
Abstract
Neck emphysema after tonsillectomy surgery is very rare. We present a case documenting the conservative management of a post-tonsillectomy neck swelling, accompanied by crepitus. Computed tomography revealed a large air density at the region of the right masticator space and the masseter muscle, proximal to other deep neck spaces and muscles. Further investigations of her associated symptoms resulted in an additional diagnosis of systemic lupus erythematosus. We have also explored the signs and symptoms associated with such cases, along with a discussion of the literature published on surgical emphysema post-tonsillectomy.
Introduction
Tonsillectomy is one of the most common procedures performed by otolaryngologists, 1 with reported overall complications in adults in about 20% of cases. 2 Most complications include post-operative infection, pain, and bleeding.
Subcutaneous facial emphysema is a rare post-tonsillectomy complication, first reported in the literature in 1910, occurring in both pediatric and adult patients. 1,3 It is defined as a facial swelling due to presence of air in between the fascial plane and the connective tissues. 4 Although it is rare, clinicians should be aware of it and immediately manage the patients to prevent any life-threatening events such as airway obstruction or cardiac arrest due to tension pneumomediastinum. 3
Case Presentation
A 40-year-old woman, with no known chronic illness, presented to the otolaryngology clinic due to of recurrent attacks of acute follicular tonsillitis, with high grade fever and antibiotic intake, usually intravenous, occurring every few months in the last 3 years. She opted to undergo an elective tonsillectomy. The tonsillectomy was administered by the dissection method using the MiFusion® Thermal Fusion Technology ENTceps®, preventing bleeding or any undesirable complication. She had an unremarkable recovery period.
