
Abstract
Olfactory neuroblastoma (ONB) is an ectodermal malignant tumor originating from the olfactory nerve epithelium of the nasal cavity and paranasal sinus. Olfactory neuroblastoma is a rare cancer, with an estimated incidence of 0.4 per million. Olfactory neuroblastoma often occurs in the top of the nasal cavity or near the lateral wall of the middle turbinate, which accounts for approximately 3% to 5% of the nasal cavity and paranasal sinus tumors. Olfactory neuroblastoma primarily in the nasopharynx is rare and tends to be misdiagnosed as nasopharyngeal carcinoma. Herein, we presented a case of ONB of the nasopharynx with recurrent nasopharyngeal tumor and by lymph node metastasis in both sides of the neck 14 months after surgical removal of the primary ONB. Long-term disease-free survival was achieved by definitive radiotherapy. Surgery combined with radiotherapy or definitive radiotherapy is recommended for primary ONB of the nasopharynx, radiotherapy target delineation including nasopharynx and pharyngeal lymph nodes, and neck lymph node drainage area of level Ib, Ⅱ, and Ⅲ.
Introduction
Olfactory neuroblastoma (ONB) also known as sensory neuroblastoma is a malignant tumor of neuroectoderm originating from the olfactory epithelium of the nasal cavity and paranasal sinus. Olfactory neuroblastoma is a rare cancer with an estimated incidence of 0.4 per million. There is no gender specific for ONB cases. Majorities of patients are diagnosed as having ONB in their fifth and sixth decades of life, and few patients develop ONB at an age of <20 years. 1 Olfactory neuroblastoma usually occurs at the top of the nasal cavity or near the lateral wall of the middle turbinate, accounting for approximately 3% to 5% of the tumors in the nasal cavity and paranasal sinus.2,3 It has been reported that ONB occurred in the regions such as maxillary sinus and sphenoid sinus, 4 but olfactory neuroblastoma primary in the nasopharynx is rare. Herein, we reported a case of nasopharyngeal olfactory neuroblastoma.
Case Presentation
The patient was a 55-year-old Chinese male admitted to the Shaoxing Hospital of Zhejiang University on September 20, 2010, due to nosebleed with pharyngeal pain for 5 days. During a nasal endoscopy, dark red mass with smooth surface was observed in the left nasopharyngeal cavity and behind the soft palate (Figure 1A and B). The computed tomography (CT) examination found a 3.7 cm × 2.1 cm soft tissue mass in the left nasopharyngeal cavity, involving the compression of the left oropharynx recess and pharyngeal orifice of the Eustachian tube. The enhanced scan showed uneven enhancement: The boundary between the mass and surrounding structures was clear, but the left pharyngeal saphenous cavity and the pharyngeal opening of the Eustachian tube were compressed (Figure 1C). Nasopharyngeal mass resection was performed under the endoscopy on September 24, 2010. During the operation, approximately 4.0 cm × 5.0 cm neoplasm with the base in the left round pillow of the nasopharyngeal cavity was removed. Postoperative pathological report confirmed that it was an olfactory nerve tumor (Hyams level IV; Figure 2A). The results of immunohistochemical staining were as follows: NSE(+), P53(+), Ki-67(+), CK(+), EMA(+), Ki-67(80%+), HMB45(−), S-100(−), Syn(−), CgA(−), CD3(−), CD45Ro(+), CD20(−), CD79a(−), 34βE12(+) focally, CD99(−), and HMB45(−). The patient did not receive any treatment after surgical removal of the tumor. The patient then developed nasal obstruction 14 months postoperation. On December 7, 2011, outpatient examination revealed another mass in the left nasopharynx. Magnetic resonance imaging of the nasopharynx revealed mass in the nasopharynx and left ethmoid sinus. Multiple nodular soft tissue signal foci were found in the left parapharyngeal space and bilateral carotid sheath (level II and III), with obvious enhancement (Figure 3A and B). Pathological report of nasopharyngeal mass biopsy confirmed the recurrence of olfactory neuroblastoma (Figure 2C). It was diagnosed as recurrent nasopharyngeal olunga neuroblastoma with double cervical lymph node metastasis. On December 20, 2011, intensity-modulated radiation therapy (IMRT) was performed, for 30 fractions per 6 weeks, and then followed by 5 fractions per week. Planned target volume for nasopharyngeal tumors (GTV-P) was prescribed to 70 Gy, and planned target volume of involved cervical lymph nodes (GTV-N) was 66 Gy. The doses delivered to the clinical target volume 1 (CTV-1, high risk) and CTV-2 (low risk) were 66 and 54 Gy, respectively. In addition, the patient did not receive chemotherapy. Endoscopic reexamination and magnetic resonance examination after radiotherapy showed complete remission of the tumors in nasopharynx and neck (Figure 3C and D). No tumor recurrence or metastasis was found during the follow-up of >8 years.
