
Abstract
Ectopic olfactory neuroblastoma (ONB) is a rare neuroendocrine sinonasal malignancy which arises from sinonasal regions where olfactory neuroepithelium does not exist. Presentation of syndrome of inappropriate antidiuretic hormone release (SIADH) in patients with ectopic ONB is extremely rare. We report a case of a 22-year-old patient with ectopic ONB and paraneoplastic SIADH that was managed at our center. The ONB was arising from the left lamina papyracea and extending into the maxillary and ethmoid sinuses and filling the nasal cavity. Correction of sodium levels occurred within 24 hours of endoscopic resection via a combined trans-nasal transorbital approach. To avoid negative sequela secondary to rapid sodium correction, the patient was managed by desmopressin to obtain gradual sodium correction, which was achieved on the fourth postoperative day. Ectopic presentation of ONB with paraneoplastic SIADH is extremely rare with only 7 cases reported in the literature to date. Management via surgical resection and/or radiotherapy for these patients requires the managing clinician to be vigilant of serum sodium levels. A multidisciplinary approach is essential for optimal outcomes.
Background
Olfactory neuroblastoma (ONB), also known as esthesioneuroblastoma, is a sinonasal neuroendocrine malignancy first described in 1924. It has a low prevalence and accounts for 3% of all sinonasal tumors with a yearly incidence of approximately 0.4 per million people.1,2 It affects males and females equally and can occur at any age, although it more commonly presents in the second or sixth decades of life. 1 ONB is associated with nonspecific symptoms such as unilateral nasal obstruction, epistaxis, headache, pain, paresthesia, nausea, and cervical lymphadenopathy. Due to the possibility of asymptomatic early-stage disease and nonspecific symptoms at presentation, diagnosis can be delayed, resulting in a more advanced stage at diagnosis. 3
In addition to the symptoms associated with direct tumor invasion and metastasis, ONB can present with symptoms related to a paraneoplastic syndrome. 4 One of the paraneoplastic endocrine syndromes is the syndrome of inappropriate antidiuretic hormone secretion (SIADH). It presents as hyponatremia and hyposmolality in a clinically euvolemic patient with urine osmolality greater than 100 mOsm/kg and urine sodium concentration greater than 40 mmol/L in the absence of other causes of hyponatremia.5,6
ONB is found in areas with olfactory neuroepithelium and classically presents as a mass in the olfactory cleft and upper nasal cavity that can extend to the ethmoid sinuses, anterior skull base, and orbit. 7 Ectopic ONB is a rare presentation of ONB arising from sinonasal regions where olfactory neuroepithelium does not usually exist. 7 Presentation of SIADH in patients with ectopic ONB is extremely rare and only 7 cases have been reported to date.7 -12 Here we report a rare case of ectopic ONB with paraneoplastic SIADH and review the existing literature on similar reported cases of ectopic ONB with paraneoplastic SIADH.
Case Details
A 22-year-old woman presented with a 6-month history of left nasal obstruction and congestion, as well as left-sided epiphora. She denied epistaxis, hyposmia, fatigue, and weakness, while never having had her electrolytes checked previously. A complete head and neck physical examination revealed a left-sided vascular nasal mass that was reaching the nasal sill with a completely intact right nasal cavity. A contrast sinus computed tomography (CT) scan revealed an enhancing mass arising from the left lamina papyracea and extending into the maxillary and ethmoid sinuses and filling the nasal cavity (Figure 1). An infused MRI also showed an enhancing left-sided nasal mass invading the orbital fat with sparing of the medial rectus muscle (Figure 2).
