
Abstract
Dysphagia remains an unsolved problem for patients with oral cavity cancer who have undergone surgery. This randomized controlled trial was conducted to determine the effect of oral exercise in addition to standard general care and diet counseling on the physiology of swallowing. Fifty patients (25 in each group) with oral and oropharyngeal cancer who underwent tumor resection, neck dissection, and reconstruction were enrolled in this study. The Rosenbek penetration-aspiration scale and modified barium swallow study were administered at 1 and 4 month(s) postoperatively. We observed significant improvements in the intervention group regarding the penetration-aspiration scale (P = .037), and oral and pharyngeal residue with thickened boluses (Nectar P < .001, Honey P < .001, and Pudding P < .001). In conclusion, oral exercise significantly improves the postoperative swallowing function of patients with oral cavity cancers.
Introduction
Although the introduction of novel surgical techniques and our expanding knowledge of radio-chemotherapy 1,2 have improved the outcomes for patients with head and neck squamous cell carcinoma (HNSCC), restricted food intake 3 remains a challenging concern in these patients. Because of disrupted swallowing physiology, 69% of advanced-stage patients with HNSCC suffer from aspiration, largely without symptoms, during the first year after treatment. 4 Nearly one-fourth of patients with HNSCC experience decreased swallowing function, even up to 5 years posttreatment. 5 These eating disabilities cause higher rates of pneumonia and malnutrition and can lead to miserable social and emotional losses. 6
In an effort to prevent aspiration and improve swallowing function in patients with HNSCC, various preventative and rehabilitative strategies have been introduced in recent decades, including dietary adjustments, 7,8 oral exercises, 9,10 tongue strengthening exercises, 11 swallowing maneuvers, 12 dental prosthetics, 13 and neuromuscular electrical stimulation. 14 Despite these options, a lack of uniformity and consensus remains regarding the best treatment strategy for treating dysphagia. An internet-based survey 15 in 2012 revealed that over 70% of institutions in the United States did not have a routine referral policy for patients with oral cancer.
Logemann noted that randomized clinical trials (RCTs) were the gold standard for studying the efficacy of dysphagia treatments. 16 Current RCTs have yielded increasing evidence supporting the use of various maneuvers and exercises for patients with HNSCC undergoing radiotherapy 17 and chemoradiotherapy. 11,18 –21 However, postoperative swallowing function has not been fully studied by well-structured clinical trials.
Surgical resection of primary oral cavity tumors is still considered the primary treatment modality according to the current National Comprehensive Cancer Network guidelines, 22 especially in Asian countries, where there is a much lower incidence of Human Papillomavirus-related oropharyngeal cancer. 23 Although a pilot study 24 suggested that range of motion exercises implemented during the first 3 months after oral cavity cancer resection could significantly improve swallowing function, there remains a lack of compelling evidence supporting the efficacy of swallowing therapy for postoperative patients.
In this RCT, we assessed the benefits of early postoperative oral exercises for oral and oropharyngeal patients with cancer. The exercises began within 3 weeks after surgery and continued for 3 months.
Patients and Methods
Trial Design
This was a single-institution, single-blind, randomized controlled trial performed in a tertiary medical center. The study was approved by the hospital's Institutional Review Board (CCH IRB No. 130409). Patient eligibility was assessed by the Head and Neck Multidisciplinary Oncology Team of Chang-Hua Christian Hospital.
Patients
Patients aged between 18 and 75 years with histopathologically proven oral or oropharyngeal squamous cell carcinoma who were prescheduled for an en bloc resection of the primary tumor, neck dissection, and reconstruction were enrolled in this study. Study participants were appropriate candidates for an early oral exercise program, which was defined as being able to try at least a thin liquid diet within 21 days after surgery. The ability to attempt oral intake was first determined by an experienced speech-language pathologist who was blinded to the study; the determination was then confirmed by the head and neck surgeon.
The exclusion criteria included patients who had received any previous treatments, previous head and neck carcinoma history, neurological or other nontumor-related swallowing difficulties, received a delayed oral diet (>21 days after surgery), or had received swallowing training before for any reason. Eligible patients were assigned to either the exercise or control group in a 1:1 ratio via computer-generated randomization.
Methods
The exercise group received instructions regarding oral exercises and standard care by an experienced head and neck clinical nurse specialist after postoperative oral intake was possible. The oral exercises included (1) range of motion exercises of the lips, jaw, and tongue 24 and (2) resistance exercises for the tongue. 25 The range of motion exercise involved extending the structure as far as possible, holding the posture for 1 to 2 seconds, then releasing it. Resistance exercise was performed by pushing a tongue blade against the tongue for 5 seconds while the tongue attempted to resist. 26 Both exercises were repeated 10 times in a session. The recommended frequency of exercise was 3 sessions per day for 12 weeks. The control group received instructions from the same nurse specialist regarding standard care, including proper swallowing positions 27 and proper food textures. Individual dietary counseling was conducted by a dietitian who was blinded to the study. Compliance in both groups was encouraged through weekly telephone advisement by the nurse specialist for 12 weeks.
