
Abstract
Cutaneous metastases from squamous cell carcinomas of the head and neck region are uncommon, and their location at the nasal tip is exceptionally rare. A patient, previously treated with surgery and chemoradiation for a hypopharyngeal squamous cell carcinoma, developed several red nodular skin lesions at the nasal tip. Biopsy revealed cutaneous metastasis from the primary tumor. This manifestation was previously described as a “clown nose,” given their appearance and location. Skin lesions should raise suspicion of malignancy, despite their location at uncommon places, particularly in patients with previous diagnosed cancer. Clinicians must be aware that metastases from head and neck cancer can present as a “clown nose.”
Keywords
Introduction
Cutaneous metastatic lesions in the facial region are a rare occurrence, 1 and their location at the nasal tip with a red nodular appearance has been described as “clown nose,” due to the similarities to the clown’s red bulging fake nose. Soyer et al first used the term in 1990 to describe a cutaneous metastasis from breast cancer. 2 We present the case of a nasal tip metastasis from a hypopharyngeal squamous cell carcinoma, previously submitted to pharyngolaryngectomy and adjuvant chemoradiotherapy, manifesting as a “clown nose” 10 months after surgery.
Case Report
A 68-year-old male, with heavy smoking and drinking habits, presented with complains of sore throat for 2 months. He had no other relevant past medical history, and during physical examination, an extensive hypopharyngeal lesion centered at the right pyriform sinus was observed. Imaging study and biopsy of the lesion were performed, the latter revealing a moderately differentiated squamous cell carcinoma. Clinical TNM was cT4aN0M0 (stage IV), 3 and after multidisciplinary discussion, the patient underwent primary surgical treatment: pharyngolaryngectomy with selective bilateral neck dissection of areas II–IV. The histopathologic study of the surgical specimen revealed a pT4aN2cR1 tumor, and the surgical approach was complemented by adjuvant chemoradiotherapy. Patient was submitted to a total dose of 60 Gy under three-dimensional conformal radiotherapy technique, with concomitant cisplatin administration.
