
Abstract
Introduction
Olfactory dysfunction has been included among the early symptoms of coronavirus disease (COVID-19). Evidence suggests that a relationship exists between the duration of olfaction disorders and the probability of developing severe COVID-19. Given the scope of the COVID-19 pandemic, this study aimed to determine the frequency of smell alteration and its association with the severity of COVID-19 in a referral hospital in Peru, which is one of the most affected countries in the Latin American region.
Materials and Methods
This study was an observational, prospective cohort study that included patients with COVID-19 who were treated at the Hospital Nacional Edgardo Rebagliati Martins from August to November 2020. To assess the association, the chi-square test of independence or Fisher’s exact test was performed. The outcome variable was COVID-19 severity, and the exposure variable was olfactory dysfunction. The first data collection was in the emergency department and the follow-up was via telephone.
Results
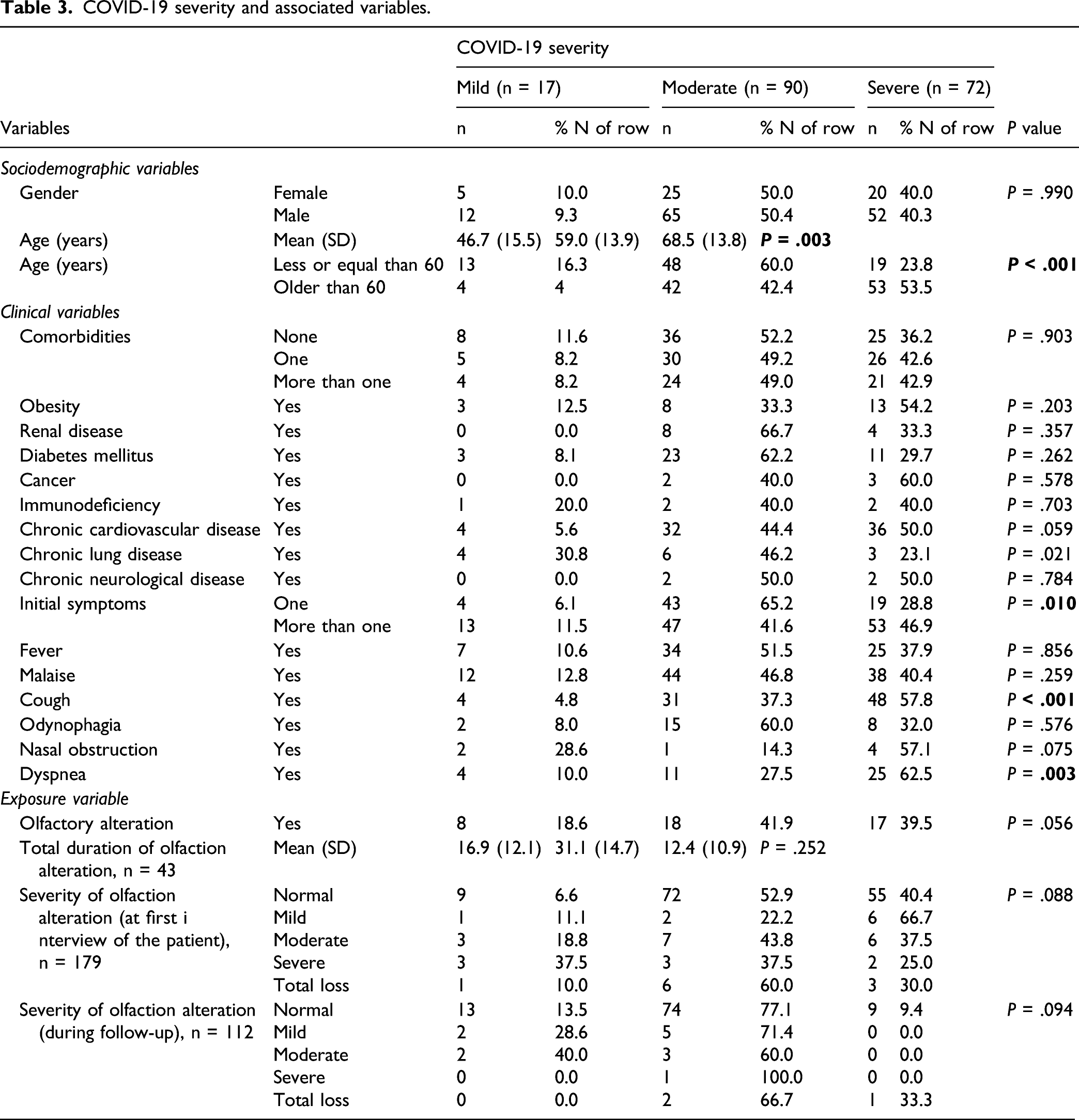
A total of 179 patients were included. The mean age was 61.6 ± 15.5 years, and 129 patients (72.1%) were male. Olfactory dysfunction was observed in 43 patients (24%). An inverse association was found between age and olfactory dysfunction (P = .002). No significant association was found between COVID-19 severity level and olfactory alteration (P = .056). However, a direct association was found between COVID-19 severity and age (P = .003), cough (P < .001), and respiratory distress (P = .003).