Baseline swallowing function was assessed with modified barium swallow study (MBSS) 1 month after surgery. Postintervention MBSS results were analyzed 3 months later (4 months postoperatively). All MBSS were completed using a standard protocol, 28 including 1 or 2 swallows of 1 mL, 3 mL, and 10 mL of thin water, 10 mL of nectar-like thick liquid, 10 mL of honey-like thick liquid, and 10 mL of pudding-like thick liquid. A commercialized gum-based thickening agent, Resource ThickenUp Clear (Nestlé, France) was used to prepare the nectar-, honey-, and pudding-like thick liquids. The viscosity level of the thickened liquids was standardized according to the National Dysphagia Diet Task Force. 29 The boluses were mixed well with barium. Considering the risk of choking events and generally difficult airway management, the cookie bolus test is not performed among patients with acute postoperative head and neck cancer in our institution. All MBSS were analyzed carefully by a blinded speech-language pathologist using frame-by-frame and slow motion videos.
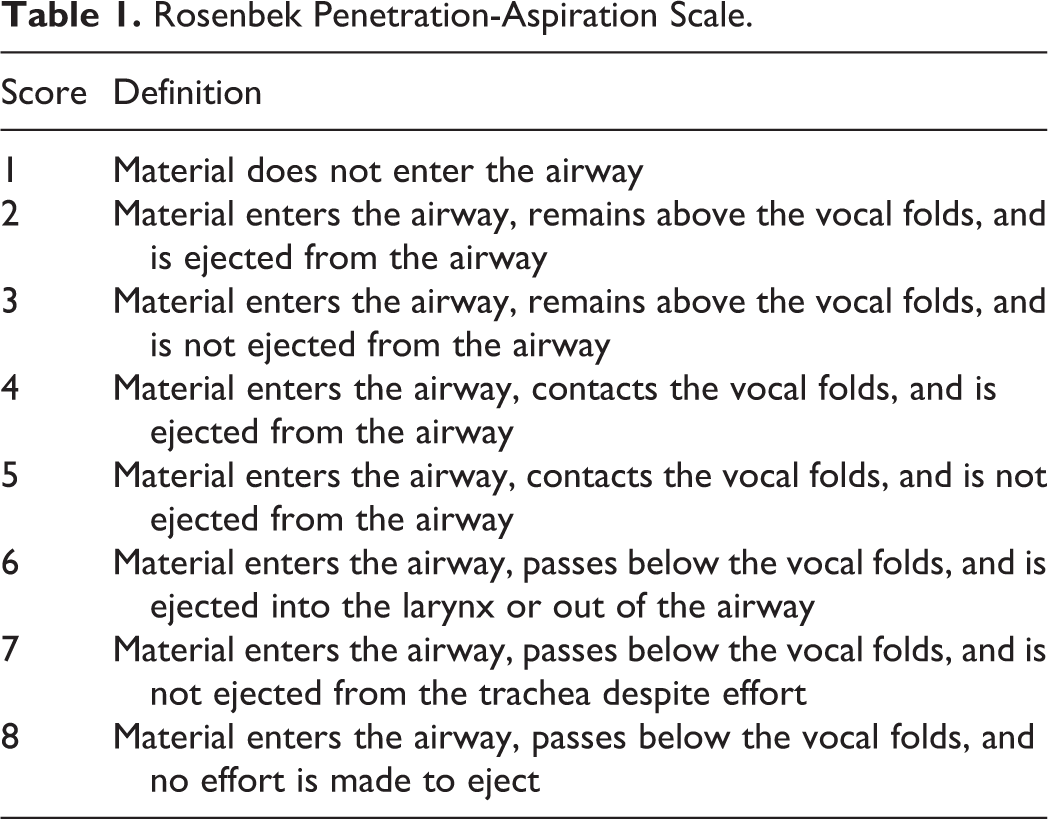
The Rosenbek penetration-aspiration scale, 30 as shown in Table 1, was used to assess the safety of swallowing. This scale is an 8-point, equal-appearing interval scale with good intra- and inter-rater reliability. The scores ranged from 1 point (no materials entered the airway) to 8 points (the material passed below the vocal cords, but no effort was made to eject the material), representing the severity of risk for aspiration and penetration.
Rosenbek Penetration-Aspiration Scale.
Because of the importance of sufficient oral nutrition and hydration, swallowing function was assessed by oral and pharyngeal residue examinations. Examples of oral residue and pharyngeal residue estimation are shown in Figure 1. Although it was impossible to quantify the exact amount of residue without performing scintigraphy, previous studies 31 have noted that the observations made by well-trained staff correlated well between MBSS estimation and scintigraphy.