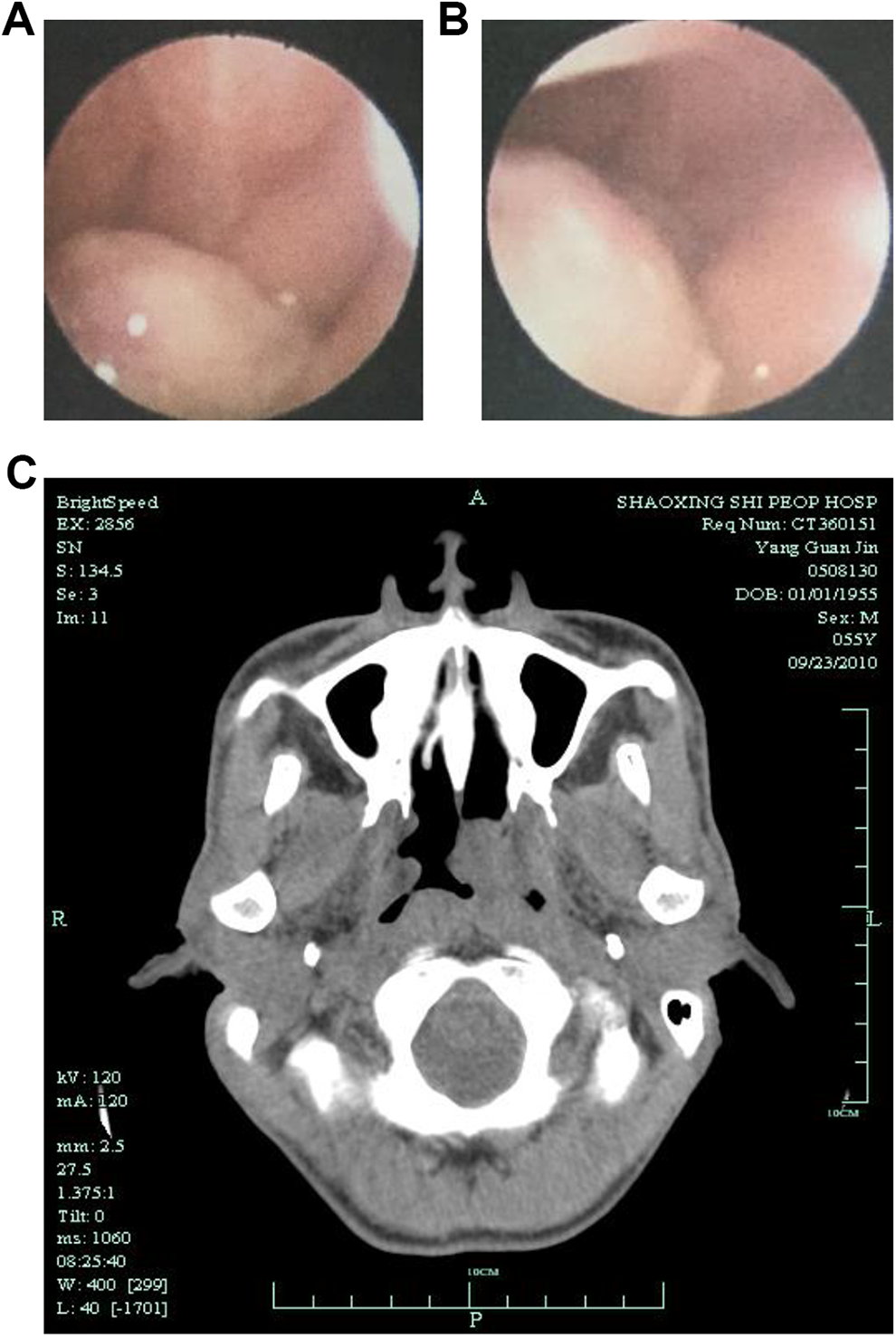
Dynamic laryngoscope and nasal endoscopy indicated a nasopharynx neoplasm (A and B). Computed tomography showed soft tissue mass in the left nasopharynx cavity (C).
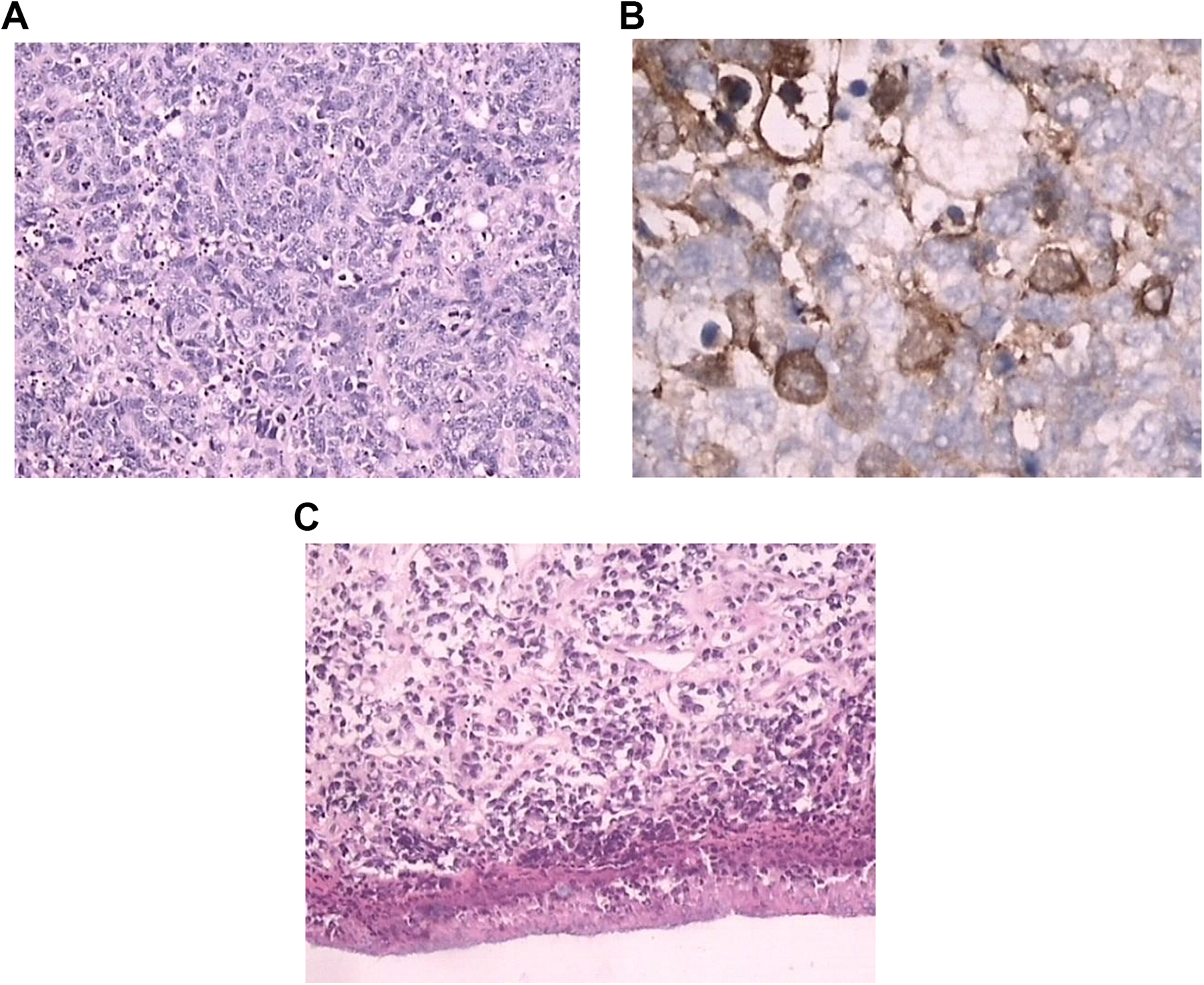
Postoperative pathological description: tumor cells were separated into nest-like structures by fibrovascular stroma. Tumor cells were of the same size (medium to small), with few cytoplasm, round nuclei, fine chromatin, and unclear nuclear membrane (A ×20). Neuron-specific enolase staining showed that the cytoplasm and membrane of tumor cells were stained with brown granules (B ×40). Pathology for recurrent tumor: tumor cells invaded nasopharyngeal mucosa and ulcerated. Tumor