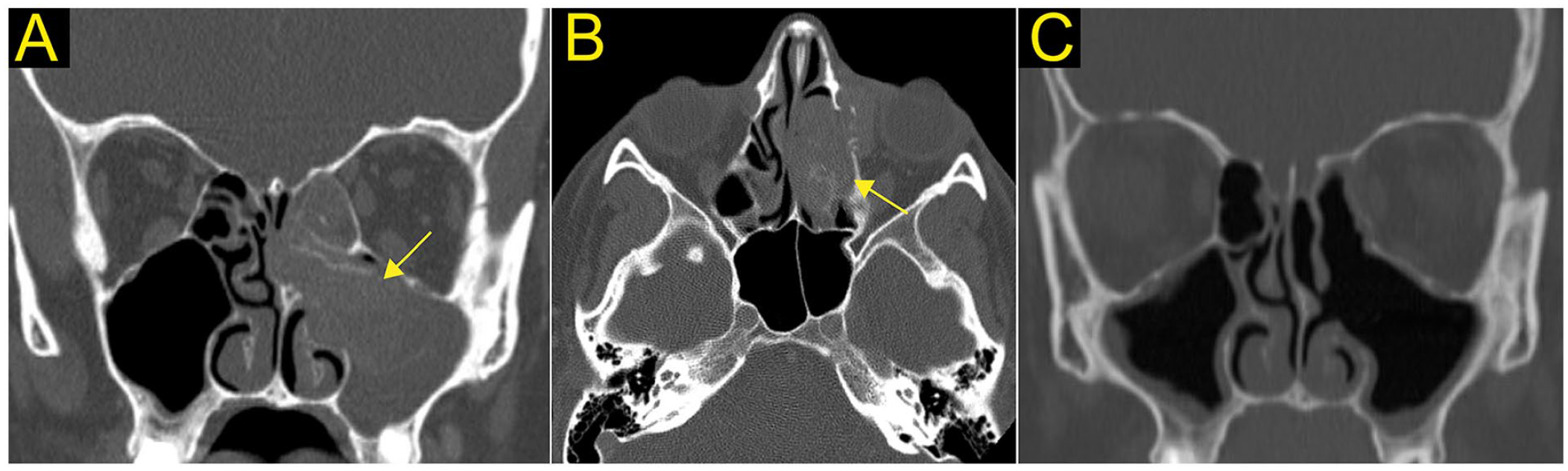
CT imaging of the sinuses in a 22-year-old female with ectopic olfactory neuroblastoma. Preoperative imaging in the coronal (A) and axial (B) view indicate a vascular soft tissue mass centered in left maxillary antrum (yellow arrow), with subsequent local middle turbinate and ethmoid bone remodeling. Successful tumor resection was confirmed on postoperative CT of the sinuses in the coronal section (C).
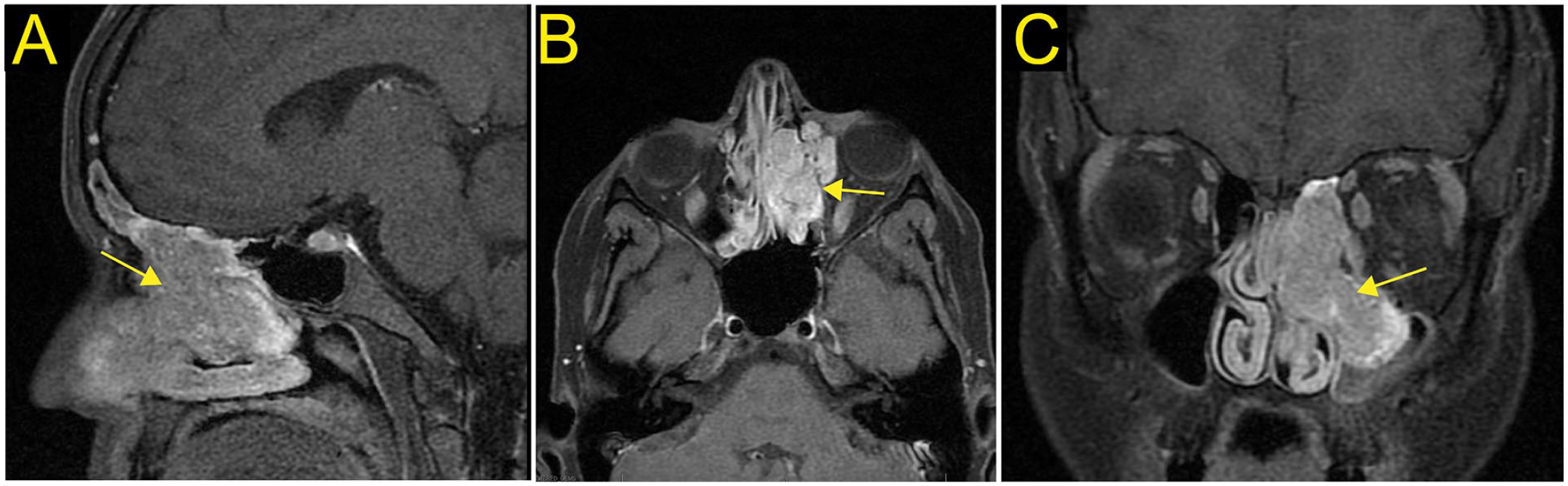
T1-weighted MRI with contrast of the sinuses in a 22-year-old female with ectopic olfactory neuroblastoma in the sagittal (A), axial (B), and coronal (C) sections. There is a large enhancing left nasal passage tumor (yellow arrow) with extension through lamina papyracea to the medial and inferior aspect of the left orbit and through the left frontoethmoidal recess into the left maxillary antrum. There is mild deviation of the nasal septum secondary to localized mass effect. There is no enhancement to suggest extension through the cribriform plate.