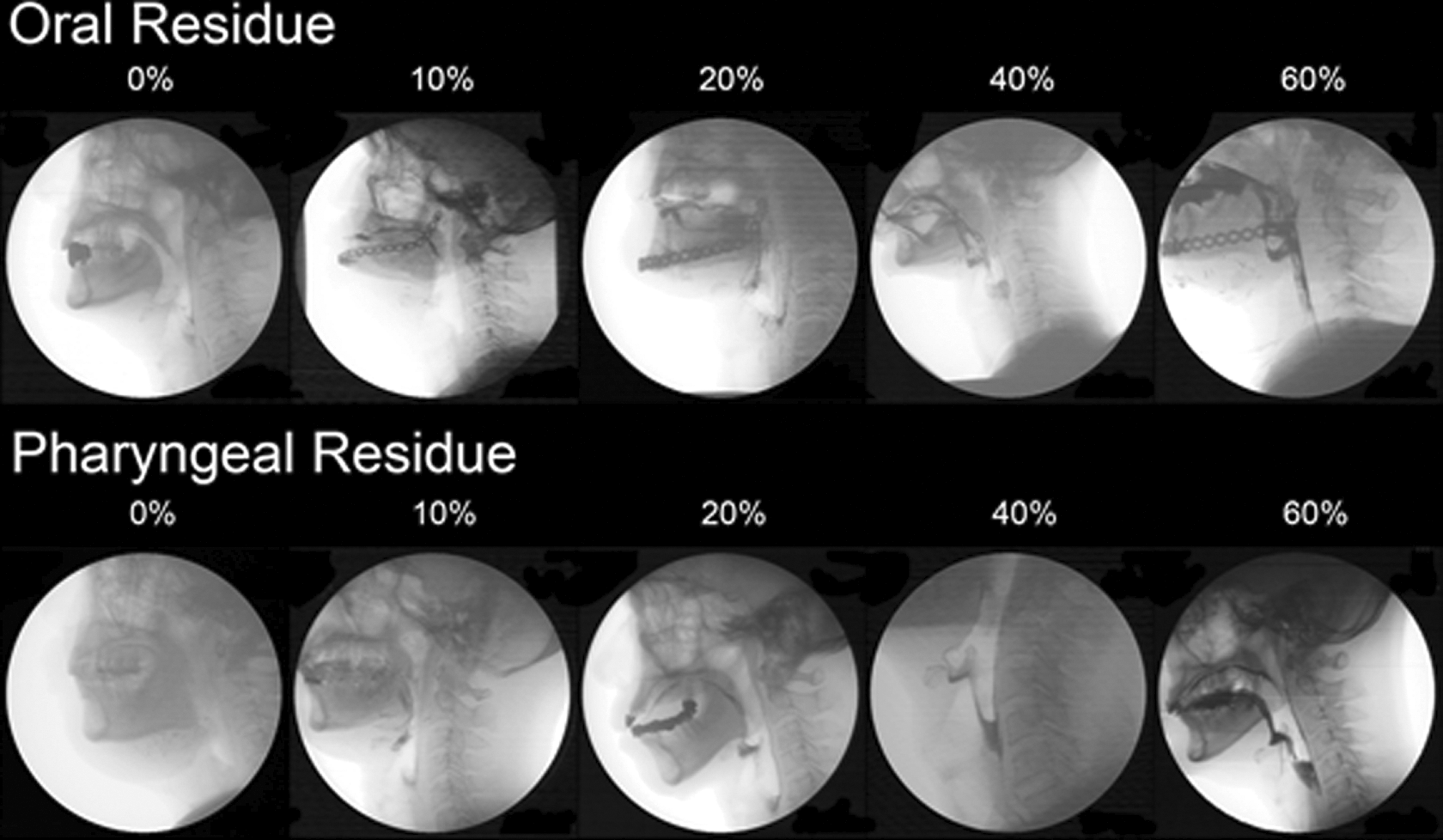
Examples of oral and pharyngeal residues. Examples of oral and pharyngeal residues in modified barium swallow examination were shown. Note that the residue amount was estimated from frame-by-frame and slow-motion videos in 3-dimensional structures. Photographs may not be able to represent the exact condition.
The primary outcome of interest was improvement on the Rosenbek penetration-aspiration scale. Secondary outcomes included improvements in oral and pharyngeal residue.
Sample Size
Based on the differences in Rosenbek penetration-aspiration scale scores and MBSS results, 2 groups of 20 patients were required to achieve an α level of .05 and a power of 80%. Estimating a withdrawal rate of 20%, 50 patients (25 patients in each group) needed to be enrolled in this trial to achieve the required sample size.
Statistical Analyses
Data were expressed as the means and standard deviations. All data were analyzed with the intention-to-treat approach. The differences in end points between the exercise and the control groups were compared with independent sample t tests. If the data were not normally distributed, the Mann-Whitney test was performed. Differences were considered to be significant when P <.05. Statistical analyses were performed using a commercially available statistical software, Medcalc, version 15.8 (MedCalc Software, Ostend, Belgium).
