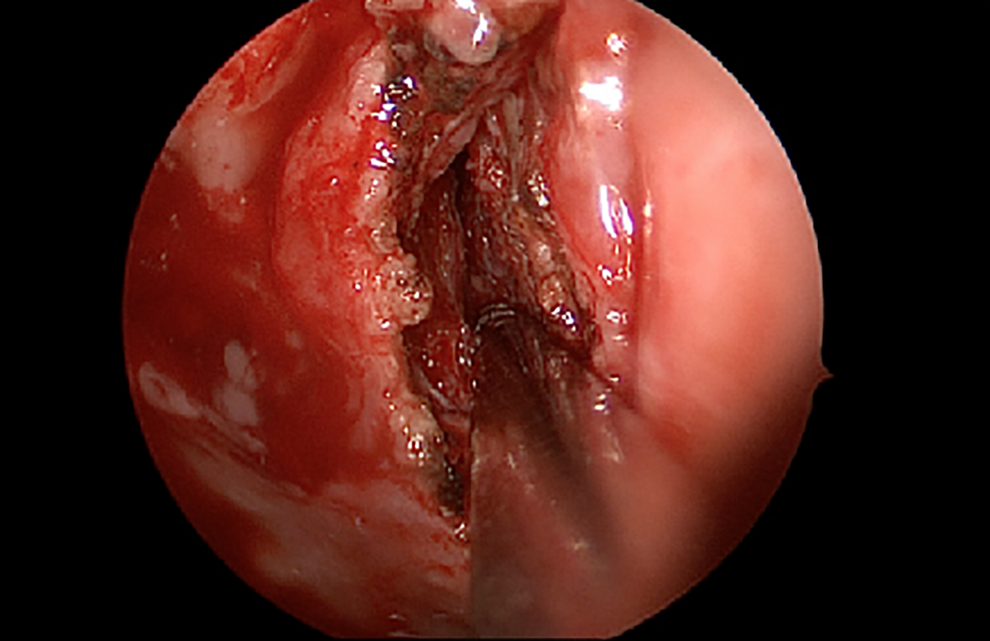
Left nasopharynx abscess cavity after incision and drainage.
Discussion
The broad differential for opacification of the sphenoid sinus includes inflammatory lesions (eg, sinusitis), neoplasms, and benign cysts. Most commonly, sphenoiditis is the result of the extension of posterior ethmoid inflammatory disease. When the other sinuses remain unaffected, an isolated sphenoiditis is diagnosed. Such a diagnosis is increasing in incidence due to increased utilization of head and neck imaging by CT and MRI as an adjunct to the workup of sinusitis.
Inflammatory lesions are the most prevalent, as opposed to neoplasms which rarely arise from the sphenoid sinus and are more likely due to invasion from a surrounding structure in the skull base. Of note, over half of neoplastic lesions diagnosed in sphenoiditis were malignant in a meta-analysis by Ng and Sethi. 7 The study further suggests that 50.3% of isolated sphenoiditis cases are inflammatory, 20.2% are mucoceles, with the rest consisting of CSF leaks or encephaloceles, fibrous dysplasia, inverted papillomas, and malignant lesions. 7
Deep neck infections involving the potential spaces (retropharyngeal, danger, prevertebral) are not classically associated with sphenoiditis. Each space has unique risks of infection based on the age of the patient and the source of primary infection. Deep neck infections are more common in children than adults. Adult involvement is usually secondary to local trauma, such as pharyngeal perforation, laryngoscopy, endotracheal intubation, or feeding tube placement. As can be expected, the most common bacteria are aerobic Gram-positive cocci or anaerobic (bacteroides, fusobacterium, peptostreptococcus) prone to forming abscesses, with many cases being polymicrobial. 8
An understanding of the deep neck spaces is critical to the analysis of the unique sphenoiditis complication being presented here. These fascial planes create potential deep neck spaces that serve as conduits for rapid infection spread. Moving from anterior to posterior, the retropharyngeal space is encountered immediately behind the pharynx, followed by the danger space, and most posteriorly is the prevertebral space. The 3 spaces are separated by the alar and prevertebral fascia from anterior to posterior, respectively. The abscess encountered in this case developed in the prevertebral space involving the longus colli muscle.