An in-office biopsy under local anesthesia was performed. Histopathology showed a small round blue cell tumor with lobules of low-grade monotonous cells with high nuclear-cytoplasmic ratios, round nuclei, and relatively homogenous/stippled chromatin among a fibrillary matrix. Homer Wright pseudorosettes, a characteristic finding of olfactory neuroblastomas, are seen. The tumor cells were positive for synaptophysin, and S100 highlights sustentacular cells on immunohistochemical stain. The cells were negative for cytokeratin. No significant nuclear pleomorphism, necrosis, or mitoses are seen. Overall, the findings were that of an olfactory neuroblastoma, Hyams grade 1. CT of the chest, abdomen, and pelvis indicated no evidence of distant metastasis.
Secondary to our previous experience with electrolyte imbalances that can accompany ectopic ONBs, a plasma sodium level was ordered. Despite the patient not showing any symptoms of hyponatremia preoperatively, her plasma sodium level was measured to be 117 mmol/L (normal is 135-145 mmol/L).
The patient subsequently underwent endoscopic image-guided sinus surgery using a combined trans-nasal, transorbital approach with complete excision of the nasal and orbital components of the mass with negative margins (Figure 3). The tumor was found to be arising from the lamina papyracea. Histopathology confirmed the diagnosis found at biopsy of a Hyams grade 1 ONB with no lympho-vascular invasion (Figure 4).