Conclusion
This study did not find any association between the severity of COVID-19 and olfactory dysfunction. It showed a low incidence rate of smell alteration compared with studies from other regions. Moreover, smell alteration was associated with younger age.
Introduction
Coronavirus disease (COVID-19), caused by the SARS-CoV-2, has continued to spread since December 2019. There have been more than 160 million cases and more than 3 million deaths globally (as of May 16, 2021). 1 The United States has the highest number of cases and mortality. Latin America has the highest health burden because of the inconsistency and inadequacy of specialized diagnosis and treatment, which is associated with a fragile economy and healthcare system. 2
The initially reported symptoms of COVID-19 included fever, cough, dyspnea, and malaise. Over time, smell alteration has been included among the early symptoms of the disease, and it has a prevalence between 29.6% and 75.2%.3,4 Evidence suggests that there is a relationship between the duration of olfactory disorders and the probability of developing severe forms of COVID-19. 5 However, most studies have been retrospective, involved outpatients, and were limited to mild stages of COVID-19; moreover, only a few studies included the Latin American population.3,6 Therefore, studies are still lacking on the association between olfactory disorders and COVID-19 severity.7,8
This study aimed to establish the initial symptoms of COVID-19 and consider smell alteration as an important screening factor for COVID-19 severity, to establish new clinical–epidemiological behaviors that may affect the management and care of the affected population. The information collected in this study will be useful as more cases are extended to the community and as external consultations are reopened by different health providers. The presence of olfactory alteration could serve as part of the screening for initial diagnosis and could be used to establish severity criteria during the initial triage of patients; this will allow us to optimize our health services and facilities during the COVID-19 pandemic. Given the scope of the COVID-19 pandemic, this study aimed to determine the frequency of olfactory alteration and its association with COVID-19 severity in a referral hospital for COVID-19 in Peru, which is one of the most affected countries in the Latin American region. 9
Materials and methods
Study design and population
This was an observational, prospective cohort study that included patients with a COVID-19 diagnosis and treated at the COVID-19 emergency service of Hospital Nacional Edgardo Rebagliati Martins (HNERM) from August to November 2020. COVID-19 diagnoses were obtained using rapid tests (IgM/IgG) or molecular tests (RT-qPCR). All patients had respiratory symptoms and were older than 18 years. Pregnant patients; patients with neuropsychiatric diseases; and those who had olfactory disorders, sinonasal pathologies, or sinonasal surgeries were excluded. HNERM provides care to social security (EsSalud) patients and serves as a third-level referral center for COVID-19 patients nationwide. All patients were diagnosed and treated according to the COVID National Guideline issued by the Peruvian Health Ministry. 10
Sample size calculation
The formula for survival analysis was adjusted to the variance inflation factor (to other factors correlated with severity). A proportion of those exposed to a study factor of 85% 11 with a 95% confidence level was considered. We consider .28 as the highest correlation coefficient between the study factor (anosmia), and all the included variables. Consequently, the sample size was set as 174 and was by convenience.
