
Abstract
Lipomas of the palatine tonsil are rare benign neoplasms in clinical practice. We present a case of palatine tonsillar fibroangiolipoma in a 50-year-old Chinese male with a history of multiple lipomas on the back and extremities. It was diagnosed based on histological examination and integrated analysis. Good wound healing and no evidence of recurrence were noted within 6 months follow-up after tonsillectomy. This article also puts a spotlight on the differential diagnosis of benign tonsillar tumors and reviewed recent relevant literature.
Introduction
Palatine tonsils, as paired immune organs, play an important role in human immune system. 1 The basal layer of tonsils consists of abundant diffuse and nodular lymphoid tissue. Neoplasms are not common in tonsils, and only about 25% of tonsillar tumors, such as hemangiomas, lipomas, and schwannomas, are benign in clinical practice. Lipomas are slow-growing mesenchymal neoplasms characterized by mature white adipocytes which are rarely seen in the normal structure of tonsils. Fibroangiolipoma is a type of lipoma and has been previously found and reported in the intra-thoracic trachea, 2 while its presence in the palatine tonsil remained extremely rare. Herein, we described a case of fibroangiolipoma in the right palatine tonsil of a Chinese male and reviewed the current relevant literature.
Case presentation
A 50-year-old Chinese man presented at the department of otorhinolaryngology-head and neck surgery of Zhongnan Hospital of Wuhan University, with the complaint of a foreign body sensation over the pharynx for 3 months. He had symptoms of alternative nasal obstruction and a slight cough. He denied pain, dysphagia, dyspnea, and changes in the character of his voice. In recent days, he had noticed a neoplasm about the right pharynx and felt anxious. Upon further questioning, the patient revealed a history of tobacco addiction for more than 20 years. Besides, he had multiple masses on the back and extremities for over 10 years and received a tumorectomy. The pathohistological examination of the specimen confirmed the diagnosis of multiple lipomas.
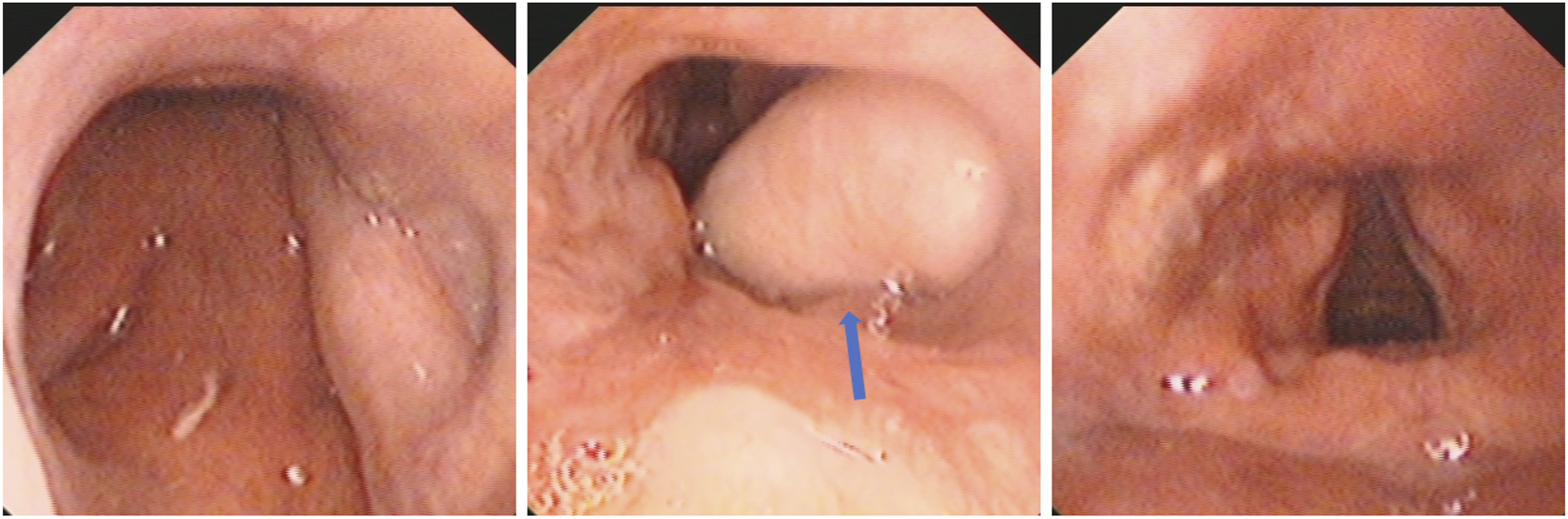
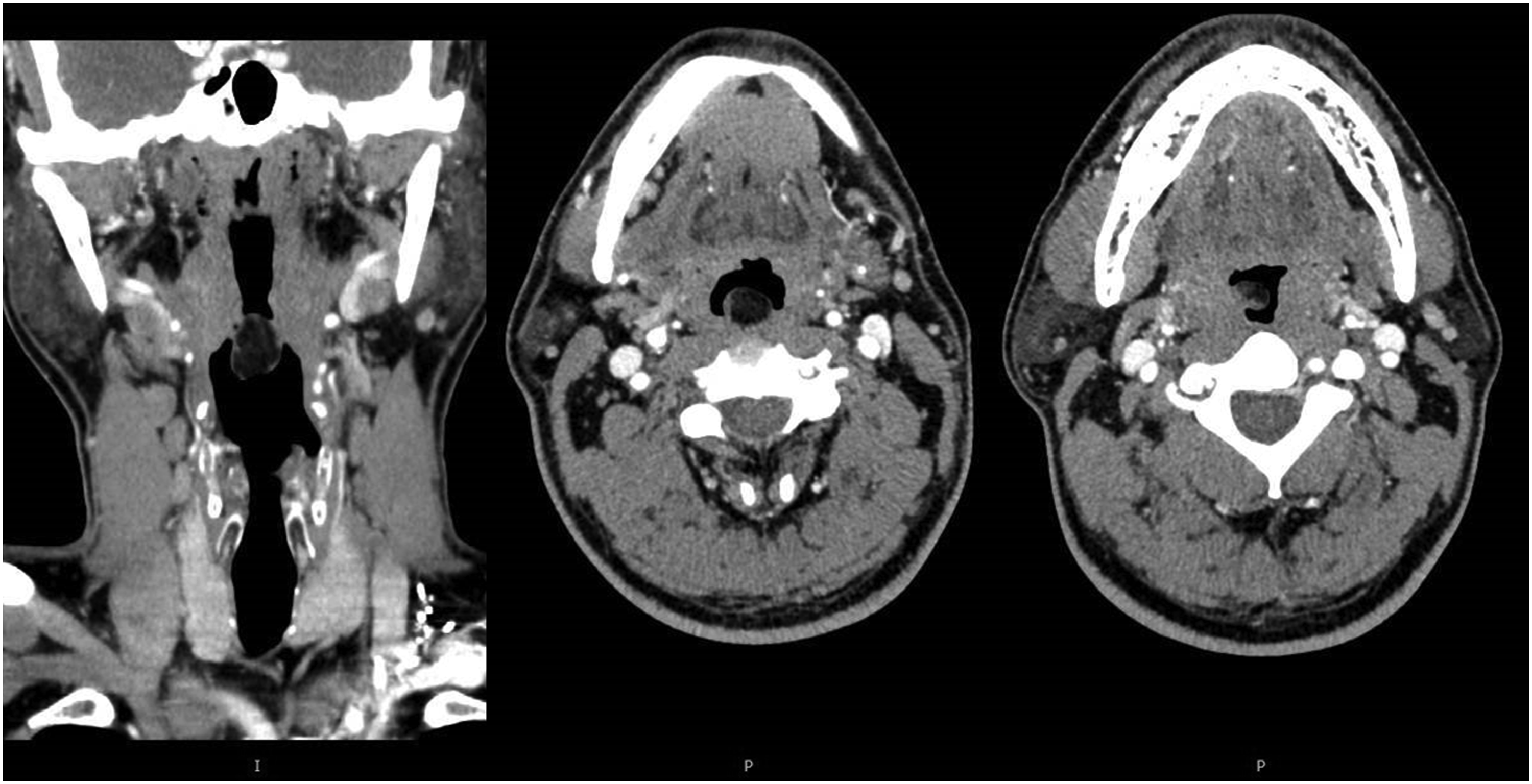