Results
Patients
Between January 2014 and January 2015, 50 patients were randomly assigned to either the exercise or control group before treatment. Demographic variables are shown in Table 2. Seventy-five percent of the tonsil cancer revealed p16 (-) in pathology result. Two patients in the exercise group and 3 patients in the control group were excluded from the study because they were unable to attempt oral intake within 21 days after surgery. Oral exercise training, feeding position education, and individualized dietary counseling were arranged for the patients. Three patients assigned to the exercise group and 2 patients assigned to the control group refused to undergo MBSS. Therefore, 20 patients were able to be analyzed in each group (Figure 2).
Baseline Characteristics by Study Group.
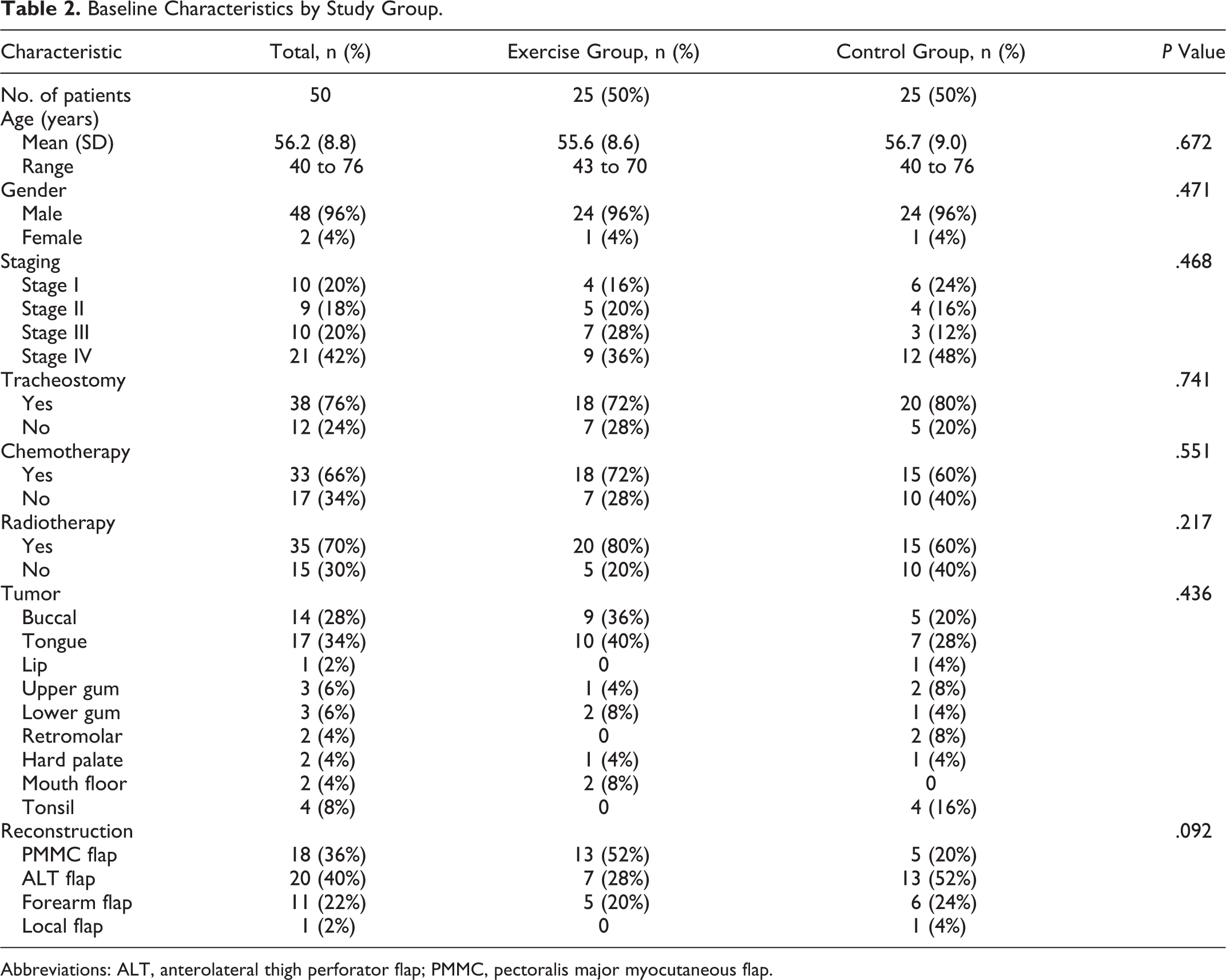
Abbreviations: ALT, anterolateral thigh perforator flap; PMMC, pectoralis major myocutaneous flap.
