
Abstract
Branchial cleft cyst (BCC) most frequently arises from the second branchial cleft and is located anterior to the sternocleidomastoid muscle at the mandibular angle. However, very rarely, this may occur in the parapharyngeal space. Interestingly, the parapharyngeal BCC is frequently misdiagnosed as a peritonsillar abscess. In this study, we reported 2 cases of parapharyngeal BCC misdiagnosed as peritonsillar abscess.
Introduction
A branchial cleft cyst (BCC) results from the failure of the involution of normal embryological structures. There are 4 types of BCCs. 1 The second BCC represents approximately 95% of all the branchial cleft abnormalities. 2 The second pharyngeal arch forms the cervical sinus of His by overgrowing the second, third, and fourth branchial clefts. Incomplete closure of this sinus causes problems anywhere along its embryological tract, resulting in the creation of a fistula or cyst. 1 This cyst or fistula tract extends from the anterior border of the sternocleidomastoid (SCM) muscle, travels between the internal and external carotid arteries, passes superficially across the XI and XII cranial nerves, and terminates at the posterior part of the tonsillar fossa. 3,4 Therefore, second BCCs are most commonly found along the anterior border of the upper portion of the SCM muscle and next to it. Sometimes, BCCs appear anywhere along the path of a second branchial fistula, which runs from the lateral neck skin, between the internal and external carotid arteries, and into the palatine tonsil. 5,6 They can also appear in the lower neck, parotid, posterior triangle, or rarely, in the parapharyngeal space (PPS).
An isolated BCC in the PPS extending into the retropharyngeal space very rarely occurs; only 25 cases have been reported in the literature. These cysts develop inward in the soft-tissue plane, eventually protruding into the oropharynx. 4 The PPS is divided into the pre- and post-styloid spaces by the styloid process. 7 Tumors in the pre-styloid space are mostly salivary tumors. However, tumors in the post-styloid space are more likely to be neurogenic tumors or vascular neoplasms. 8 Tumors within the PPS grow slowly and painlessly. Cystic lesions in the PPS are frequently difficult to diagnose clinically and should be distinguished from schwannomas or salivary gland cancers. Complete surgical removal is required for differential diagnosis of the mass.
