
Abstract
We describe a rare occurrence of unilateral vocal fold paralysis associated with a cervical osteophyte abutting the course of the recurrent laryngeal nerve. Trans-nasal laryngoscopy is vital in diagnosing vocal fold paralysis, but often does not provide insight into etiology. This case highlights the importance of radiographic imaging in newly diagnosed vocal fold paralysis, and underscores the principle that a diagnosis is not idiopathic until all sources have been ruled out.
Significance statement
We describe a rare occurrence of unilateral vocal fold paralysis associated with a cervical osteophyte abutting the course of the recurrent laryngeal nerve. Trans-nasal laryngoscopy is vital in diagnosing vocal fold paralysis, but often does not provide insight into etiology. This case highlights the importance of radiographic imaging in newly diagnosed vocal fold paralysis, and underscores the principle that a diagnosis is not idiopathic until all sources have been ruled out.
Main text
A 70-year-old female presented with 6 months of dysphonia impacting her conversational as well as singing voice. She described difficulty with vocal projection, range and endurance, and easily running out of breath when talking. Concurrently, she had been having chest congestion, notably not responsive to inhalers. Nothing seemed to help or make it worse. It was overall stable over the preceding months. On exam, her voice was mildly rough and breathy with reduced projection. Videostroboscopy was performed which showed right vocal fold bowing, a fixed paramedian position, and a present jostle sign (Figure 1A, B). Although laryngeal electromyography (LEMG) was not performed for the definitive diagnosis, these findings are most consistent with unilateral vocal fold paralysis. A vocal fold injection augmentation was discussed, but ultimately the patient opted for voice therapy. Laryngoscopy showing right vocal fold paralysis. (A) Right fold is paramedian and fixed with dilated right pyriform sinus. (B) Vocal fold adduction during phonation results in persistent glottic gap and insufficiency from flaccid right vocal fold.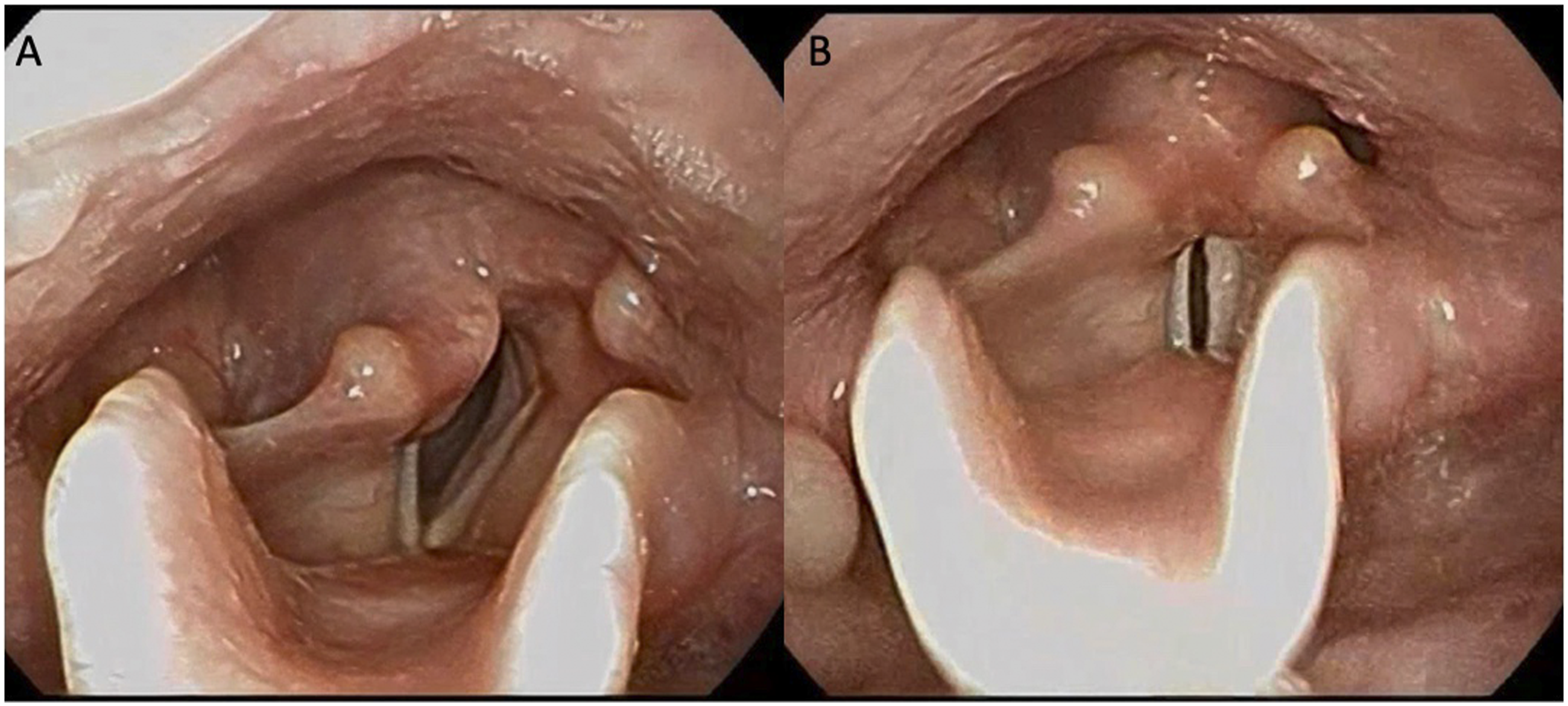