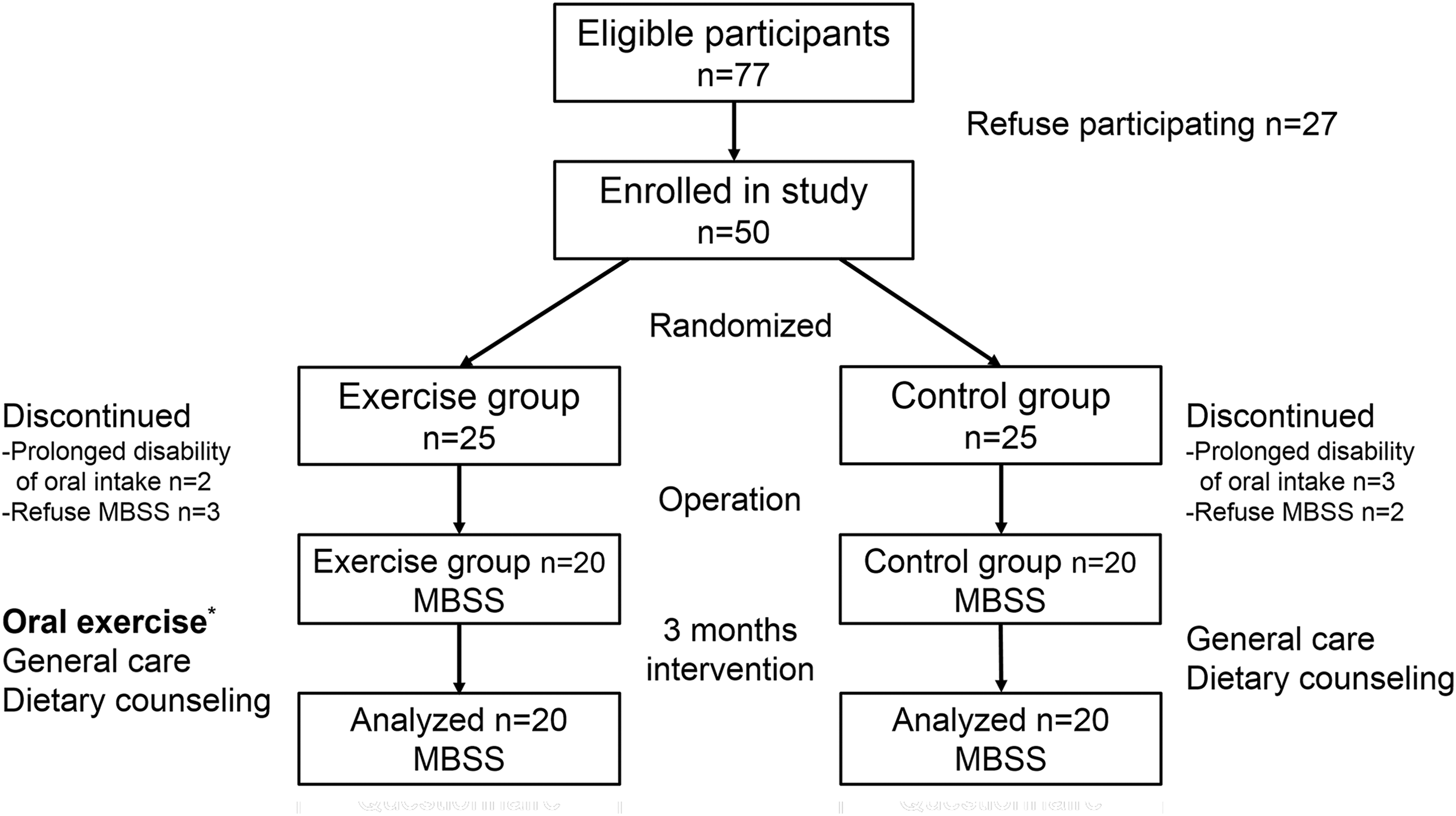
Flow diagram of patient randomization and analysis. *Oral exercise included range of motion exercise and tongue resistance exercise. MBSS indicates modified barium swallow study.
Rosenbek Penetration-Aspiration Scale
The mean values and standard deviations of the baseline scores, postintervention scores, and improvements in the Rosenbek Penetration-Aspiration scale (P-A scale) are presented in Table 3. A slight decrease in the P-A scale was observed in the control group (−0.15 [0.65]). Although similar baseline P-A scales were noted in both groups, a small but significant improvement was observed in the intervention group (P = .037), which suggests that patients may benefit from early postoperative oral exercise by decreasing the severity of aspiration.
Rosenbek Penetration-Aspiration Scale by Study Group.