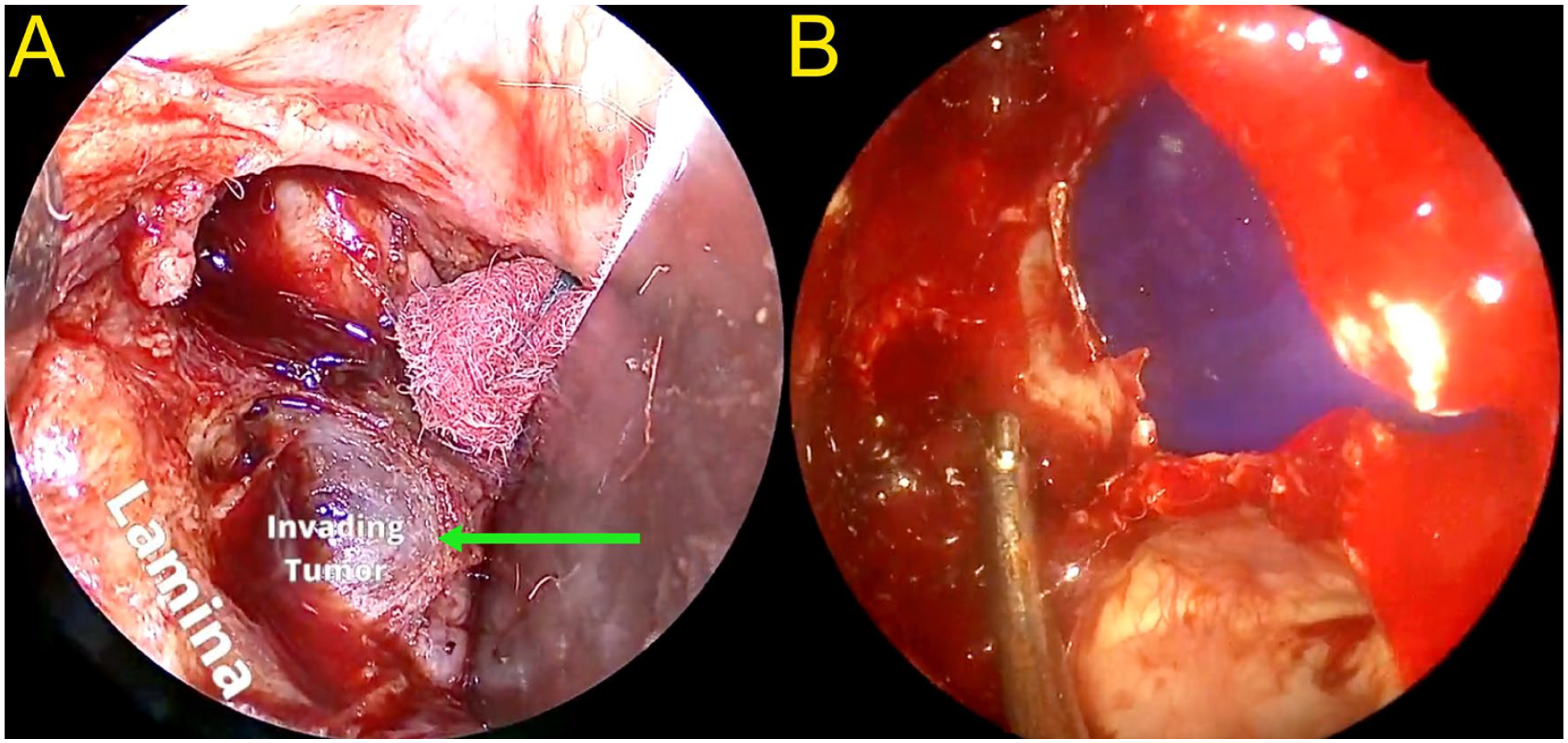
Transorbital view of the tumor (green arrow) extending into the orbit without direct invasion into the periorbita or medial rectus muscle (A) and endoscopic view of the reconstructed lamina papyracea using polydioxanone (PDS) plate (B).
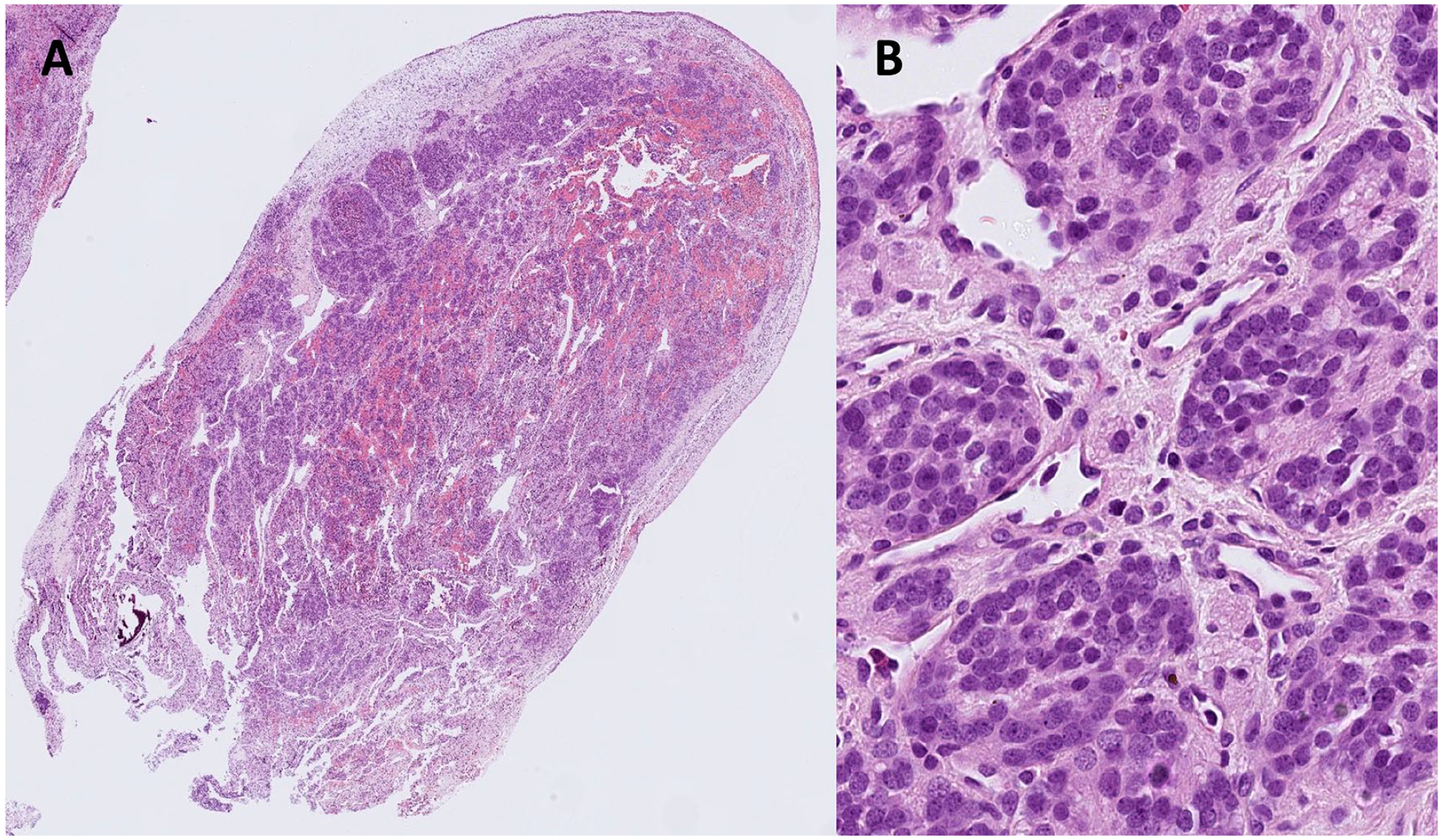
Sections of the left nasal mass from a 22-year-old female patient show a small round blue cell tumor infiltrating a squamous lined polypoid tissue with a fibrillary matrix and pseudorosette formation (A, 20x magnification, Hematoxylin & Eosin). The findings are that of a Hyams grade 1 olfactory neuroblastoma. High magnification shows the stippled chromatin of the nuclei (B, 400x magnification, Hematoxylin & Eosin).
Postoperatively, the patient had a rapid correction of her plasma sodium to 144 mmol/L after 24 hours. To avoid negative sequela secondary to this rapid sodium correction, the medical and endocrinology team continued managing the patient’s sodium level using desmopressin (DDAVP, 6 µg intravenous every 4 hours initially, then 2 µg subcutaneous once a day), which was finally normalized on the fourth postoperative day. From a surgical perspective, the patient tolerated oral intake easily with no diplopia or changes in vision. The patient finished radiotherapy and has remained disease free ever since.
Discussion