She was seen 2 months later and while she remained functionally well, her vocal fold remained paralyzed. A computerized tomography (CT) scan was ordered to evaluate the course of the recurrent laryngeal nerve. The CT scan revealed asymmetric dilation of the right pyriform sinus compared to the left as well as a bulky right ventrolaterally projecting osteophyte arising from the C56 level abutting and indenting the right carotid sheath as well as the right posterior aspect of the cricoid in the expected location of the recurrent laryngeal nerve (Figure 2A, B). CT scan of the neck with contrast. Thin white localizer lines present. (A) Axial slice showing osteophyte abutting course of the recurrent laryngeal nerve with only 7 mm bone to cartilage separation (arrow). (B) Sagittal slice showing the anterior projection of the cervical osteophyte again abutting the course of the recurrent laryngeal nerve (arrow).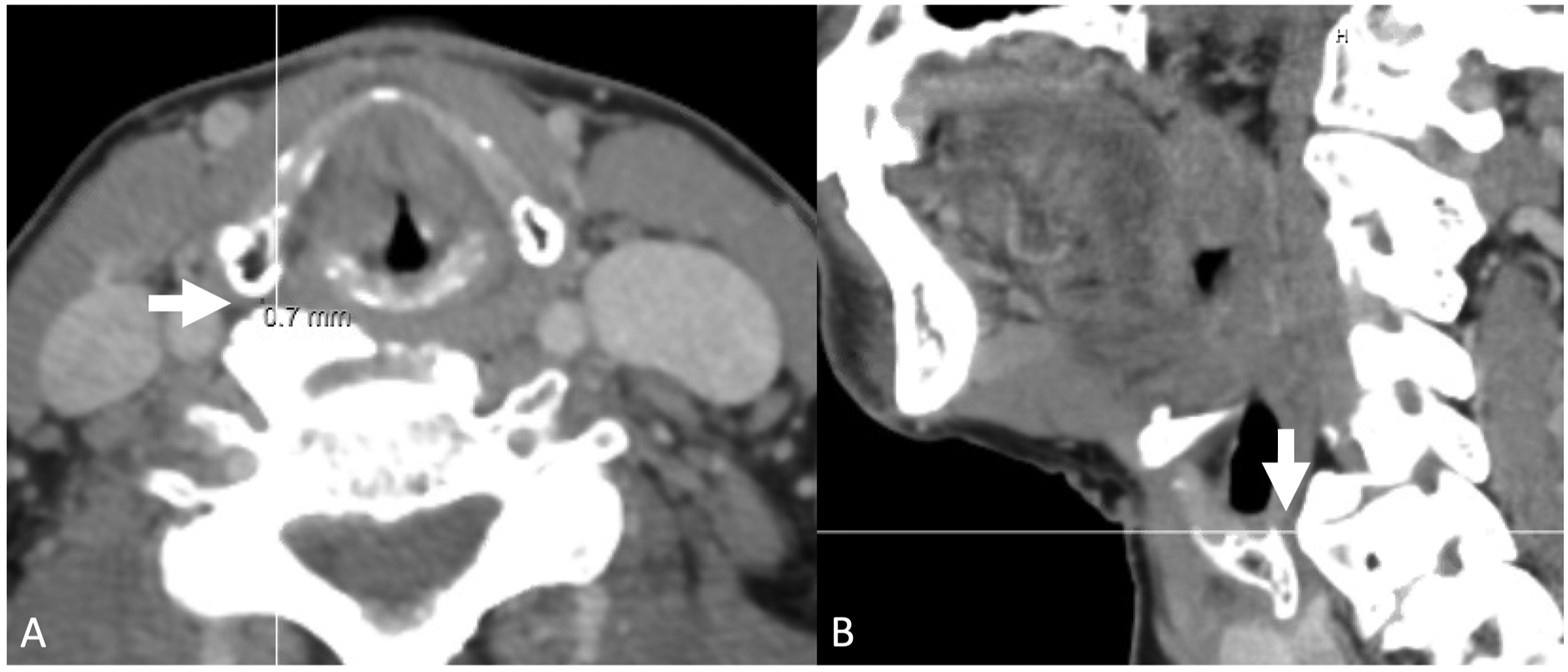
Vocal fold paralysis is relatively uncommon with an incidence rate of less than 1% in the population. 1 Bilateral vocal fold paralysis is seen in as many as 9% of these cases. 2 Unilateral vocal fold paralysis is caused by damage to the recurrent laryngeal nerve which can result in dysphonia, difficulty swallowing or dysphagia, and shortness of breath. Symptoms can manifest as a breathy voice, dysphagia, regurgitation, and even difficulty exercising due to increased airway resistance. 3
