
Abstract

Significance statement
Angiomyxomas are mesenchymal benign tumors localized to the trunk, head and neck, lower extremities, and genitals with a frequency of 0.008%–3%. They are neoplasms of uncertain differentiation, classified as aggressive and superficial. Superficial angiomyxomas of the oral cavity are extremely rare. This is the first clinical report of a large angiomyxoma of the tongue causing dysphagia; treated successfully with surgical excision using CO2 laser.
A 70-year-old female patient referred to our Ear, Nose, and Throat department (ENT) with a 6 month history of progressive dysphagia. Clinical examination of the oral cavity revealed a large tumor in the apex of the tongue (Figure 1A). Palpation of the tongue showed a soft, mobile, non-ulcerated, and well-defined mass. In addition, no palpable lymph nodes of the neck have been found. Patient’s breathing was normal, but her speech was impaired to some extent, along with difficulty in swallowing. The patient had dysphagia, as the tongue movement was insufficient due to the size of the mass. The endoscopic examination did not reveal any other pathology on the base of tongue and larynx. Magnetic resonance imaging (MRI) showed a well-defined cystic mass with a diameter of 4.1 x 3.3 x 3.4 cm in the apex of the tongue (Figure 2) and no lymph nodes of the neck. A) Preoperative image of superficial angiomyxoma arising from the tongue, B) the mass after the excision, and C) postoperative image of the mass. Parasagittal reconstruction section of magnetic resonance imaging (MRI) showing the mass (yellow arrows), arising from the apex of the tongue.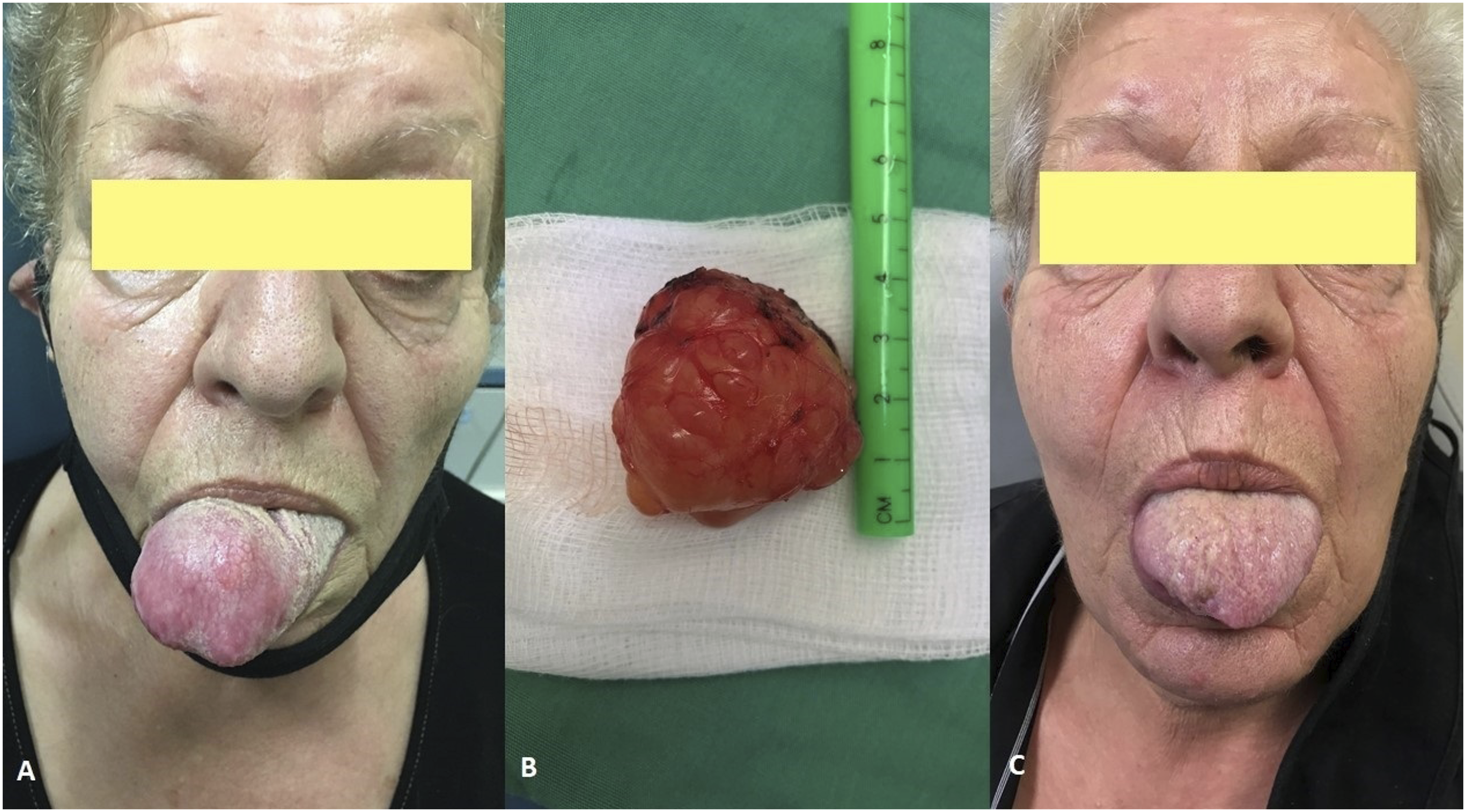

Based on clinical and imaging findings, an excisional biopsy of the mass under general anesthesia and nasotracheal intubation was decided. A horizontal incision along the apex of the tongue has been performed, protecting the lingual papillae. The well-encapsulated, yellowish mass was removed en-block by means of Sharplan CO2 laser (Sharplan Lasers LTD, London, United Kingdom) at a continuous super pulsed mode, focused beam, 5 to 9 Watts and 0.5 mm spot size (Figure 1B). Absorbable sutures were used to reduce the dead space of the side of excision.