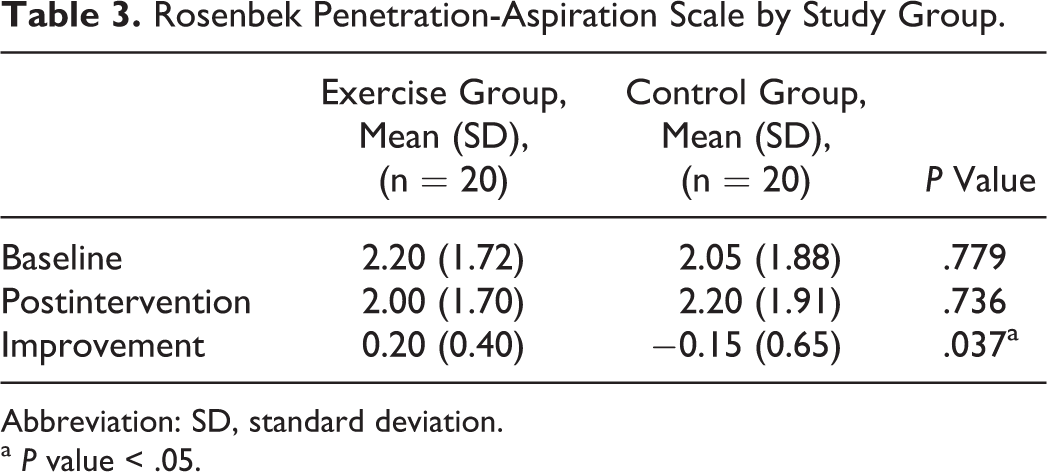
Abbreviation: SD, standard deviation.
a P value < .05.
Oral and Pharyngeal Residue
The amount of oral residue (6 different consistencies) was compared between the exercise and control groups (Figure 3A and Table 4). Because only small amounts of oral residue were observed when thin water was administered, no differences were noted between the groups. However, significant improvements were observed in the exercise group when nectar-like thick liquid (P < .001), honey-like thick liquid (P < .001), and pudding-like thick liquid (P < .001) were tested. As the texture of the bolus thickened, more pronounced improvements in the amount of oral residue were observed in the exercise group. Similar results were observed in terms of pharyngeal residue (Figure 3B and Table 4). These results were clinically important while modifying the texture of meal replacement shakes prepared for postoperative patients.
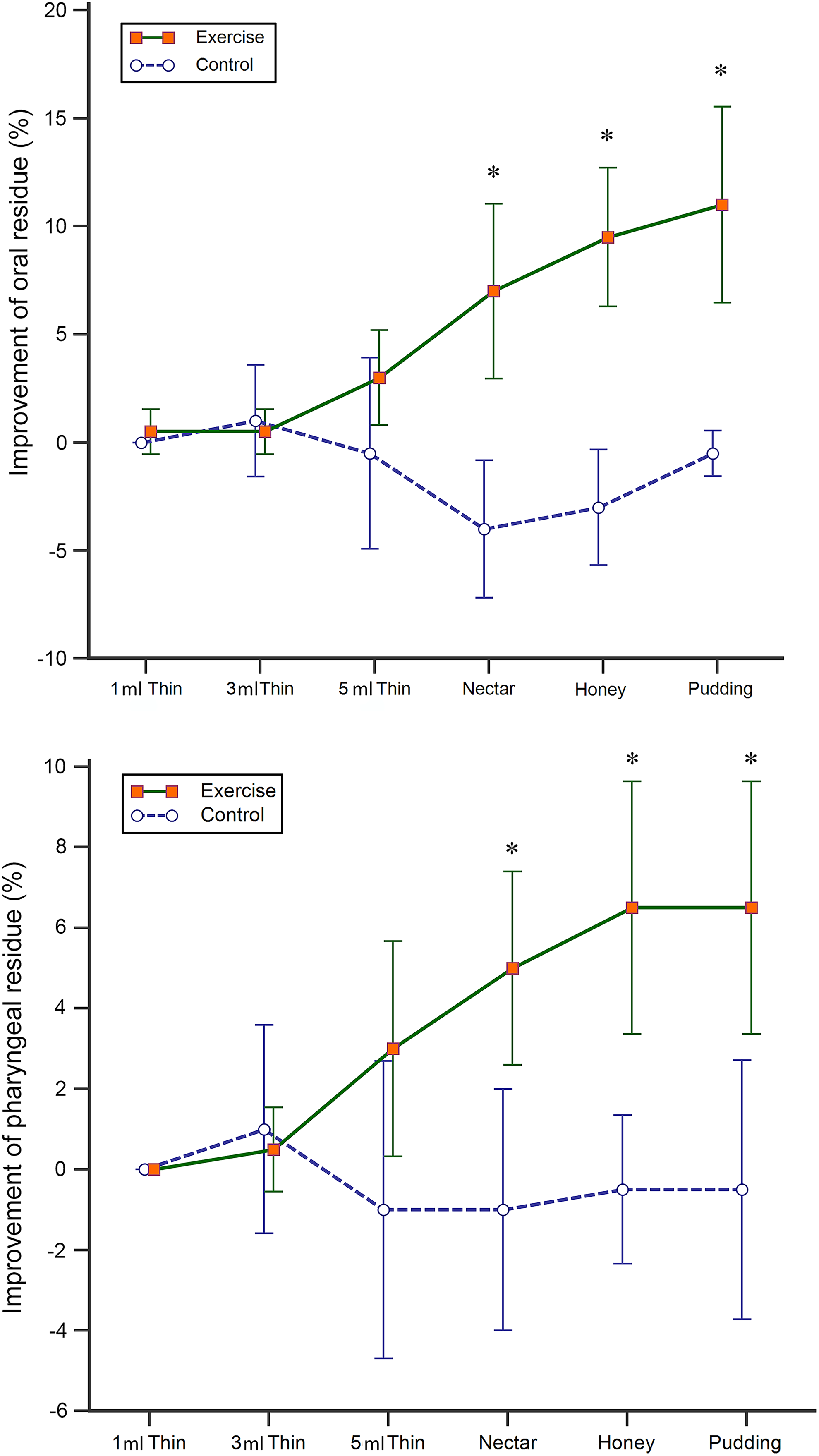
Improvement of oral and pharyngeal residue. Significant improvements of oral residue (A) were observed in the exercise group when nectar-like thick liquid (P < .001), honey-like thick liquid (P < .001), and pudding-like thick liquid (P < .001) were tested by modified barium swallow study. Similar finding was also noted when pharyngeal residue (B) was tested. Error bars represent the 95% confidence interval of the means. *P value < .05.