cells were separated by abundant fibrous vascular stroma and distributed in scattered and small nests (C ×20).
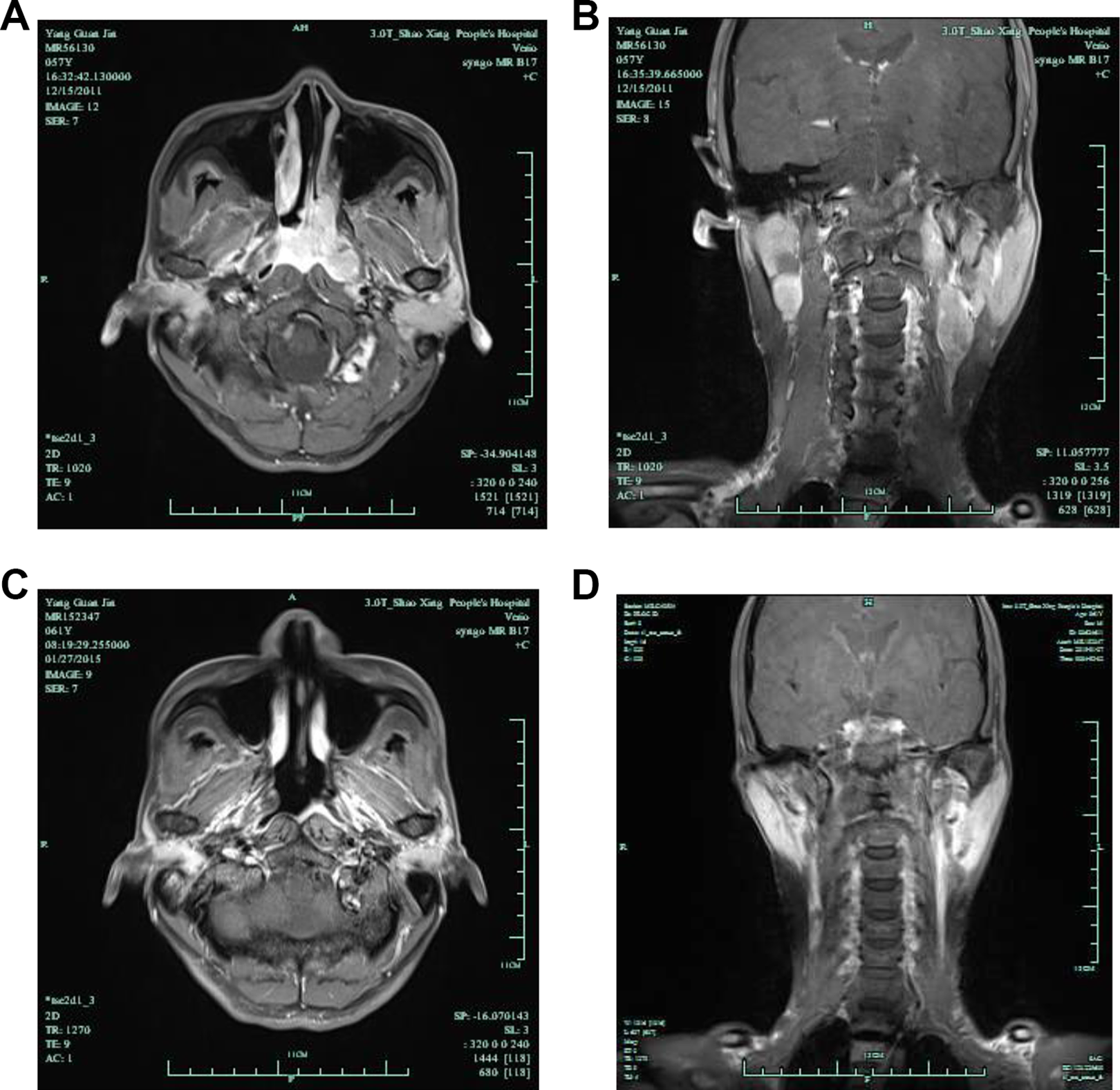
Magnetic resonance imaging of the nasopharynx: mass in nasopharynx and left ethmoid sinus, and multiple enhanced lymph node lesions in the left parapharyngeal space and bilateral carotid sheath area (A and B). Nasopharyngeal tumor and cervical lymph node metastasis disappeared after radiotherapy (C and D).
Discussion
Olfactory neuroblastoma is a rare malignant tumor of the nasal cavity, paranasal sinus, and anterior skull base. Olfactory neuroblastoma is generally considered as a neuroectodermal tumor originating from basal cells of the epithelial cells of the olfactory nerve. 