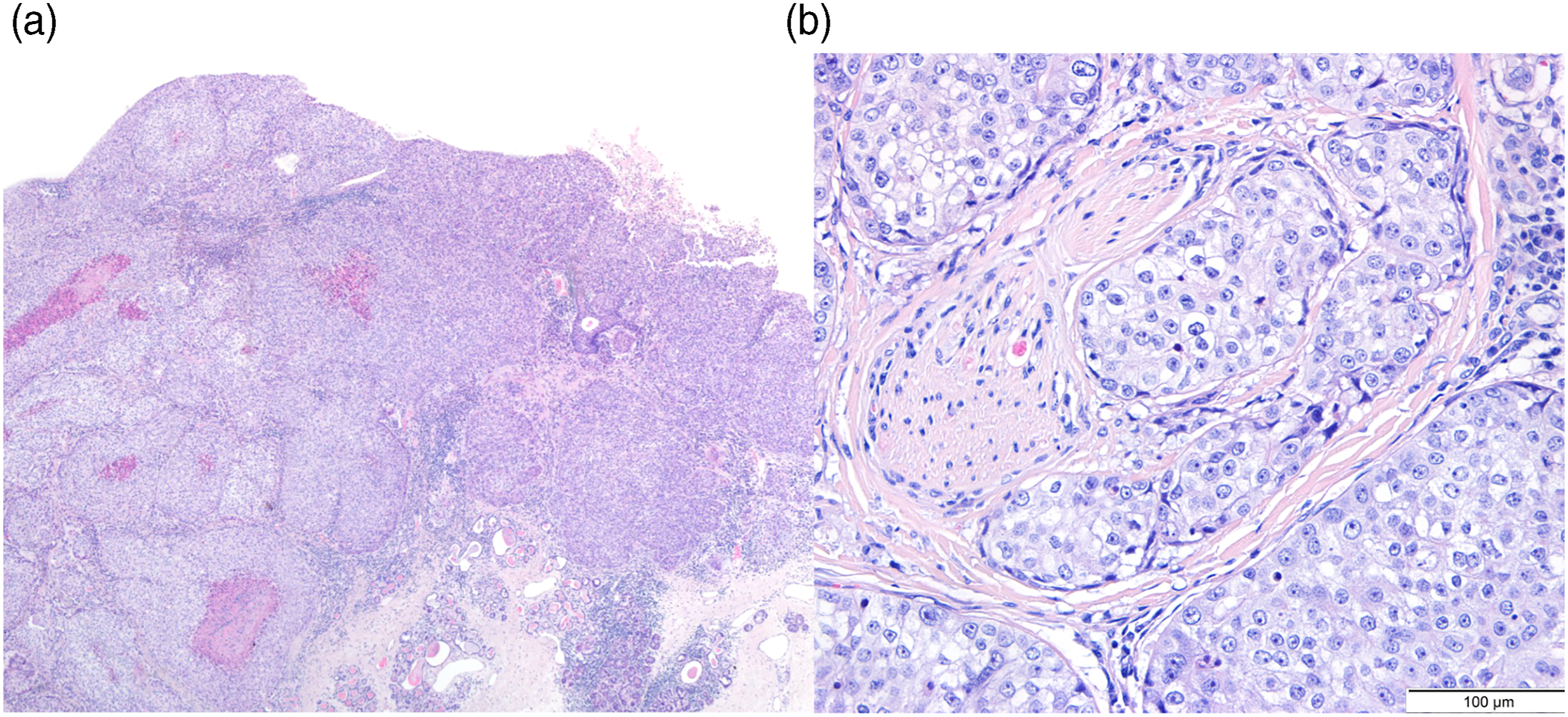
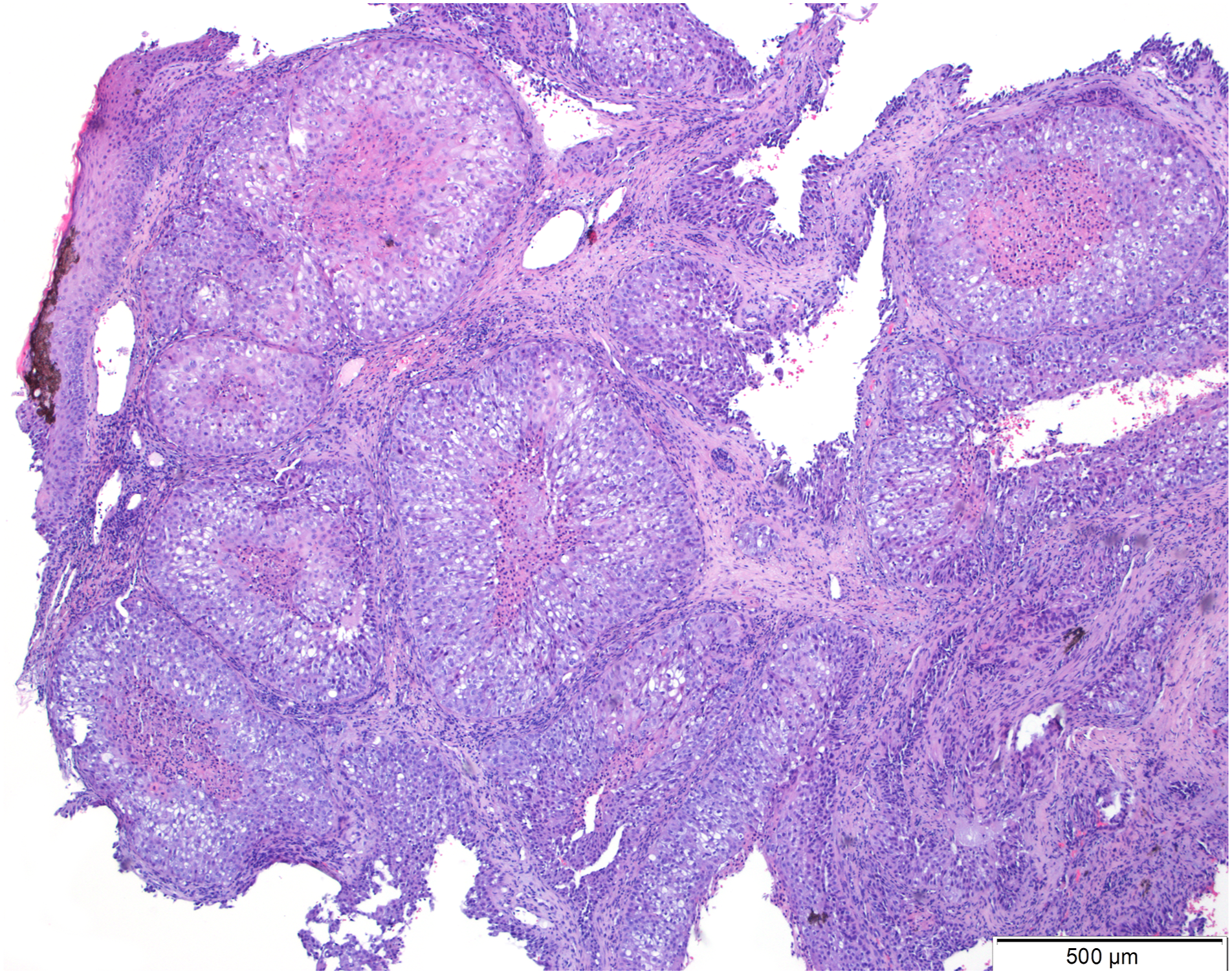
Five months after surgery, follow-up imaging revealed regional recurrence and suspected metastatic lesions in the lungs and brain. Consequently, palliative brain radiotherapy and weekly paclitaxel chemotherapy was initiated. Ten months after surgery, the patient developed nasal hyperesthesia, and clinical examination showed multiple reddish nodular lesions at the nasal tip (Figures 1A and 1B). The biopsy revealed a squamous cell carcinoma with morphologic and immunohistochemical characteristics compatible with a metastasis from the primary tumor (Figures 2A and 2B and 3). The patient died 11 months after surgery. (A) and (B) Clown nose lesions. (A) and (B) Microscopic view of the primary tumor showing a moderately differentiated squamous cell carcinoma, left image (H&E, x40), with perineural invasion, right image (H&E, x100). Nasal lesion consisting of moderately differentiated squamous cell carcinoma with identical morphologic characteristics to the primary tumor (H&E, x40).
Discussion
The most common metastatic sites for head and neck squamous cell carcinomas are the lungs, liver, and bone. 4 Skin metastases are uncommon, with incidences ranging from .7 to 7% described in the literature.4-6 Breast cancer is the most frequent to metastasize to the skin, followed by the bronchus and lung. A meta-analysis with over 20.000 patients with tumor registries reported a cutaneous metastases overall incidence of 5.4%. 1 Regarding pharyngolaryngeal tumors, it has been recognized that subglottic larynx and hypopharynx have an increased incidence of distant metastases, when compared to glottic or supraglottic primary lesions. 6
The nasal tip is a rare location for cutaneous metastasis, and such occurrence has been reported in patients with lung/bronchial cancer,7-16 esophageal cancer,17-20 breast carcinoma,2,21 thyroid cancer,22,23 cervical cancer, 24 hepatocellular carcinoma, 25 choriocarcinoma, 26 and chordoma. 