Oral and Pharyngeal Residue.
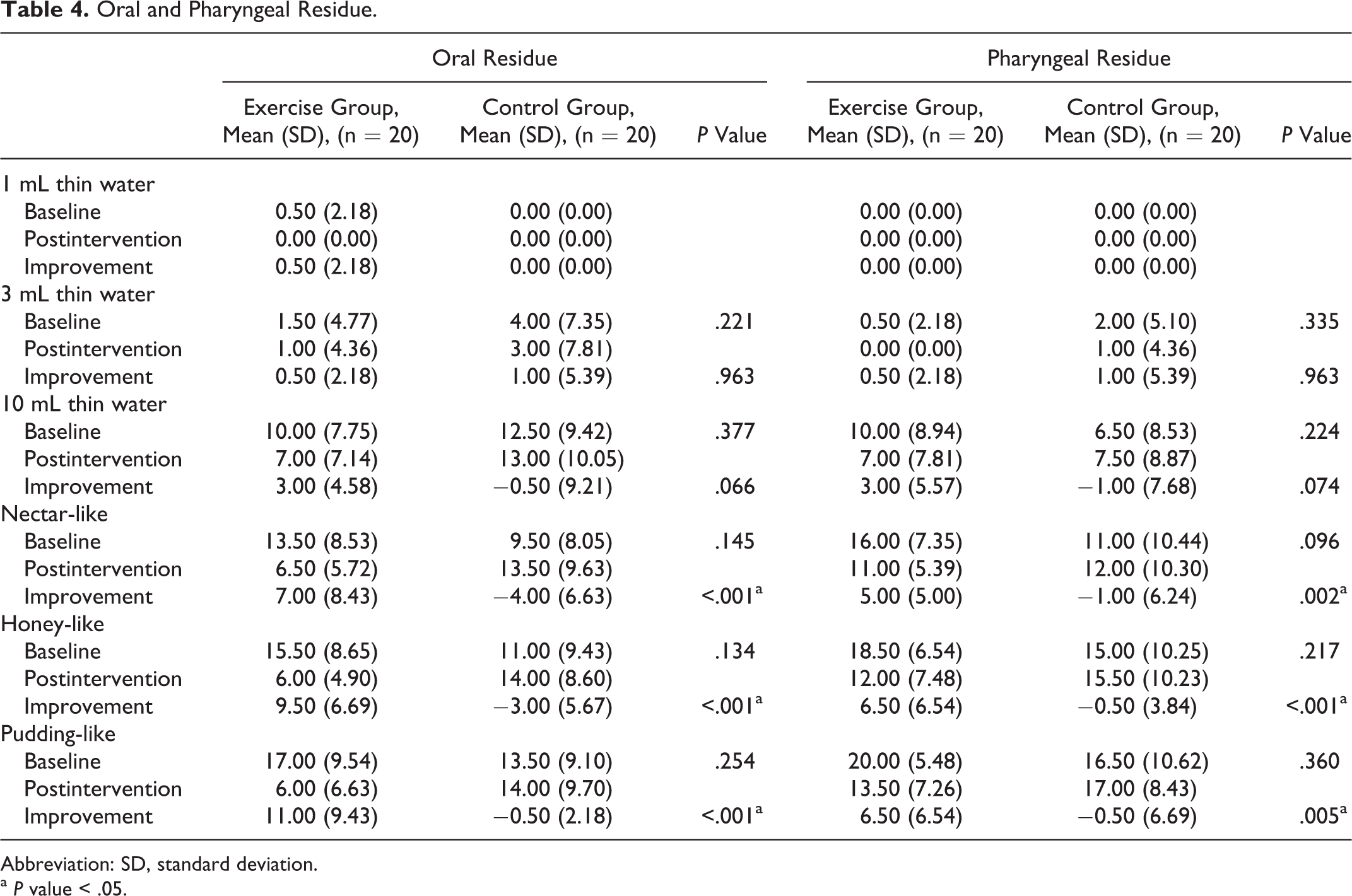
Abbreviation: SD, standard deviation.
a P value < .05.