Postoperatively, there were no complications and the patient was discharged on the second day. The histological examination revealed an epithelium overlying the myxoid stroma with numerous small blood vessels and scattered spindle-shaped cells that did not show any nuclear atypia. Neutrophils and lymphocytes were infiltrating the space between small vessels. Immunohistochemically, tumor cells were positive for vimentin, CD34, and S-100 protein of the angiomyxoma (Figure 3). These features were diagnostic of a superficial angiomyxoma. The patient had a follow-up assessment 3 months later, with no evidence of relapse and symptom-free (Figure 1C). A) Histopathological and immunohistochemical examination showing A epithelium overlying myxoid stroma with small blood vessels and scattered spindle-shaped cells (H&E, ×10), B) vimentin + (x10), and C) CD34 + (x10) and D. S-100 protein + (x10). H&E indicates hematoxylin and eosin; CD indicates cluster of differentiation.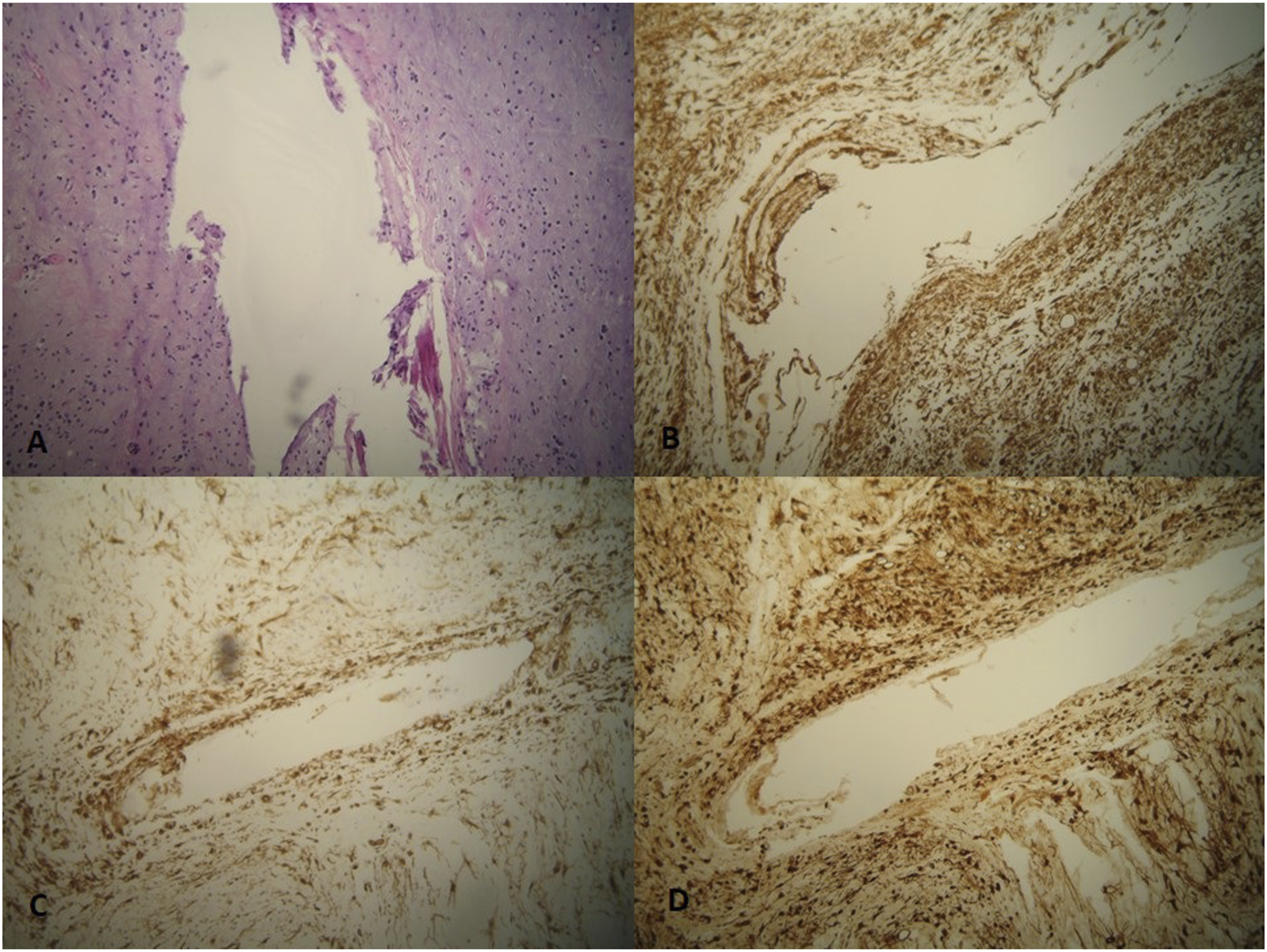
Angiomyxoma is a non-malignant tumor that originates from soft tissues with mesenchymal substance. Angiomyxomas can be found at the trunk, the lower extremities and the genitals, with those of oral and neck areas being extremely rare. They are classified as aggressive and superficial. 1 Aggressive angiomyxomas are locally infiltrative benign tumors that are formed by myofibroblastic cells with poorly defined margins. Usually are found in middle-aged women, in genitals, presenting frequent recurrences.2,3 On the contrary, superficial angiomyxomas are benign, superficial soft tissue masses with well-defined margins. They are more common in middle-aged men, and occur on the trunk but with infrequent recurrences. 4 They are extremely rare in the head and neck region with only four cases of oral angiomyxomas reported in the literature: specifically, one in the buccal vestibule, one in the upper alveolus, and two in the flour of the mouth. 4 This is the first reported case of a superficial angiomyxoma on the tongue described in the literature.