Olfactory neuroblastomas are extremely rare tumors, and primary ectopic ONBs are even less prevalent. Considering their malignant nature and the possibility of metastasis, early diagnosis and treatment can greatly improve patient outcomes. It is estimated that it takes on average 6 months from the onset of symptoms to properly diagnose ONBs. 13 Late recognition and diagnosis of ONBs is primarily due to the rareness of this malignancy and the nonspecific symptoms at presentation, often secondary to tumor mass effect. When ectopically located, the mass effect of ONBs can differ depending on the location of the tumor, further complicating the symptoms at presentation. In rare instances, ONBs can remain asymptomatic or present with symptoms associated with a paraneoplastic syndrome, the most common being SIADH. 4
In addition to the patient discussed here, literature review of all studies between the year 2000 and June of 2022 revealed 7 other cases of ectopic ONBs with SIADH that have been reported in the literature (Table 1). In 4 of these reported cases, the patients were asymptomatic from an otolaryngological perspective and presented with symptoms secondary to hyponatremia, such as neurocognitive disturbances, nausea, vomiting, and lethargy.7,10 -12 In the remaining 2 cases, the ONB lesions were located in the sellar region and were causing visual disturbances, including progressive binocular visual loss 8 and left temporal hemianopsia. 9
Literature Review of Ectopic Olfactory Neuroblastoma and Syndrome of Inappropriate Antidiuretic Hormone Secretion.