Procedures
Data collection was performed in 2 stages. The first stage was performed in the COVID-19 emergency service, from August to October, where sociodemographic and medical variables and information on olfactory alterations were obtained. These data were obtained using a collection form and questionnaires designed by the researchers. All patients participating in the research provided informed consent prior to data collection. The second stage was performed after the third week of the initial emergency care. The researchers contacted patients with a positive COVID-19 result, their family members, or an authorized contact person by telephone. A follow-up questionnaire was used to record the appearance (if they had not been present during their first evaluation in the emergency service) and duration of the olfactory alterations, and the severity of COVID-19 (Figure 1). Study flowchart.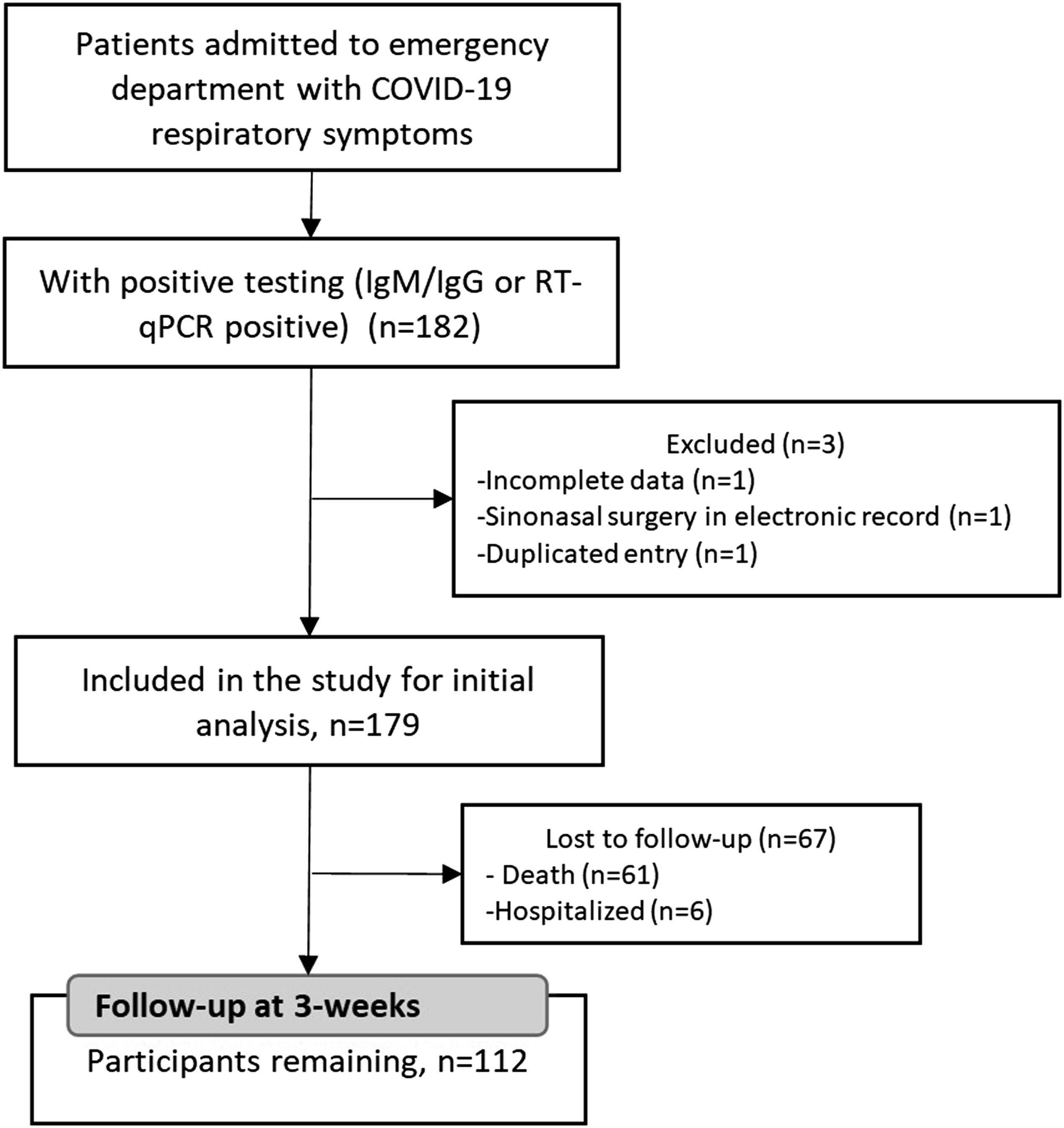
Variables
Regarding severity, a mild case was defined as a patient who required less than 48 hours of emergency observation/hospitalization; a moderate case, a patient who required more than 48 hours of emergency observation/hospitalization; and a severe case, a patient who needed admission to the intensive care unit (ICU) or died during treatment. 