On physical examination, the bilateral tonsils were enlarged in degree II and congestive without any secretion (Figure 1). Electronic nasopharynx laryngoscopy showed enlarged tonsil crypts and a smooth and pale-yellow mass on the surface of the right tonsil which blocked some part of the pharynx (Figure 2). A contrast-enhanced computed tomography scan indicated a low-density neoplasm on the right side of the oropharynx, which was attached to the right tonsil and not strengthened during enhanced scanning (Figure 3). Pharynx obstruction before operation. Bilateral tonsils were enlarged in degree II enlargement, and the mass (blue arrow) was on the surface of the right tonsil. Electronic nasopharynx laryngoscopy. A smooth and pale-yellow mass (blue arrow) was on the surface of the right tonsil and blocked part of the pharyngeal cavity. Enhanced CT scanning of the neck. The neoplasm was on the right side of the oropharynx and attached to the surface of the right tonsil. No obvious enhancement was found. The enhancement value (Hounsfield units) of the mass was significantly lower than that of its surrounding tissues.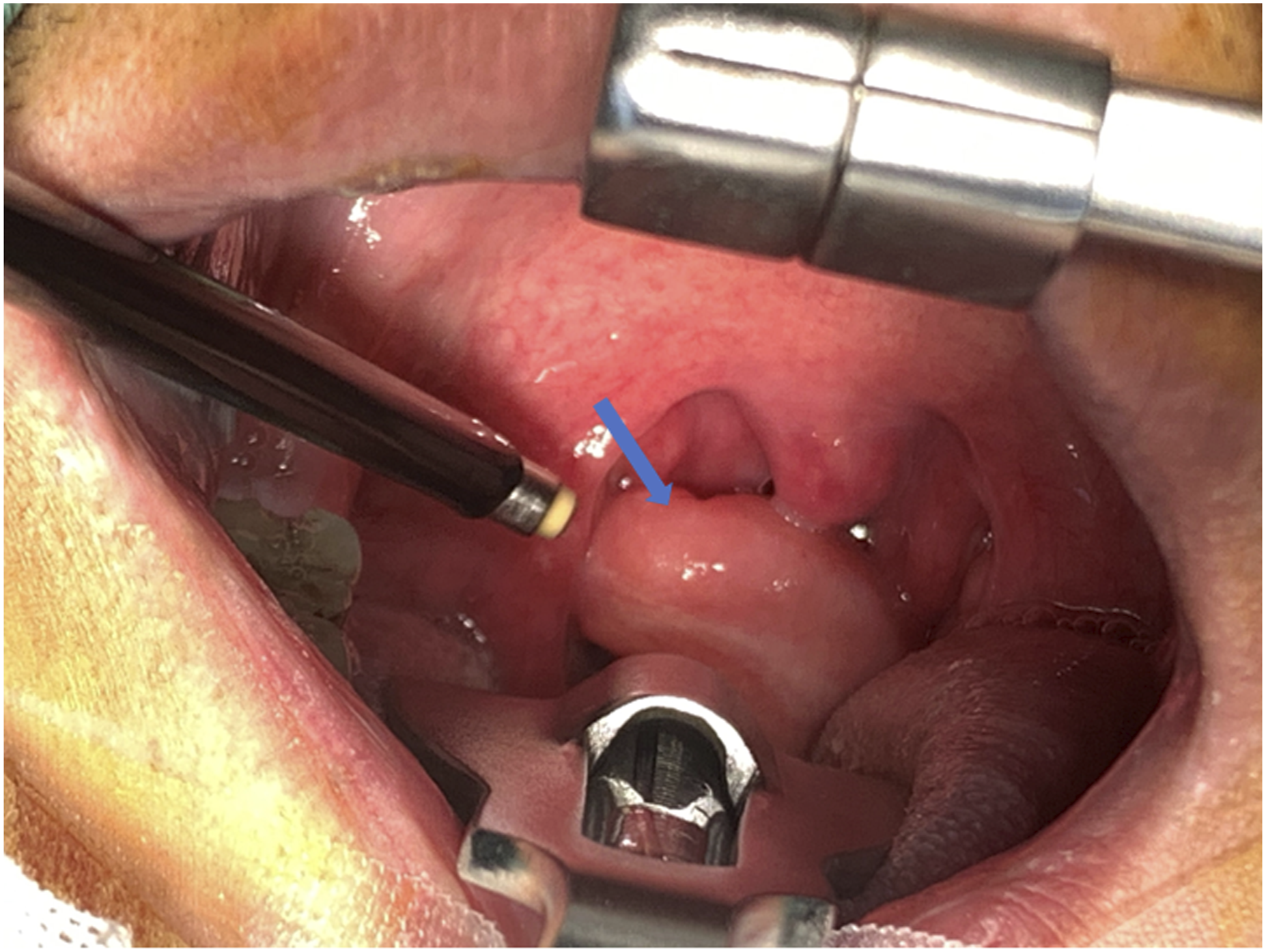