27 To our knowledge, only 4 cases of metastases to the nasal tip from head and neck squamous cell carcinomas have been described: two were primaries from the hypopharynx28,29 and the other two were basaloid variants from the larynx.30,31 The macroscopic characteristics of the lesions can vary from an induration of the skin and subcutaneous tissues to a nodular or exophytic mass, typically red in color. Although in the majority of the cases, the patient has an already known malignancy, a “clown nose” can be the first sign leading to the diagnosis of a primary tumor.12,16 While the term is mostly applied in the literature to secondary metastatic lesions, it has also been linked to cases of primary skin tumors of the nasal tip and, recently, as a manifestation of genetic syndromes.32-34
Hypopharyngeal cancer is associated with a higher incidence of delayed regional and distant metastatic disease when compared to laryngeal cancer. 6 In the present case, besides the tumor location, there were other characteristics shown to be related with an increased potential of metastatic lesions, as the presentation at an advanced stage and regional spread to the neck lymph nodes. 6 Occurrence of skin metastases from head and neck squamous cell carcinomas is associated with a poorer prognosis, with most patients dying a few months after the diagnosis. 5 The median time to the occurrence of distant skin metastases is significantly shorter when compared to the time to occurrence of metastases in other locations. 5
Nasal tip cutaneous metastasis is a rare event in head and neck squamous cell carcinomas. In this particular case, the patient was already under palliative care due to disease progression, so no major changes in the disease management were undertaken. Skin metastases can be the first sign of disease relapse and are tied to a poor prognosis, which may dictate a change in the treatment approach. Clinicians should pay attention to suspicious skin lesions, particularly in patients with a prior or current history of head and neck cancer.
Footnotes
Authors’ Note
Written consent was obtained from the patient’s family.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.