11 The alteration of olfaction was defined according to the patients’ response to the following question: How would you consider your sense of smell today? The alternatives were normal, mild, moderate, severe, or a total loss of smell. The total duration of olfactory alteration was considered, as well as whether it was the first symptom that presented during the evolution. The other symptoms considered were fever, general malaise, cough, odynophagia, nasal obstruction, and respiratory distress. Sociodemographic variables, such as sex, age, and comorbidities (cardiovascular diseases, diabetes, neurological, nephrological, pulmonary, obesity, cancer, and immunodeficiency) were evaluated by reviewing medical records. Owing to the number of comorbidities, a new variable was created according to the number of comorbidities present in the patient (none, one, or more than one comorbidity).
Statistical analysis
The collected data were tabulated in an Excel spreadsheet and then exported to SPSS 24.0 (IBM, Armonk, NY, USA) for analysis. Descriptive statistics were used for qualitative variables by using absolute and relative frequencies. For quantitative variables, the mean and standard deviation were used. To assess the association, the chi-square test of independence or Fisher’s exact test was performed.
Ethical aspects
All study participants signed informed consent forms and showed agreement for subsequent follow-ups by telephone. The data collected were codified and duly protected to guarantee the confidentiality of the information and the results of the patients. The study was approved by the research committee and ethics committee of HNERM.
Results
Sociodemographic and clinical characteristics (n = 179).
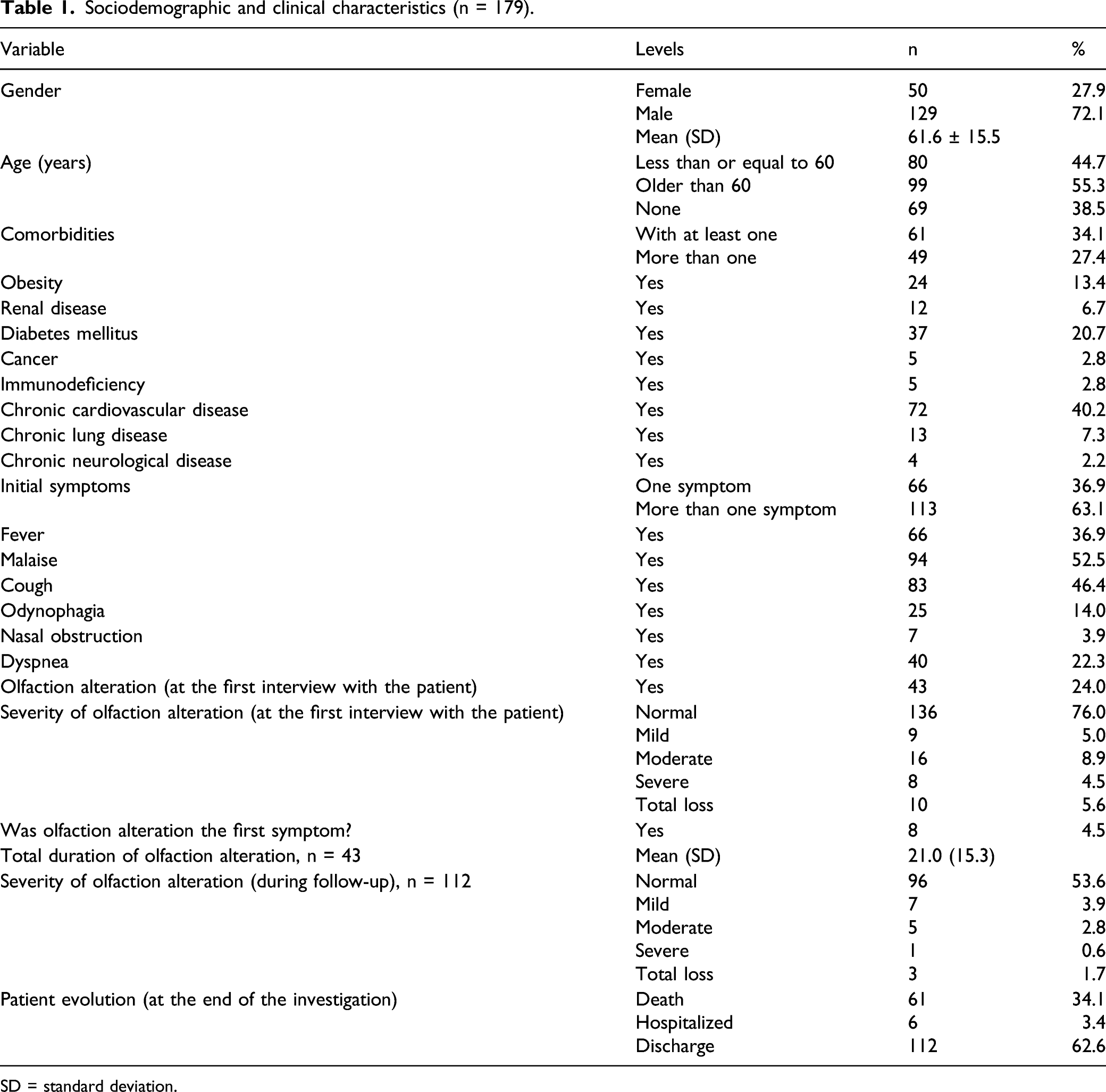
SD = standard deviation.
Regarding the severity of COVID-19, 17 cases (9.5%) were mild, 90 (50.3%) were moderate, and 72 were (40.2%) severe. However, in the follow-up, it was noted that 61 patients (34.0%) had died, and 6 (3.5%) were hospitalized. These accounted for 17 (15.2%) mild cases, 86 (76.8%) moderate, and 9 (8.0%) severe cases during the follow-up. Therefore, the final state of their smell could not be determined. The most frequent symptoms were general malaise (52.5%), cough (46.4%), and fever (36.9%). Nasal obstruction was found in 3.9% of patients (Table 1).
Differences with olfactory alteration (at the first interview with the patient).