Superficial angiomyxomas are often presented as polypoid lesions. Their clinical features are not specific. When they are located in the oral cavity, resemble cysts and can have recurrences. 4 Large masses can cause functional problems such as swallowing and speech difficulties. Histologically, angiomyxomas are characterized by an extensive myxoid stroma and numerous small blood vessels. Neutrophils and stellate fibroblasts are usually present. Immunohistochemically, cells of angiomyxomas are negative for smooth muscle actin and pankeratin. 5 The differential diagnosis includes aggressive angiomyxoma, angiomyolipoma, myxoid nerve sheath tumor, myxoid neurofibroma, soft tissue myxoma, odontogenic myxoma, oral focal mucinosis, and myxofibrosarcoma.4,6
Imaging is required for the appropriate treatment of these lesions by means of computed tomography (CT) and/or MRI scans. Angiomyxomas often have a cystic appearance.7,8 The treatment of choice is surgical excision and a long-term follow-up due to frequent recurrences. 8 The excision of these lesions on the two anterior thirds of the tongue is usually performed transorally. Transoral robotic surgery could be used in poorly visible areas such as the upper alveolus. 9 Surgical excision of lingual soft tissue tumors with a CO2 laser, as in our case has a sharp and very accurate effect with little injury to surrounding non-excised tissue. During the operation, CO2 laser fiber cuts precisely and reduces blood loss, sealing small blood vessels, which leads to better hemostasis. 10 Its thermal effect does not penetrate tissues deeply and significantly influence the histological assessment of the sample. 11 The use of CO2 laser provides a smooth postoperative course with a lower risk of bleeding and inflammation than conventional surgery, presenting less pain and faster wound healing. 11
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed consent
We declare that written informed consent for patient information and images to be published was provided by the patient.