Discussion
Although the importance of treating dysphagia in patients with head and neck cancer has been long acknowledged, there remains a lack of evidence 16 and consensus 15 regarding treatment recommendations and efficacy. This RCT was designed to determine the efficacy of postoperative oral exercise among patients with oral cavity cancer. Tongue resistance exercises potentially strengthened the remaining lingual muscle, which is critical for moving the food through the mouth and pharynx. Range of motion exercises prevented the formation of irreversible restrictive scarring and fibrosis. Thus, it was not surprising that oral exercises combining both rehabilitation plans yielded significant improvements in objective and subjective swallowing function.
Swallowing function is often already impaired preoperatively 32 and becomes even more compromised after surgery. 33 Resection of the functional organs and the bulky effect of the reconstruction flap influences the efficacy of swallowing. Concurrent chemo-radiotherapy, which is often utilized for patients with postoperative advanced-stage HNSCC, worsens the situation. In the pilot study by Logemann et al, 24 swallowing efficacy was reduced in postoperative patients who did not perform range of motion exercises and was significantly improved in the exercise group. In the current study, swallowing efficacy tests and the aspiration-penetration scale revealed a worsening trend in the control group, especially regarding the amount of oral residue following the administration of thickened boluses.
The assessment of aspiration by MBSS in the current trial revealed a small but significant improvement on the mean P-A scale in the exercise group. Compared to patients with laryngeal and hypopharyngeal cancer, patients with oral and oropharyngeal HNSCC experience fewer aspiration events. However, because our oral exercise protocol involved tongue resistance exercises, this result was expected. A recent study 34 using fiberoptic endoscopic evaluation of swallowing suggested that tongue motility and tongue strength correlated significantly with the rate of aspiration in patients with surgically treated HNSCC. Tongue resistance exercises improved the physiology of swallowing and therefore eliminated aspiration. 35 Other rehabilitation strategies, such as chin tuck positions and supraglottic swallowing maneuvers, have also been reported to be promising and may eliminate over 50% of the aspiration events among patients after oropharyngeal tumor resection. 36 The Mendelsohn maneuver, which prolongs hyolaryngeal elevation and cricopharyngeal opening during swallowing, is widely believed to have an even better effect on eliminating aspiration. 12,37
Due to their decreased ability to move food through the mouth cavity, increased oral and pharyngeal residues are often noted in postoperative patients. Residues not only increase the risk of bacterial growth but may also lead to aspiration. In a prospective study by Borggreven et al, 3,38 which included 54 oral and oropharyngeal patients treated by tumor resection and free flap reconstruction, revealed an average of 16% oral residue and 20% pharyngeal residue at 6 months posttreatment. Similar findings were observed by Pauloski et al 39 among patients undergoing tongue and mouth floor cancer resection. Both studies showed a lack of improvement during the follow-up and were comparable to our results in the control group. The RCT conducted by van der Molen et al 18 found significant improvements in the presence of residue among chemo-radiotherapy-treated patients with HNSCC who practiced range of motion and strength exercises. Similar improvements were also seen in our study, especially with boluses with a thickened consistency. On the other hand, only small amount of oral and pharyngeal residues was noted while swallowing thin liquid consistency in both groups (Table 4). This can explain why less improvements were noted with thinner consistency.
There were limitations in the present study. First, the sample size was too small for further subgroup analyses. The efficacy of postoperative oral exercise in patients with different tumor origin sites, different operation methods, and different reconstruction methods is potentially interesting. Although the present study was unable to answer these questions, future clinical trials should consider these factors. Second, whereas oral exercise resulted in significant improvement over 3 months, no long-term follow-up was arranged. However, in previous studies, speech and swallowing function at 12 months postoperatively was essentially unchanged compared to the measurements obtained at the 3-month follow-up. 40 Third, this RCT was not double-blinded. It was difficult to blind the researchers because they provided the interventions to the patients. Designing a double-blind trial is not feasible in this situation.
Conclusion
This RCT provided compelling evidence for how to treat dysphagia in patients with postoperative oral cavity cancer. Compared to the control group (only standard care and individual dietary counseling), the patients who performed additional early postoperative oral exercises demonstrated significantly improved P-A scale scores and a reduction in oral and pharyngeal residues. Greater improvements in oral and pharyngeal residues were observed with thicker boluses. Oral exercise clearly improved swallowing function in patients who had been surgically treated. More tumor-location-specific and surgical-method-specific RCTs will be necessary to add to our best evidence for treating swallowing difficulties among patients with postoperative HNSCC.
Footnotes
Author Contribution
Ching-Chi Hsiang and Andy Wei-Ge Chen contributed equally to this work.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.