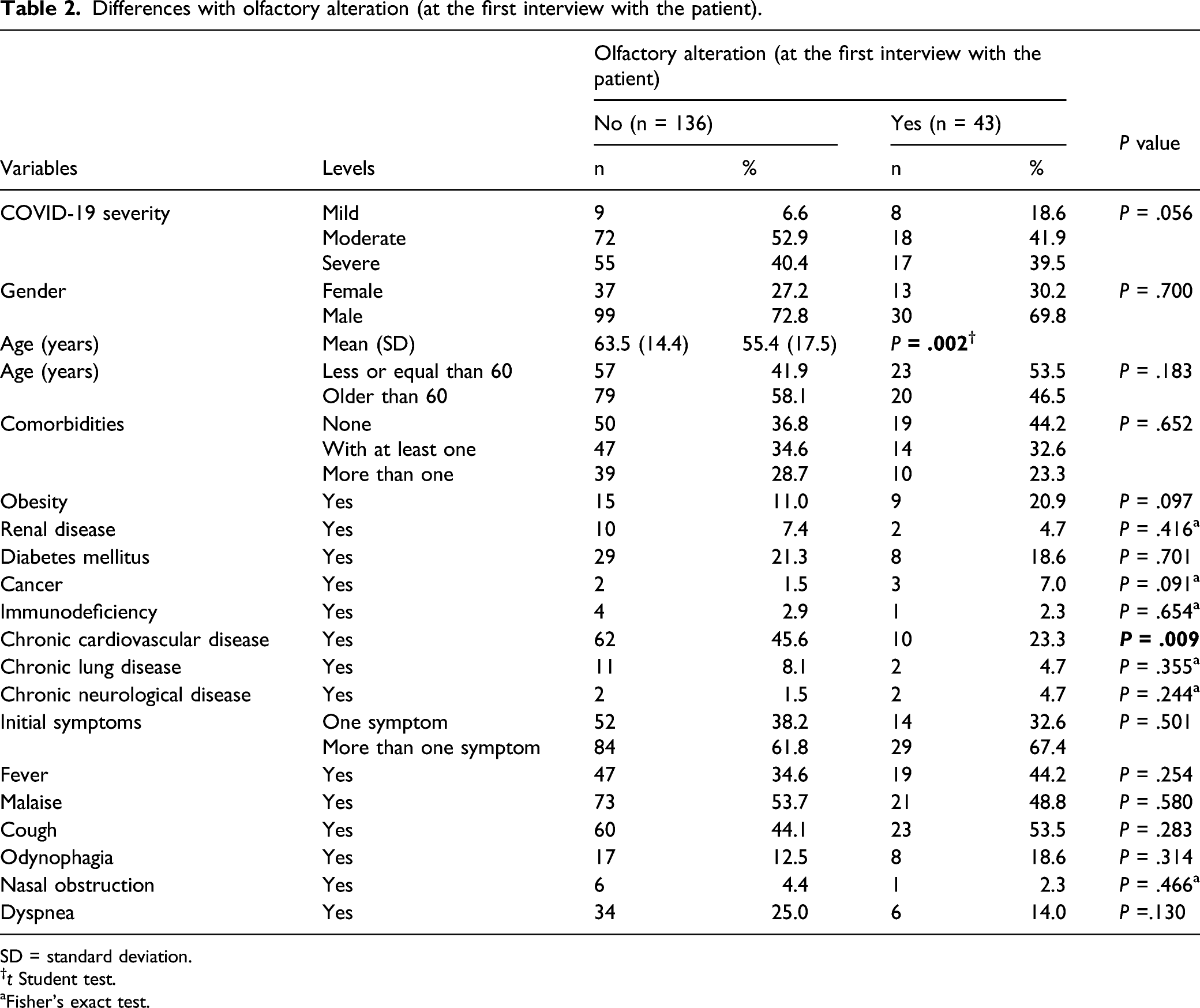
SD = standard deviation.
†t Student test.
aFisher’s exact test.
In terms of age, we found that there is an inverse association between this variable and the presence of olfactory dysfunction (P = .002). We also found an association between hyposmia and chronic cardiovascular disease (P = .009) (Table 2).
COVID-19 severity and associated variables.
Discussion
Main results
We found that approximately 1 in 4 patients had olfactory alteration at the start of enrollment, and that four of 10 patients had severe COVID-19. However, no association was found between the alteration of smell and the severity of COVID-19. To our knowledge, this is the first prospective study that was conducted in a Latin American population and included patients affected during the first wave of the COVID-19 pandemic in Peru. These findings are relevant and allow for comparisons with studies conducted in other regions.
Comparison with previous studies
The frequency of olfactory alteration in our study was 24%, which is considerably lower than the frequency reported in other countries in North America (66.8%) and Europe (31.2%) but higher than the frequency reported in Asia (14.9%).6,12,13 In Latin America, this frequency of olfactory alteration is less than the 36.1% reported in Ecuador 14 but is similar to that described in Argentina (23.9%). 15 Because the initial data collection was in the emergency department, we did not use psychophysical testing, but a subjective assessment. Nevertheless, our sample showed a low prevalence of olfactory dysfunction. One explanation is the high number of hospitalized patients with moderate and severe forms of COVID-19 compared with the number of patients with mild COVID-19. Some of the studies that evaluated the association between olfactory dysfunction and COVID-19 severity were conducted in patients with mild COVID-19 or outpatients3,11 or were conducted in a cross-sectional or retrospective manner; this approach leads to significant heterogeneity in the results. 6 However, the current study was prospective and performed in hospitalized patients, thus adding to the novelty of our findings.