Interestingly, parapharyngeal BCCs are frequently misdiagnosed as peritonsillar abscesses. When a branchial cleft cyst becomes infected, it causes clinical symptoms. 7 The physician may need to differentiate between a peritonsillar abscess and a parapharyngeal cystic lesion. Clinically, a patient with a peritonsillar abscess presents with fever and a medially displaced palatine tonsil due to abscess formation. Resolution of the above symptoms of a peritonsillar abscess is usually seen after aspiration or incision and drainage. 6,7
In this study, we reported 2 cases of parapharyngeal BCCs misdiagnosed as peritonsillar abscesses.
Subjects
Two patients, a 67-year-old woman and a 43-year-old man, were referred to our department complaining of sore throat, intermittent fever, and trismus. They had been diagnosed with peritonsillar abscesses at a local clinic and received incision and drainage (I&D) but it recurred several times and eventually, the patients received tonsillectomies at another hospital. Upon physical examination, the left posterolateral wall of the oropharynx showed swelling (Figure 1). The swelling almost approached the midline of the pharyngeal wall. Initially, these masses were suspected to be recurring peritonsillar or parapharyngeal abscesses. The oropharyngeal swellings were palpated, fluctuant. Needle aspirations were performed in both patients and serosanguinous fluids were identified. We subsequently checked the neck computed tomography CT images, which showed cystic masses of about 5- and 4-cm sizes in the left PPS (Figure 1). The cytologic findings of the aspirated fluids indicated inflammatory cells. We decided to remove the masses via the intraoral approach for definitive diagnosis. Upper: Axial (A) and coronal (B) section of CT images (case 1) showing a 4 × 3 cm cystic mass in the left parapharyngeal space. Endoscopic images showing swelling of the posterolateral area of the oral cavity (C). Lower: Axial (A) and coronal (B) section of CT images (case 2), and endoscopic images showing swelling of the posterolateral area of the oral cavity (C).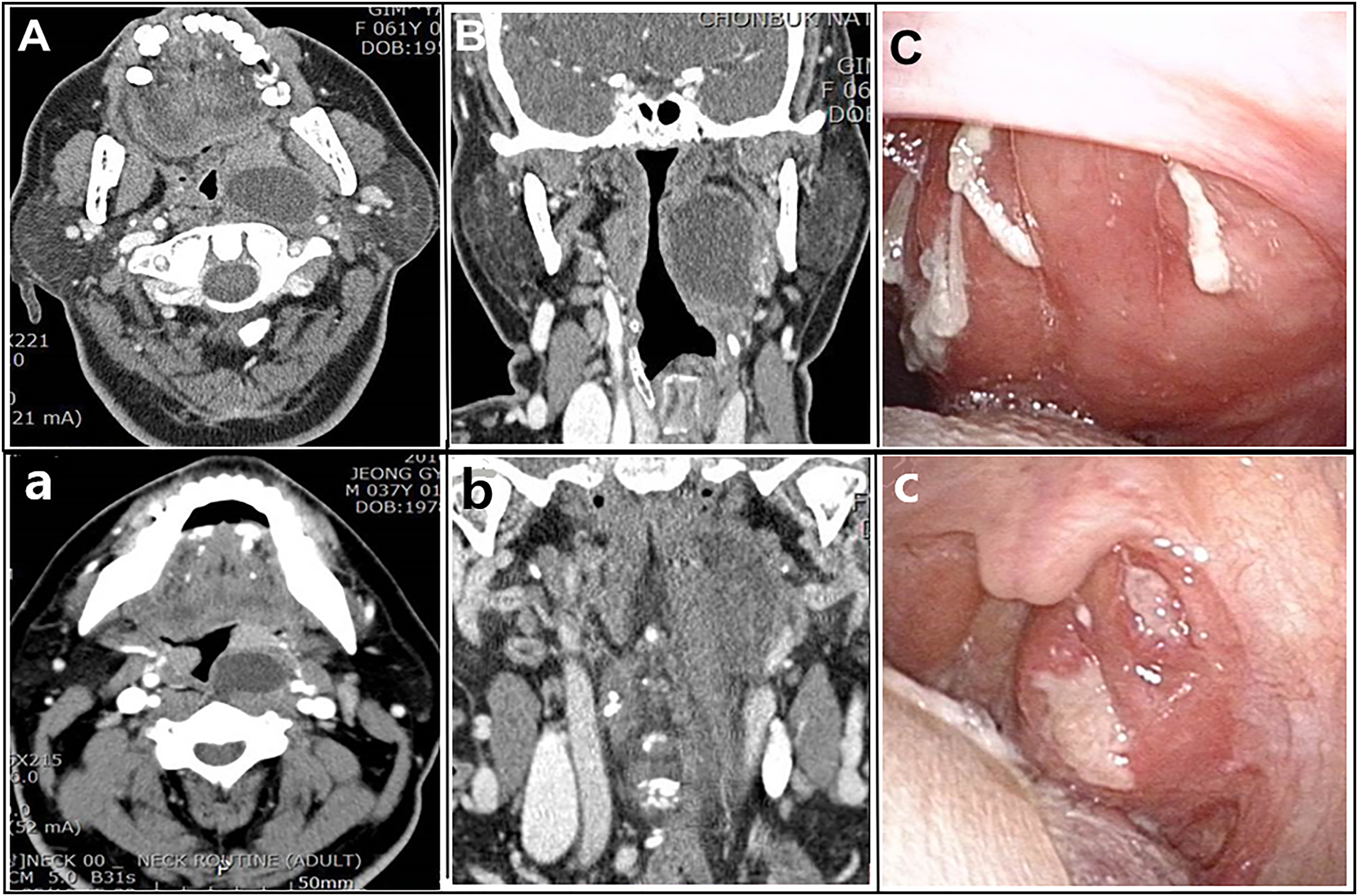