With the presence of clinical and radiological evidence, we performed the right tonsillectomy and neoplasm resection after successful general anesthesia. The operations went smoothly with no significant incidents. The neoplasm (presented as a polypoidal mass) was light yellow in color, oval in shape, soft in feel, and had a waxy surface and rich blood supply, and was measured 20 × 15 × 10 mm (Figure 4). There was no adhesion between the right tonsil and its peripheral tissue. The neoplasm after the operation. The soft neoplasm was on the surface of the tonsil measuring about 20 × 15 × 10 mm. The neoplasm and right tonsil were completely removed in operation.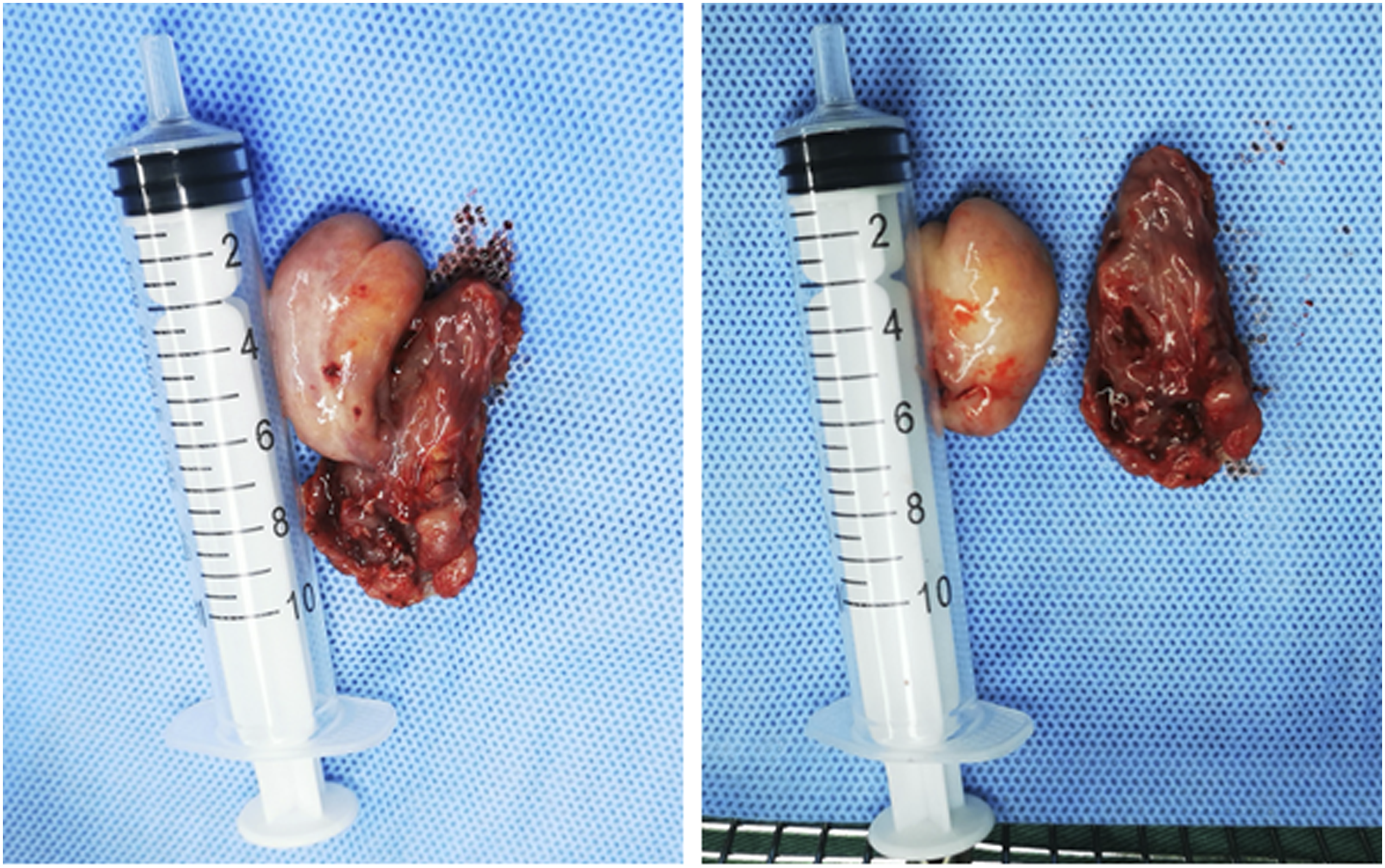
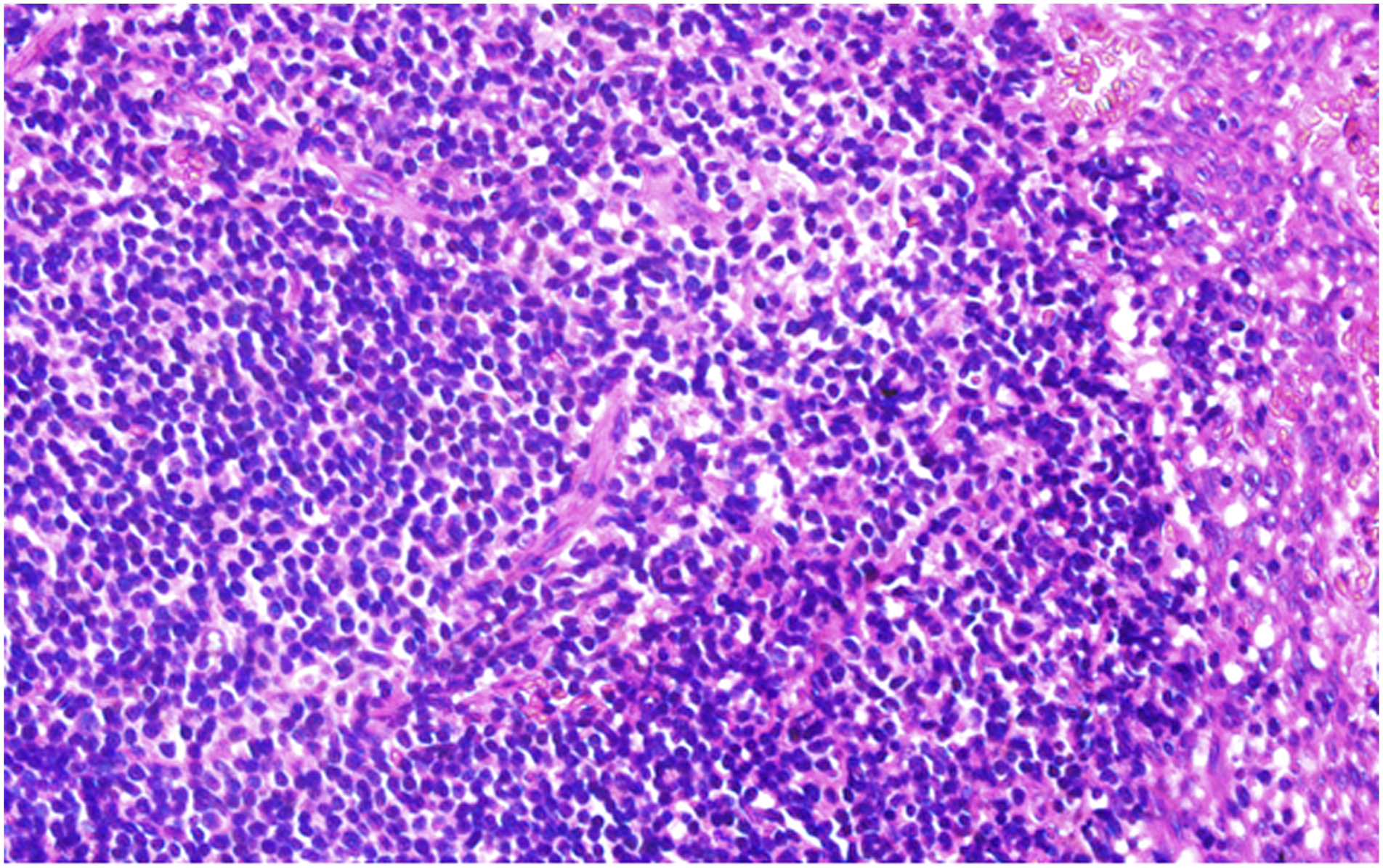
Histological view of the excised specimen showed that tonsillar tissue was infiltrated with masses of abnormal mature adipose cells covered by complete nonkeratinizing squamous epithelium. The neoplasm was composed of a large number of mature adipocytes and thick fibrous strands which contained capillaries filled with erythrocytes. Based on the histological examination and integrated analysis, the neoplasm was finally identified as fibroangiolipoma (Figure 5). In addition, abundant inflammatory cells infiltrate were seen in the tonsils (Figure 6). Histopathology (hematoxylin and eosin stain) of the excised specimen