A second explanation for the low prevalence of olfactory dysfunction is the SARS-CoV-2 variant in the region. A meta-analysis that included 38,198 patients found a prevalence of olfactory alteration of 43%. The meta-analysis only had 1 Brazilian study representing South America (n = 125). They found that patients of Caucasian origin had a 3 times higher prevalence of chemosensory dysfunction (54.8%) than Asians (17.7%). 16 This finding could be explained by the predominance of SARS-CoV-2 variants in each region. Type A and C variants are predominant in Europe and North America, whereas the type B variant is predominant in Asia. 17 In Peru, the Asian variant was the predominant variant during the first wave of COVID-19. However, 3 variants with different subtypes have been identified so far during the pandemic. 18 From the 1094 samples processed for a genomic sequence in Peru during 2020, only 12 were gamma variants. The most persistent viral lineage in different cities in Peru was B.1.1, different from the ones reported in other countries.19,20 There is evidence that new variants, Alpha (B.1.1.7), Beta (B.1.351), Gamma (B.1.1.28), and Delta (B.1.671.2), which harbor the D614G mutation, can cause increased olfactory dysfunction. 21 However, there is no information regarding B.1.1 lineage and olfactory dysfunction. This could explain the high frequency of anosmia in the European and North American cohorts in contrast to our population.5,11,22
Results analysis
We did not find an association between COVID-19 severity and the presence of impaired olfaction. This is in contrast to studies that suggested that mild forms of COVID-19 are associated with a higher percentage of olfactory alteration and described a relationship between anosmia and a lower probability of being hospitalized.16,23,24 On the contrary, other studies indicated that there is no relationship between the severity of COVID-19 and the alteration of olfaction.5,25
The proposed mechanism of olfactory disturbance includes conductive deficits due to the loss of permeability caused by mucosal edema and mucus production, changes in mucus composition, and secondary changes in olfactory signals caused by the release of inflammatory intermediates such as cytokines. Additionally, it can cause postviral anosmia (months) because of direct damage to the olfactory sensory neurons responsible for the detection of odors in the olfactory epithelium 26 and can even cause retrograde propagation toward the upper neurons of the olfactory pathway. 27 However, recent evidence suggests that neural function is indirectly altered because of the sequelae of infection in peripheral support cells, including local inflammation and the gene expression of olfactory sensory neurons and ciliary structures. 26
Angiotensin-converting enzyme 2 (ACE2), which is found in high levels in the human olfactory epithelium of the upper airway, could contribute to the spectrum of symptoms involving the nasal passage, such as the olfactory alteration present in COVID-19. 28 Additionally, there might be an interaction between the spike proteins and ACE2 receptors of the target cells via the cell surface protease transaminase protease serine 2. 6 Finally, the severity of the symptoms may be related to the viral load, but a recent study refuted this idea. 29
We found differences between anosmia and age, thus corroborating the studies suggesting that a lower age is correlated with a higher prevalence of olfactory alteration. 13 In this regard, a mild course of the disease may be associated with a higher percentage of symptoms; this could explain the low prevalence of anosmia in older patients because these patients have a higher risk of developing a severe COVID-19 infection than that by younger patients. 30 It is worth noticing that there is a possible bias in our study because younger patients experienced less severe forms of COVID-19 infection, for that reason many of them could report this symptom more frequently rather than older patients who were dealing with more debilitating symptoms such as respiratory distress and cough. Furthermore, it is a fact that elderly patients experience a progressive loss of smell throughout their lives, and this could affect their subjective perception of their olfactory function during the acute COVID-19 infection. 13 However, there were no differences in sex, which is a finding similar to that of other studies. 13 Some reports have suggested that olfaction dysfunction is more prevalent in women than in men. 30 Other studies have suggested a higher percentage of anosmia as the initial symptom, 13 but it only occurred in 4.5% of patients in our sample. We also did not find an association between the alteration of smell and other symptoms of COVID-19.