In the first case, we attempted to remove the mass under general anesthesia. We equipped the operating microscope with a CO2 laser. An encapsulated cyst was sited deeply in the PPS and tightly adhered to the surrounding tissues. Intraoperatively, a laser incision was made on the lateral surface of the cystic mass after lateral retraction of the tonsillar pillar (Figure 2). The cyst capsule was opened with the CO2 laser with a tonsil dissector and cystic fluid was evacuated. The cystic capsule was grasped medially and the lateral part of the cystic wall was carefully dissected using laser vaporization. Laser dissection of the cyst was performed close to and along the cystic capsule to protect the neighboring structures. After full dissection of the cyst, bleeding control was done. The retracted mucosa and muscle of the posterior pillar of the left tonsil was repositioned to the posterior pharyngeal wall (Figure 2). Postoperative CT images and endoscopic images showed no evidence of recurrence. The patient complained of mild discomfort while swallowing, but the symptom was tolerable. Intraoperative images showing the complete dissection of the cystic mass (A) and control of bleeding in the surgical bed (B). The posterior cystic wall was sutured to the posterior pillar (C) after exposure of the cystic wall and the anterior cystic wall was sutured to the anterior tonsillar pillar. (D) Postoperative findings in the oral cavity and histologic findings of the cyst ((1) ×20 and (2) ×400).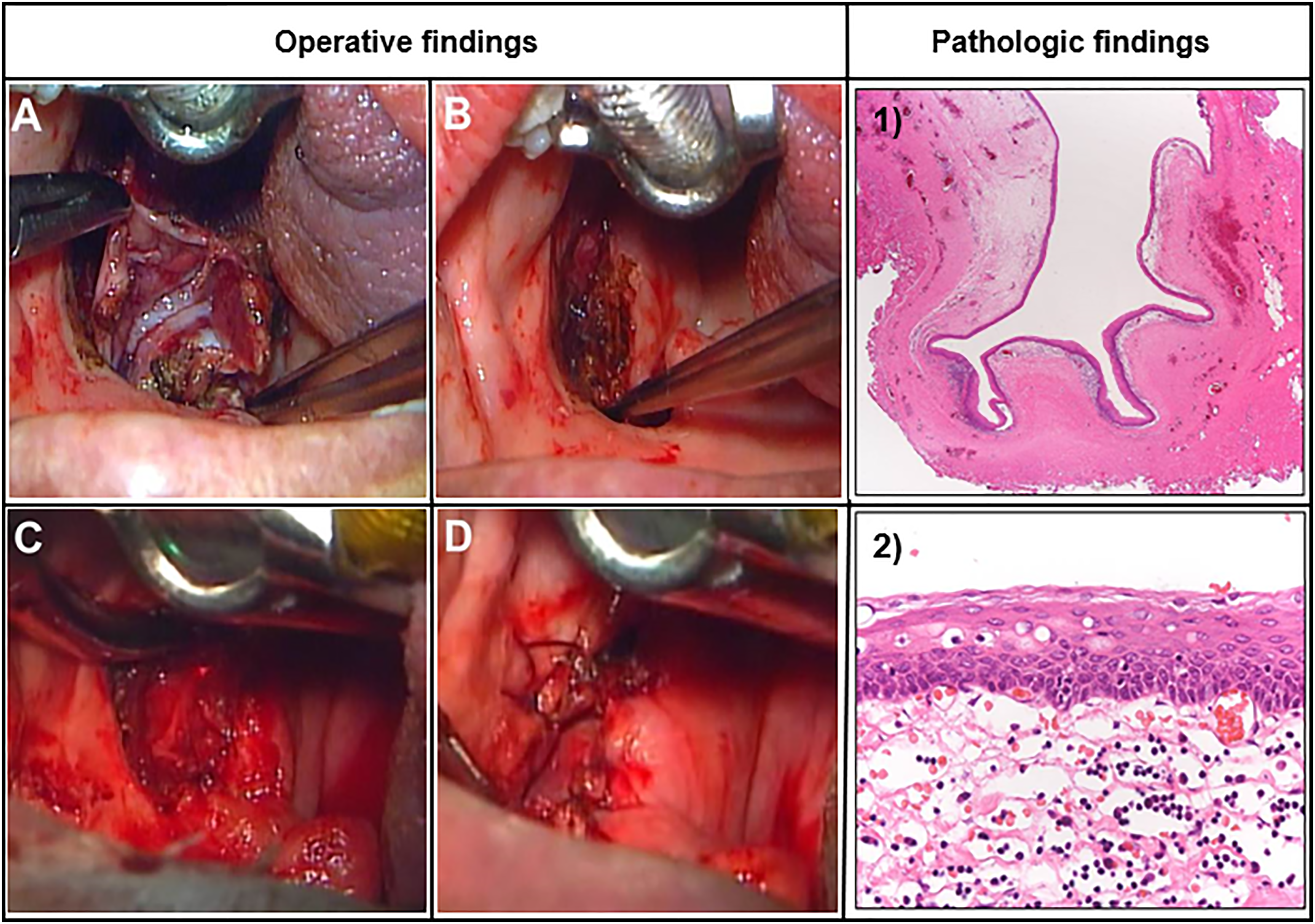
In the second case, we also equipped the operating microscope with a CO2 laser. An encapsulated cyst was sited deeply and very tightly adhered to the surrounding tissues due to the previous tonsillectomy. The cyst capsule was opened with a CO2 laser and cold instruments. The cystic capsule was grasped medially, but it was difficult to dissect due to severe adhesion. We decided to marsupialize the capsule in an attempt to avoid carotid artery injury. After identifying the cystic wall, the posterior wall of the cyst was sutured to the posterior tonsillar pillar, and the anterior cystic wall was sutured to the anterior tonsillar pillar (Figure 2). There was no evidence of recurrence. In the histologic findings, the cyst was lined with stratified squamous epithelium and supported by fibrous stroma. The findings were consistent with a branchial cleft origin (Figure 2).