Three days later, she presented to the emergency room with swelling on the right side of her neck, associated with tenderness, and two spikes of fever. No signs or symptoms indicative of airway compromise were noted. On physical examination, the patient was afebrile with unremarkable vital signs, was well-oriented, and was not in distress or pain. Neck palpation revealed a right-side neck swelling, extending from the right preauricular area to right clavicle, with tenderness and crepitation. Examination of the oral cavity and oropharynx showed normal healing mucosa on the tonsillar bed, with no asymmetry or specific findings. Computed tomography (CT) revealed subcutaneous and deep soft tissue air densities, suggestive of surgical emphysema (Figure 1). The patient was admitted for observation and conservative management. Computed tomography shows the extent of the air densities.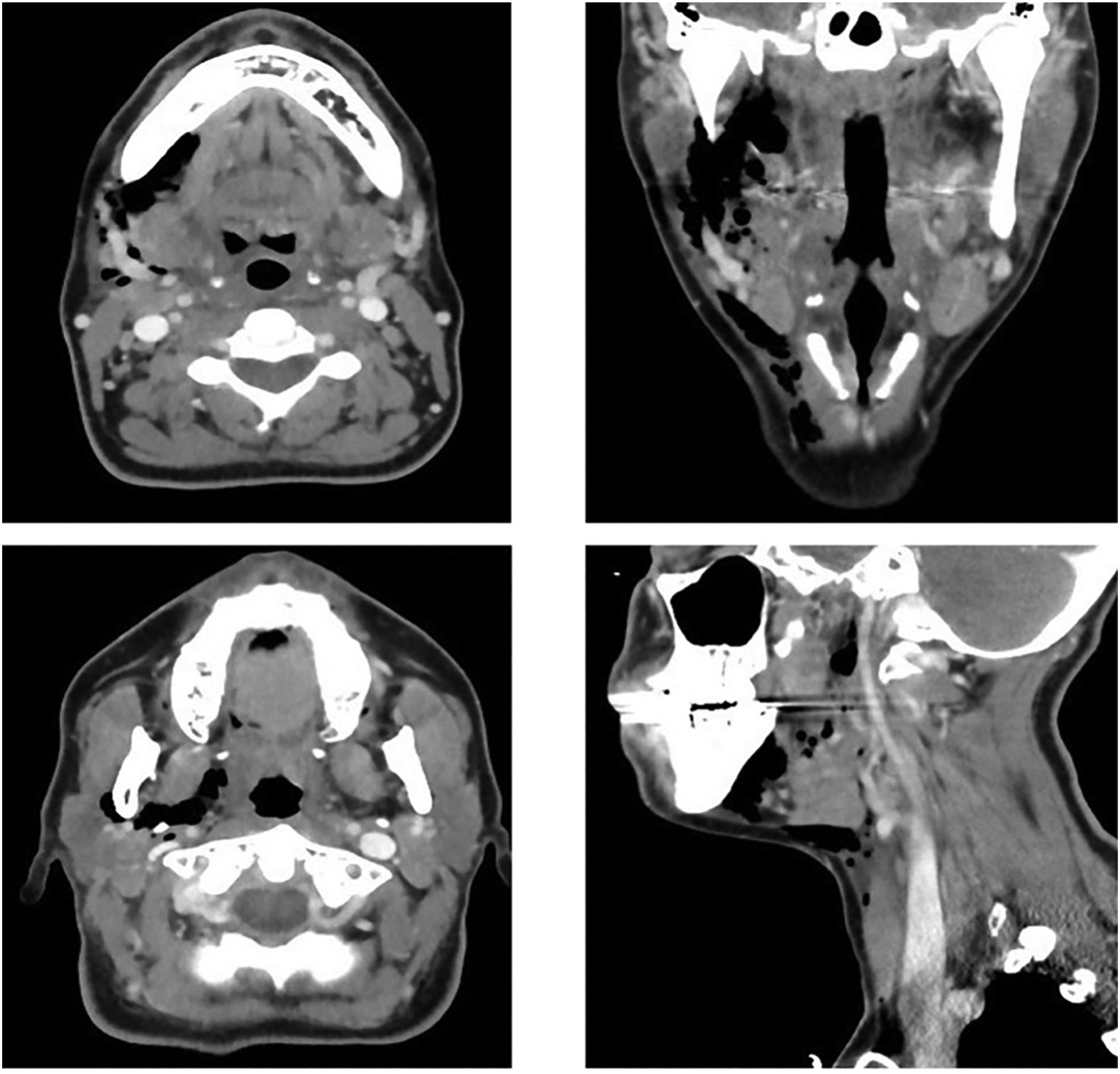
The following day, the patient complained of left knee swelling and hotness, and mild cervical vertebral pain, Magnetic resonance imaging of the neck helped confirm surgical emphysema without any abnormal findings. The patient consulted a rheumatologist, who provided a differential diagnosis of systemic lupus erythematosus (SLE) and rheumatoid arthritis, necessitating further investigations. The swelling and crepitation over the right neck region resolved dramatically from Day 1 post-admission. She was discharged on Day 3 in a stable condition, with further follow-up appointments at both the Otolaryngology and Rheumatology departments. A definitive diagnosis of SLE was provided by the Rheumatology department.
Discussion
Subcutaneous emphysema has been reported as a rare complication post-tonsillectomy. The severity of the emphysema varies from mild subcutaneous emphysema to serious life-threatening airway compression, pneumomediastinum, and pneumothorax complication. 1 The pathophysiology of this complication is still unclear, but two main theories have been proposed in the literature. The first theory describes it as an anesthesia-related complication through a laryngeal or tracheal tear, caused by the endotracheal tube intubation, hyperinflation of cuff tube, and/or high alveolar pressure ventilation. 5 -7 The second theory postulates a mucosal and muscular tear injury of the pharynx in the superior constrictor muscle and deep cervical fascia, through the tonsillar bed, which allows air to enter deep neck spaces. 