The prevalence of the most frequent comorbidities, such as cardiovascular disease (21.9%) and diabetes (9.7%), was similar to that described in other studies. 31 These chronic diseases share similar characteristics with infectious diseases, such as a proinflammatory state and attenuation of the innate immune response. For example, in diabetes, inflammatory mediators that promote systemic insulin resistance are released, and metabolic disorders lead to a decrease in the immune function of lymphocytes and macrophages, which makes patients more susceptible to complications. 32
Regarding other symptoms in our study, we found that general malaise and cough were the most frequent; this finding differs from what was found in previous studies in the Asian population, where fever and general malaise were the most frequent. 32 However, compared with Latin American studies, general malaise, cough, and fever had similar frequencies. 2 These data allow us to elucidate that fever is not the most frequent symptom of COVID-19 in our country.
Relevance in clinical practice and public health
Peru has an inadequate healthcare system that is concentrated in isolated geographic areas and vulnerable groups. The health system has been operating at the limit for decades and was not prepared for a greater health burden (little budget allocated to health, low number of ICU beds [5 beds per 100,000 inhabitants], health coverage for only 60% of the population, and few health professionals). 33 Furthermore, there is a low capacity for molecular diagnosis, which was initially managed with the use of rapid antibody tests. 34 The coastal region and urban areas have a greater capacity of diagnostic testing than the Andean and Amazon regions or rural areas. 35 This has resulted in one of the highest mortality rates in the world, of 189.10 per 100,000 inhabitants, which has been surpassed by only Hungary, Italy, and Brazil. 36
Limitations and strengths
The study had the following limitations: 1) Our study performed a subjective evaluation of smell, which could have underdiagnosed the true dimension of olfactory alteration; however, the measurement was performed by considering the criteria described in international consensus 37 ; 2) The hospital in which the study was conducted is highly complex; therefore, patients admitted to the emergency service could have had more severe disease. However, upon enrollment, patients with a mild to moderate disease only could adequately respond to the survey; 3) The diagnostic criterion needed for COVID-19 to be considered in the study was a positive serological test, which does not have adequate diagnostic performance; however, it gave a reasonable clinical picture of COVID-19 at the time of evaluation. Furthermore, the Peruvian COVID national guideline used antibody testing as part of diagnostic criteria due to the lack of RT-PCR. 10 4) There was a high mortality rate in our study that limited olfactory follow-up. HNERM is a national referral center and thus receives more complex COVID cases. This is one of the few studies in the region that used a prospective design. Despite its limitations, this study represents the first prospective study in Latin America that aimed to evaluate olfactory alteration as a marker of COVID-19 severity. Future studies are needed to corroborate these findings in patients with mild disease.
Conclusions
This study found no significant differences between the severity of COVID-19 and olfactory dysfunction. Additionally, a low frequency of smell alteration was found in this study compared with studies from other regions. Smell alteration was also found to be associated with a younger age.
We recommend conducting studies with a larger number of patients to corroborate our results.
Footnotes
Acknowledgments
We thank the Instituto de Evaluación de Tecnologías en Salud e Investigación of EsSalud for their support to the development of this manuscript through their Mentoring Program.
Author contributions
OA, DS, AT, and MS designed the research. PM was responsible for the recruitment of COVID-19 patients and collecting data. OA, DS, and AT were responsible for organizing data. OA wrote the manuscript. All authors contributed to the article and approved the submitted version.
Declaration of conflicting interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by the Instituto de Evaluación de Tecnologías en Salud e Investigación of EsSalud through the Premio Kaelin en Ciencias de la Salud – Protocolo de Investigación 2020 (Versión especial de Investigaciones relacionadas a COVID-19) [Resolución 56-IETSI-ESSALUD-2020].