5 It has been suggested that ectopic ONB may be derived from ectopic dormant cells located in the sinus, Jacobsen’s vomeronasal organ, persistent terminal ganglion cells, or sympathetic/parasympathetic autonomic ganglion. 4
The primary site of ONB may be difficult to identify. The common symptoms include unilateral nasal congestion, bloody nose, head and face pain, anosmia, and so on. Olfactory neuroblastoma can invade paranasal sinuses and paranasal sinuses and break through the ethmoid plate to invade the anterior fossa, causing lacrimal overflow, diplopia, exophthalmia and vision loss, frontal lobe compression symptoms, or seizures.4,5 Olfactory neuroblastoma is typically manifested as soft tissue mass at the top of the nasal cavity and ethmoid sinus, with rare necrosis, and linear, floral ring moderate or obvious enhancement on enhanced CT scan. 6 Magnetic resonance imaging is superior to CT in evaluating the degree of involvement of tumor soft tissue. 7 Primary nasopharyngeal ONB is rare. The clinical symptoms and imaging findings of this nasopharyngeal ONB case we reported were very similar to nasopharyngeal carcinoma, that is, CT showed left nasopharyngeal cavity lump, involving the left oropharyngeal, uneven reinforcement of enhanced scanning, which was likely to be misdiagnosed as nasopharyngeal carcinoma. Therefore, the diagnosis still depends on histopathological and immunohistochemical examination.