There are several etiologies for unilateral vocal fold paralysis including cancer, surgical injury, trauma, and idiopathic. Cancers such as metastatic lung cancer and laryngeal carcinoma had been leading causes for unilateral vocal fold paralysis. 3 Surgical injury to the recurrent laryngeal nerve, however, is now the leading etiology for unilateral vocal fold paralysis and paresis with incidence rates of 1.6% paralysis and 2.96% paresis in thyroidectomies. 4 Other surgical procedures associated with vocal fold paralysis include spine and cardiothoracic surgeries. Trauma to the vocal fold or other parts of the airway contributes to unilateral or bilateral vocal fold paralysis. 3 It is not uncommon to see temporary unilateral vocal fold paralysis or paresis caused by endotracheal intubation following general anesthesia. 5 Lastly, idiopathic etiologies are thought to be secondary to viral infection and are seen in about 1.6 per 100,000 persons, 29.5% of whom achieve spontaneous recovery within 4 months.6,7
In the past, similar cases of more inferior osteophytes associated with unilateral vocal fold paralysis have been reported with the patient responding to speech therapy. A reported case of bilateral vocal fold paralysis secondary to C3C7 cervical osteophyte has also been reported in an 81-year-old male. 8 Cervical osteophytes are not the only rare etiologies diagnosed through cross-sectional imaging. 9 Vocal fold paralysis from Ortner’s syndrome is diagnosed via cross-sectional imaging showing enlarged cardiac structures, causing recurrent laryngeal nerve palsy through mechanical compression at the aorticopulmonary window. 10
Our case illustrates a cervical osteophyte abutting the course of the recurrent laryngeal nerve associated with unilateral vocal fold paralysis. This case highlights the importance of a thorough work-up in newly diagnosed vocal fold paralysis including cross-sectional imaging. It also highlights that management decisions are patient-specific, largely driven by functional deficit, and impact quality of life and safety. In the aspirating patient, procedural intervention is often the right answer. In a patient with a safe swallow and mild deficit, voice therapy and support may be all that is needed.