Discussion
Tumors in the PPS are uncommon, at about .5% of all head and neck tumors, and are predominantly benign (70–80%). 2,3 They often enlarge slowly and painlessly. The most common neoplasms in the PPS are pleomorphic adenomas. Cystic lesions in the PPS have a range of possible origins due to their various anatomic structures. The cystic degeneration of a pleomorphic adenoma is very rare and is easily differentiated from a parapharyngeal BCC. The second most common cystic tumor in the PPS is neurogenic tumors, mostly schwannomas with cystic degeneration. Other common lesions with a cystic component in the PPS are the lymphatic metastasis of squamous cell carcinoma or papillary thyroid carcinoma, lymphangiomas, and lymphomas. 8
A second BCC is a common lateral neck mass arising anterior to the sternocleidomastoid muscle at the mandibular angle. However, they rarely occur in the PPS. Isolated parapharyngeal BCCs have rarely been reported and are often difficult to diagnose clinically. Parapharyngeal BCCs are frequently confused with peritonsillar abscesses, as in our cases. In the patients in this report, we initially misdiagnosed isolated parapharyngeal BCCs as simple peritonsillar abscesses.
Preoperative evaluation for a differential diagnosis and surgical planning is essential. Neck CT and magnetic resonance (MR) images are available for evaluating masses in the PPS. On CT images, a parapharyngeal BCC presents as a low-density, well-demarcated cystic mass with a thin wall and without septations. 9,10 However, MR images have more advantages than CT images for delineating the soft-tissue characteristics of PPS masses. The cystic content appears hyper-intense in the T1-weighted images on MRI and no enhancement of the cyst is detected with contrast. 9
A parapharyngeal BCC requires complete surgical removal to confirm the diagnosis and proper treatment. Various approaches can be taken for PPS masses including the transoral, transcervical, transcervico-parotid, and mandibulotomy approaches. The transoral approach is generally accepted for small benign neoplasms in the pre-styloid PPS when they present as an oropharyngeal mass. Practically, the transoral approach sometimes has a limitation with minimal exposure of the surgical field. 7-10 Therefore, when the masses are large and not mobilizing well during dissection, a combined transoral and transcervical approach needs to be taken. Lesions in the post-styloid PPS also need a transcervical approach for better exposure. This transcervical approach can also be combined with a transparotid approach for tumors from the deep lobe of the parotid gland. In this approach, the superficial parotidectomy is usually performed after identification and preservation of the facial nerve. The transcervical approach could be combined with mandibulotomy when improved access to the skull base is needed. 10 In this report, we used a CO2 laser because the cystic mass and other deeper structures were not well dissected with cold instruments. We also used an operating microscope for better visualization and careful dissection of the cyst from important adjacent structures.
Conclusion
Parapharyngeal BCCs are very rare lesions that need to be differentiated from other cystic neck masses in adults. A comprehensive understanding of the complex anatomy and embryology is essential for proper management. Finally, to confirm the diagnosis with permanent pathology and histological evaluation, this type of cystic parapharyngeal mass must be surgically resected. In this study, we attempted the intraoral dissection of lesions using a CO2 laser and operating microscope. This approach has benefits in providing good surgical visualization and preserving important adjacent structures while dissecting the cyst.
Footnotes
Acknowledgments
This paper was supported by Fund of Biomedical Research Institute of Jeonbuk National University Hospital.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.