of the neoplasm. The neoplasm was infiltrated with masses of abnormal mature adipocytes (a) covered by complete nonkeratinizing squamous epithelium (b) (original magnification ×100). The neoplasm was composed of a large number of mature adipocytes and thick fibrous strands (c) and capillaries (d) (original magnification ×400). Histopathology (hematoxylin and eosin stain) of the excised specimen of the right tonsil. A large number of inflammatory cells (most were lymphocytes) infiltrated the tonsillar tissue (original magnification ×400).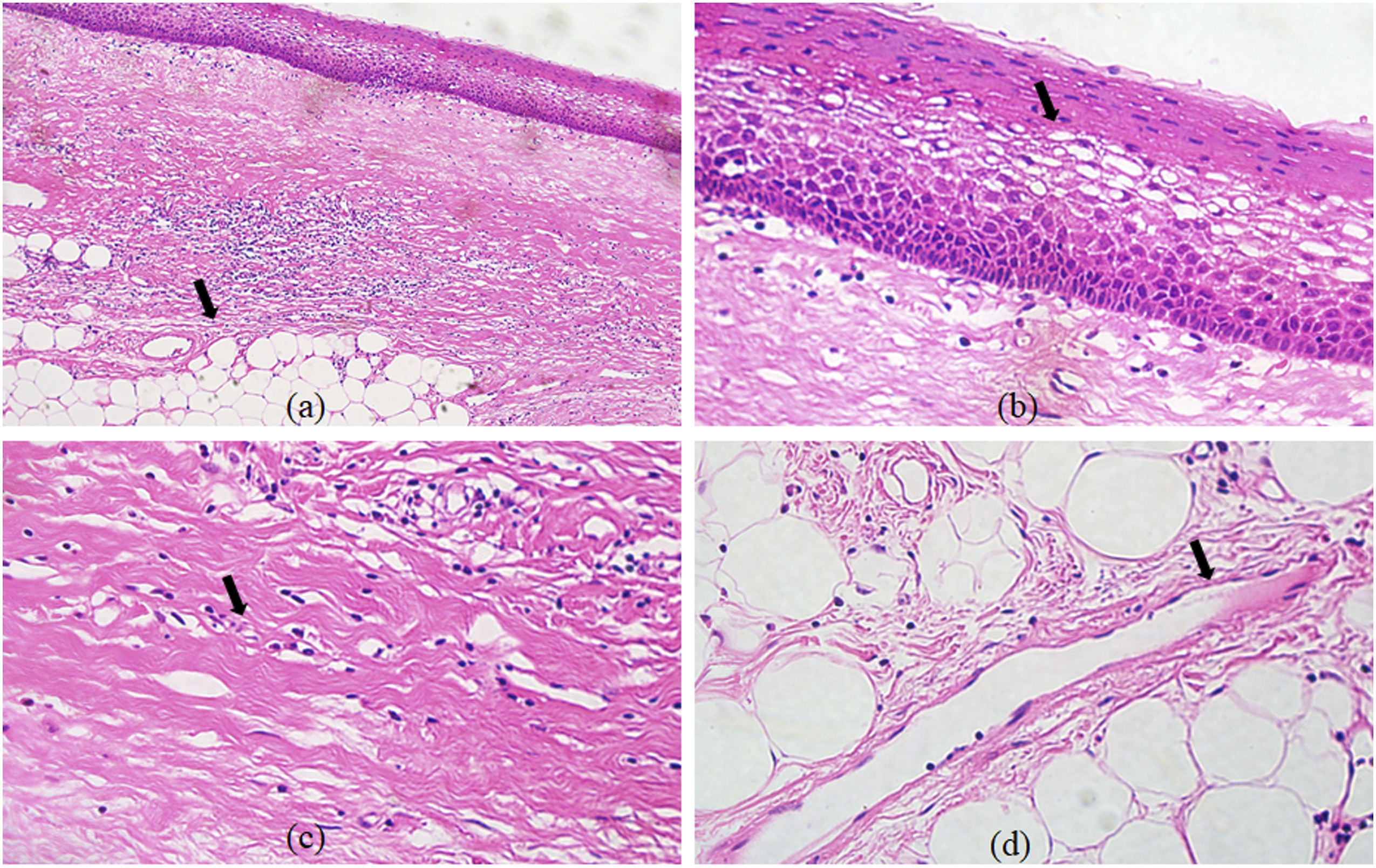
At 6 months postoperatively, the patient had a good wound healing and showed no evidence of recurrence.
Discussion
Lipomas are benign slow-growing neoplasms and occur commonly in subcutaneous tissue. These neoplasms occur among individuals at different age stages and can be asymptomatic with few clinical manifestations and could be ignored by patients. Lipomas have been reported in gastric tissue, 3 bronchial tube, 4 intraoral area, 5 and cardiac tissue. 