Classically, ONB is composed of small round cells with a nest or patch-like nerve fiber matrix arranged with chromatin dots and having Flexner-Wintersteiner and Homer Wright rosettes.7,8 It is important to differentiate ONB from small-cell carcinoma, lymphoma, rhabdomyosarcoma, undifferentiated carcinoma, and even melanoma by immunohistochemical examination. 9 Immunohistochemical markers, such as neuron-specific enolase, synaptophysin, pheochromochrome A (CgA) and CD56, were positively expressed in ONB tumor cells. 7 The cellular proliferation measured by Ki-67 staining was associated with tumor grade. 5 Hymas pathological grade is an important prognostic factor. The 5-year survival rate of grade I-II (low-grade) ONB is 56% to 80%, significantly higher than that of grade III-IV (high-grade) patients (25%-40%). This case had grade IV tumor according to Hymas histologic grading system. Although the morphology of pathological grade IV ONB is similar to Ewing’s sarcoma (EWS) or primary neuroectodermal tumor, it lacks specific EWS-FLI1 fusion gene. 10
The Kadish stage is most widely used in clinics: stage A, the lesion confined to the nasal cavity; stage B, the lesion located in the nasal sinus; stage C, the lesion extends beyond confines of nose locally to include the skull base, intracranial compartment, or orbit; stage D, distant disease, either to regional lymph nodes or distant metastasis. 11 Kadish staging is an independent prognostic factor for ONB.
Surgery combined with radiotherapy is the best treatment for ONB.12,13 Compared with radiotherapy alone, platinum-based etoposide regimen did not improve the survival rate of ONB, and the indication of chemotherapy and the best drug for ONB are still controversial. 14 It was reported that nasal endoscopic surgery could achieve surgical clearance, even in advanced Kadish C stage disease, with favorable outcomes to open craniofacial resections. 15 Radiotherapy can improve prognosis as well. If it is difficult to obtain a reliable negative surgical margin, postoperative radiotherapy should be performed, 16 with a dose of 50 to 60 Gy.8,15 For Kadish A/B patients, radical radiotherapy achieves similar survival benefits as a treatment combined surgery with radiotherapy, and thus the optional treatment. For Kadish Stage C patients with negative lymph nodes, the combination of surgery and radiotherapy improves survival and patients who receive preoperative radiotherapy have the most favorable prognosis. 13 Due to the rarity of ONB, there has been no study comparing the efficacy of preoperative and postoperative radiotherapy.
The most common failure mode after ONB treatment is local recurrence, with a recurrence rate of about 14% to 30%.2,17 Surgery combined with postoperative radiotherapy can reduce the local recurrence rate to around 15%. 12 The incidence of cervical lymph node metastasis was as high as 30% in recurrent metastasis. 18 The involvement is common for level II and Ib lymph nodes, followed by level III and retropharyngeal lymph nodes. Patients with cervical lymph node involvement were prone to distant metastasis. Multivariate analysis showed that the prophylactic elective neck irradiation was a favorable predictor for regional control, and the regional failure significantly decreased from 23% to 2% for node-negative ONB. 3 In this case, the patient presented nasopharyngeal tumor recurrence and cervical lymph node metastasis 14 months after surgical treatment, possibly due to the absence of postoperative radiotherapy. After radical IMRT for the nasopharyngeal tumor and lymph node metastases in both sides of the neck, the tumor was completely remitted. The patient was free of disease for more than 8 years, suggesting that the radiation dose of 66 to 70 Gy provided an effective control of tumor growth.
Conclusion
Surgery combined with radiotherapy or definitive radiotherapy is recommended for primary ONB of the nasopharynx, radiotherapy target delineation including nasopharynx and pharyngeal lymph nodes, and neck lymph node drainage area of level Ib, Ⅱ, and Ⅲ.
Footnotes
Authors’ Note
Wangyan Zhong and Cheng Wang contributed equally to this work.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.