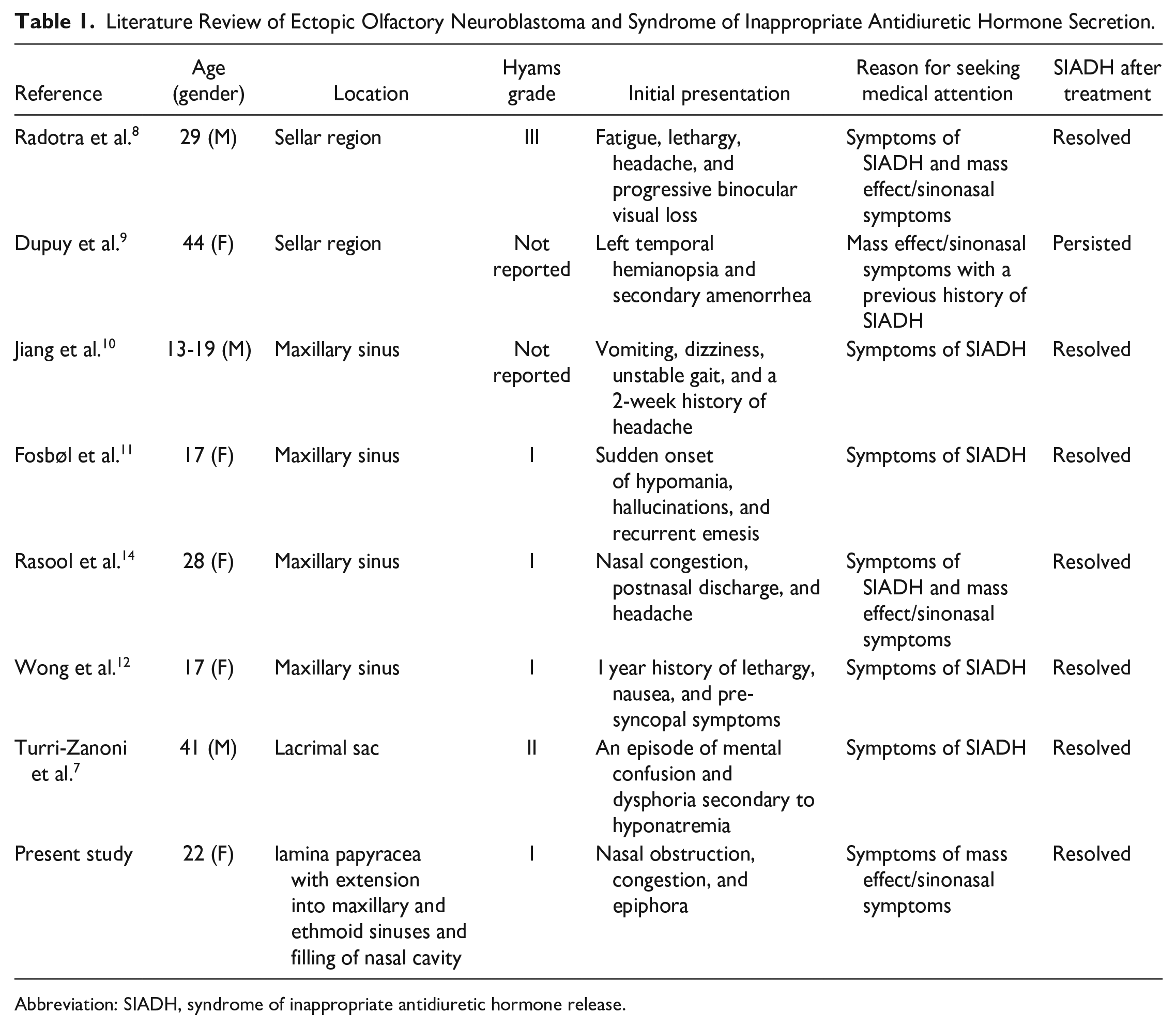
Abbreviation: SIADH, syndrome of inappropriate antidiuretic hormone release.