Prevertebral infection microbiology is variable depending on the source of infection; thus, broad empiric coverage is necessary until culture susceptibilities are available. 9 Mycobacterial prevertebral involvement has rarely been documented as the first presenting sign of a pulmonary tuberculosis infection. 10 Intravenous drug use, alcoholism, immunosuppression, and diabetes are known risk factors for prevertebral abscesses. Hematogenous spread or contiguous extension from vertebral osteomyelitis are additional known common primary sources. 11 Infections of this space are concerning for psoas abscesses, since the prevertebral fascia connects directly with the psoas sheath within the abdominal cavity to provide a path for distant seeding of infection. 12 Prevertebral abscesses are difficult to diagnose with fewer than 75% of patients complaining of neck or back pain, although some may present with neurologic deficits localizing to affected nerve roots. 13 In the case of the current case, neck pain was a presenting complaint, but no neurologic deficits were noted.
The extension of deep neck infection from the skull base appears to be undocumented in the literature. The case of sphenoiditis with direct extension into the prevertebral space, involving the longus colli muscle, has not been reported. Figures 1 to 5 demonstrate 3 routes of infection spread posterior to the sphenoid, into the opticocarotid recess, and inferior to the clivus.
Extension into surrounding structures is a well-known and feared complication of sinusitis. The most dreaded extension is into the brain, which is more likely when the posterior sinuses are involved. The frontal sinus can easily spread posteriorly into the brain by eroding through the posterior table. Ethmoiditis can spread into the orbit by eroding laterally. These complications are analogous to this report of sphenoiditis extending posteriorly through bone and moving caudally from the clivus, though orbital and intracranial complications are much more common.
The prevertebral fascia connects most superiorly at the base of the clivus and most inferiorly at the tip of the coccyx. Thus, erosion through the sphenoid, into the clivus, and down into the prevertebral space is anatomically plausible. Previous reports of sphenoid lesions extending through natural spaces also suggest that an anomalous path of least resistance may have existed. Tumors have been reported to follow canals into the skull base, such as nasopharyngeal carcinoma following the foramen lacerum in extension. 14
The appropriate workup of sinusitis with suspected posterior extension requires imaging of head and neck for abscesses. As noted previously, over 75% of prevertebral abscesses do not complain of neck or back pain. 13 Computed tomography with contrast is the gold standard for deep neck infections and may demonstrate rim enhancement of the abscess and can additionally highlight mucosal and bony paranasal sinus inflammation while defining bony erosion. Magnetic resonance imaging is helpful for soft tissue definition and distinguishing postobstructive mucus from intrasinus masses.
Endoscopic sinus surgery was the treatment of choice for this case. Endoscopic sinus surgery is indicated for any isolated sphenoiditis with symptoms of progression or nerve involvement. 15 Thus, endoscopy was indicated regardless of deep neck abscess presence. Endoscopy provided adequate view of the abscess location in the nasopharynx and allowed for appropriate drainage and exploration (Figure 5).
Conclusion
To our knowledge, this is the first reported case of sphenoiditis with direct extension into the prevertebral deep neck space. Although this route of extension is not common, this report highlights the importance of understanding that clival erosion can offer a low resistance path into a deep neck potential space. Intracranial extension is often a feared complication of sphenoiditis, but extracranial extension can occur, and symptoms should not be overlooked. This case also reports that endoscopic access to the prevertebral space has been proven a successful method of abscess treatment, as seen in this example. At this point, this is the first reported case that highlights the diagnosis and management of sphenoiditis with direct extracranial extension. Given the rarity of this presentation, management should be tailored on a case-by-case basis with consideration of extension route and location of the deep neck abscess along the length of the spine.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.