6,7 Emphysema presentation has been reported to occur either immediately during the operation, or in the recovery room if the injury occurred and was noted during the procedure. 6 -8 However, several studies have reported immediate emphysema without the operators noticing any intraoperative injury to the mucosa. 1,5,9,10
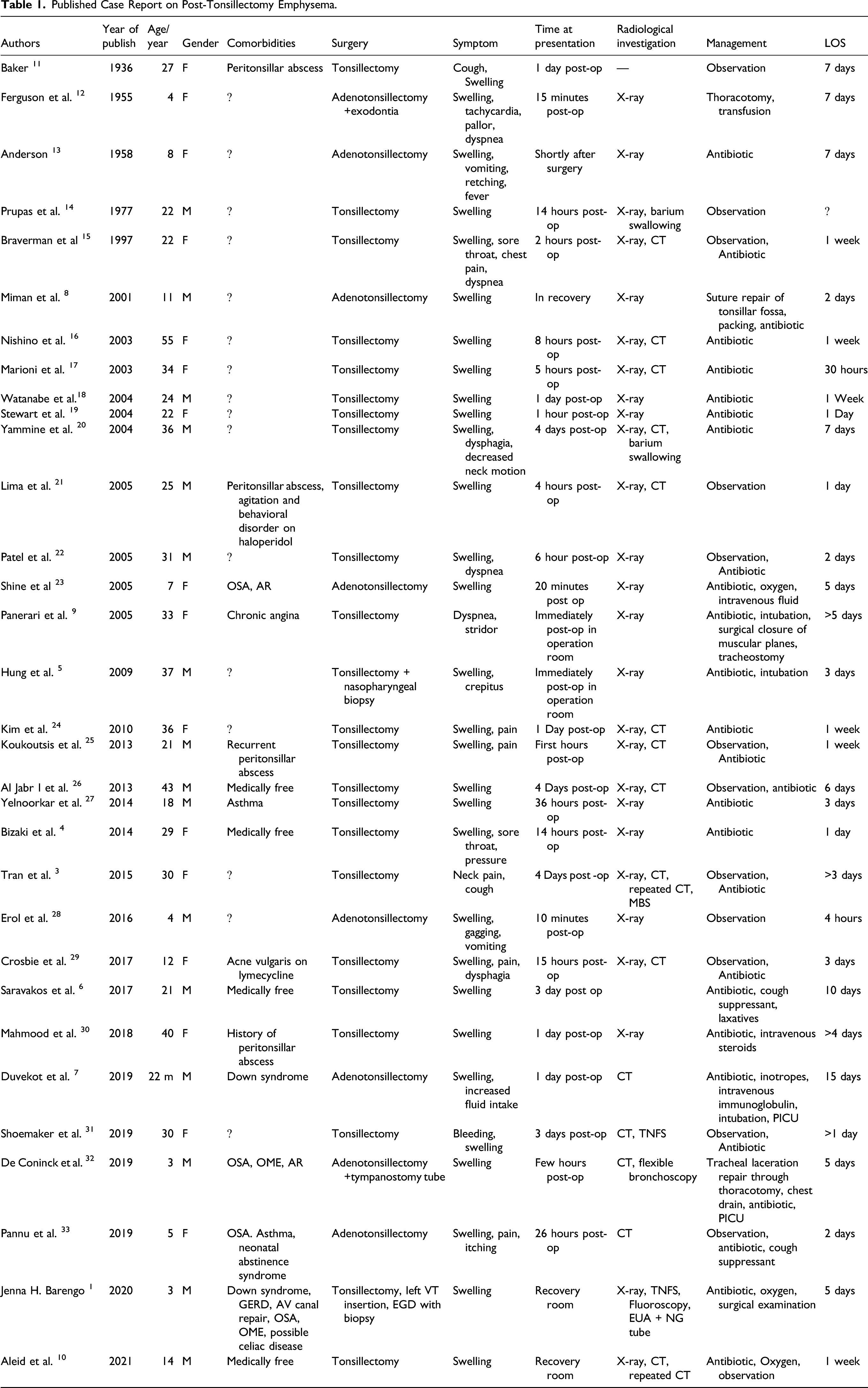
Published Case Report on Post-Tonsillectomy Emphysema.
In this case report, the patient underwent an uneventful tonsillectomy and presented 3 days post-tonsillectomy with neck and facial swelling, accompanied with tenderness. Her symptoms were associated with systemic manifestations, such as cervical neck pain and knee swelling. This was investigated by the rheumatology department and subsequently diagnosed as SLE. A literature search revealed that several case reports have observed SLE and spontaneous recurrent emphysema, pneumomediastinum, and pneumothorax. 34 -37 However, the correlation between these entities is unclear. We postulate that, when compared with a healthy population, SLE patients who undergo tonsillectomy are more likely to develop surgical emphysema, regardless of the pathophysiology of developing such a complication (anesthesia-related vs surgical-related).
Surgical emphysema post-tonsillectomy is a rare but potentially serious complication. Adults are more prone to develop surgical emphysema in comparison to pediatric patients, and their presentation is usually delayed. Most patients are treated conservatively with antibiotics and observation. However, some patients may require further airway establishment and surgical intervention. Further studies need to be conducted to identify the pathophysiology of surgical emphysema post-tonsillectomy and the possible correlation between SLE and the manifestation of such complications.
Footnotes
Acknowledgments
This case was reported in Security Forces Hospital, Riyadh, Saudi Arabia
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Patient Consent
Patient’s consent was received for this case report to be published.