6 Nevertheless, as a type of lipoma, fibroangiolipoma in the head and neck is uncommon. It is well-known that tonsils are the important part of the immune system in human, and their normal framework is usually devoid of adipocytes. Several cases of tonsillar lipomas have been reported previously, 7 -9 and the diagnosis of tonsillar fibroangiolipoma is mainly based on histological examination. A microscopic one is composed of mature adipocytes with intervening fibrovascular connective tissue septae, along with tonsillar lymphoid tissue at the periphery (hematoxylin and eosin stain).
In this case, the tonsil tissue was filled with a large number of inflammatory cells, but there was no direct correlation between chronic tonsillitis and the susceptibility to fibroangiolipoma. We suspected that the history of systemic multiple lipomas and tobacco addiction may serve as predisposing factors for tonsillar fibroangiolipoma. Additionally, the inflammatory cells might involve in the migration of adipose stem cells to the tonsils. Further research is needed for their confirmation. At present, tonsillectomy is still considered the optimal treatment for adequate management of tonsillar fibroangiolipoma.
Conclusion
We presented a case of palatine tonsillar fibroangiolipoma in a Chinese man with the history of multiple lipomas on the back and extremities and performed tonsillectomy for its management. It should be taken into account in the differential diagnosis at the presence of one or more benign lesions of the tonsils. With the spotlight on the pathogenesis of fibroangiolipoma, further research is required to explore the occurrence and development of tonsillar lipomas.
Footnotes
Authors' contributions
Rui Lu and Zhiyong Li drafted the manuscript and revised it critically for important intellectual content. Zhiyong Li, Xiong Chen, and Shucheng Yin gave final approval of the version to be published. Rui Lu, Zhiyong Li, Shucheng Yin, and Xiong Chen contributed to the conception. All authors agreed to be accountable for all aspects of the work.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study is supported by the National Natural Science Foundation of China (NSFC) grants 81900913 (Zhiyong Li) and 81372881 (Shucheng Yin).
Ethics Approval and Consent to Participate
The patient involved in this study gave his informed consent. Institutional review board approval of our hospital was obtained for this study.
Consent for publication
The patient involved in this study gave his informed consent.