Ectopic ONB isolated to the maxillary sinus with SIADH has been reported in 4 patients.10 -12,14 Isolated sellar region involvement has been reported in only 2 cases.8,9 The remaining 2 cases of ectopic ONB with SIADH include a patient with lacrimal sac involvement, 7 and lastly, the patient included here has ONB originating from the lamina papyracea and involving the nasal cavity, maxillary sinus, and ethmoid sinuses with extension into the orbital fat.
Given the rare occurrence of ONB, clear management guidelines are not well established. Common approaches to the treatment of ONB include surgical resection in addition to radiotherapy, although Villano et al. 15 reported that adjuvant radiation does not increase survival when compared to surgical resection alone. The role of chemotherapy in the treatment of ONB is controversial. Induction chemotherapy in cases of poorly differentiated ONB (Hyams grade III or IV), or systemic treatment with chemotherapy in metastatic disease or unresectable ONB tumors, may provide benefits.5,16 Although the data on treatment strategies are often based on cases of ONB without ectopic presentation, they are still applied to the management of primary ectopic presentations of ONB with modifications.
In cases of ectopic ONBs, further investigation of electrolyte abnormalities, specifically sodium, can allow the care team to prepare for potential rapid correction of sodium after treatment. Postsurgical correction of electrolyte abnormalities was noted in 6 cases of ectopic ONBs with SIADH7,8,10 -12 in addition to the patient in the current report, which further emphasizes the importance of a multidisciplinary approach to posttreatment care. Additionally, we recommend routine preoperative screening for hyponatremia in patients presenting with ectopic ONBs, as asymptomatic SIADH is possible, as occurred with our patient. Failure to identify asymptomatic hyponatremia could lead to life-threatening consequences such as brain edema secondary to rapid postoperative electrolyte correction.
The variation in the presenting symptoms of ectopic ONBs can be further complicated by potential paraneoplastic effects as a sequela of SIADH. For patients presenting with idiopathic SIADH, we recommend a complete otolaryngology examination in addition to a CT scan of the head to rule out malignant processes in the sinonasal cavity. A positron emission tomography scan may be useful in identifying the exact location of the ectopic ONB.
The patient presented in the current study in addition to all reported cases of ectopic ONB with SIADH, except for 1 patient, had full resolution of SIADH after tumor resection with clear margins. The only reported case with persistent SIADH posttreatment was of a 44-year-old woman with a 4-year history of SIADH who was noted to have an ectopic neuroblastoma in the sellar region. 9 Despite endoscopic resection of the tumor, small stable remnants of the disease were found in the postoperative MRI scans, indicating that eradication of SIADH is likely dependent on complete tumor resection with clear margins. Although studies with larger sample sizes are likely needed to better assess the prognosis of paraneoplastic SIADH after surgical resection of ectopic ONB, the reported cases to date suggest that the expected outcomes after surgical intervention are favorable.
Conclusions
Ectopic presentation of ONB is seldomly described in the literature and its prevalence and incidence have yet to be determined. Paraneoplastic SIADH among cases of ectopic ONB is an even rarer entity, with only 7 cases reported to our knowledge. The existing cases in the literature in addition to the patient discussed here suggest that ectopic ONB with SIADH can remain completely asymptomatic or present with signs and symptoms of hyponatremia and/or tumor mass effect. Appropriate management of patients with ONB should include a thorough preoperative investigation of serum electrolytes and a multidisciplinary approach to postoperative care to optimize patient outcomes.
Footnotes
Acknowledgements
We would like to thank Dr. Vivian Yin and her team for their help with the trans-nasal, transorbital approach, as well as all the medical personnel that aided in the management of our patient.
Availability of Data and Materials
Not applicable.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics Approval and Consent to Participate
Not applicable.
Consent for Publication
The article does not contain any individual person’s data in any form; however, the patient has consented for their case to be published.