
Abstract

Keywords
Significance Statement
To date, the concurrence of extranodal natural killer (NK)/T-cell lymphoma (ENKTL) and chronic lymphocytic leukemia (CLL) has been reported in only 2 studies; however, in both, CLL was restricted to the bone marrow. Here, we report an extremely rare case of ENKTL/CLL coexistence in the nasal cavity. This expands the spectrum of ENKTL/CLL co-occurrence. Additionally, it highlights the importance of clinical history, histological observations, and immunohistochemistry in correctly diagnosing and effectively treating a patient.
In 2018, a 65-year-old man presented with multiple, bilateral enlarged lymph nodes in his neck, axilla, and groin and an elevated peripheral blood lymphocyte count (9.95 × 109/L). He was diagnosed with chronic lymphocytic leukemia (CLL) (The detailed data of pathology is available in Supplementary Figure S1). Treatment with a combination of thymosinα1, chlorambucil tablets, and interferon resulted in a favorable outcome. In September 2020, he presented with nasal obstruction and underwent a right nasal cavity biopsy. Peripheral blood showed white blood cell count of 5.74 × 109/L (lymphocytes, 3.15 × 109/L; neutrophils, 2.23 × 109/L), hemoglobin count of 118 g/L, and platelet count of 122 × 109/L. Computed tomography (CT) scanning revealed a soft-tissue mass in his dilated right inferior nasal meatus, reaching up to the right side of the right nasopharynx, and multiple bilateral enlarged lymph nodes in his neck (Figures 1a and 1b). The biopsy results revealed lymphocytic infiltration with lymphocytes of 2 different morphologies and focal coagulative necrosis (Figure 1c). One of the lymphocytes was medium to large with irregular nuclei (Figure 1d), and it stained positive for CD3 (Figure 1e), CD56 (Figure 1f), granzyme B, T-cell intracellular antigen 1 (TIA-1), and EpsteinBarr encoding region (EBER) in situ hybridization (Figure 1g), but negative for CD20, CD5, CD23, CD10, and cyclin D1. The other lymphocytic population included small mononuclear cells (Figure 1h) and its immunophenotype was positive for CD20 (Figure 1i), partially positive for CD23 (Figure 1j), and negative for CD3, CD56, CD5, CD10, cyclin D1, granzyme B, TIA-1, and EBER (Figure 1k). Polymerase chain reaction analysis revealed an identical monoclonal band for the immunoglobulin heavy chain gene (IgH) rearrangement, as compared to that observed in the first biopsy (Supplementary Figure S2); however, T-cell receptor gene (TR) gene rearrangement was not detected. Finally, the patient was diagnosed with composite extranodal natural killer (NK)/T-cell lymphoma (ENKTL) and CLL. (a and b) Computed tomography scanning of the nasal sinuses shows a soft-tissue mass in the dilated right inferior nasal meatus, reaching up to the right side of the right nasopharynx (a, soft-tissue window; b, bone window). (c) The biopsy results reveal the occurrence of 2 lymphocyte populations with different morphologies in the lymphocytic infiltrates, along with focal coagulative necrosis (hematoxylin and eosin (HE) stain, original magnification ×1.25). (dg) Medium to large lymphocytes (HE stain, original magnification ×400) with irregular nuclei and positively stained for CD3 (immunohistochemical (IHC) stain, original magnification ×400), CD56 (IHC stain, original magnification ×400) and EpsteinBarr encoding region (EBER; in situ hybridization (ISH), original magnification ×400). (hk) Small, mononuclear cells (HE stain, original magnification ×400) stained positive for CD20 (IHC stain, original magnification ×400), partially positive for CD23 (IHC stain, original magnification ×400), and negative for EBER (ISH, original magnification ×400).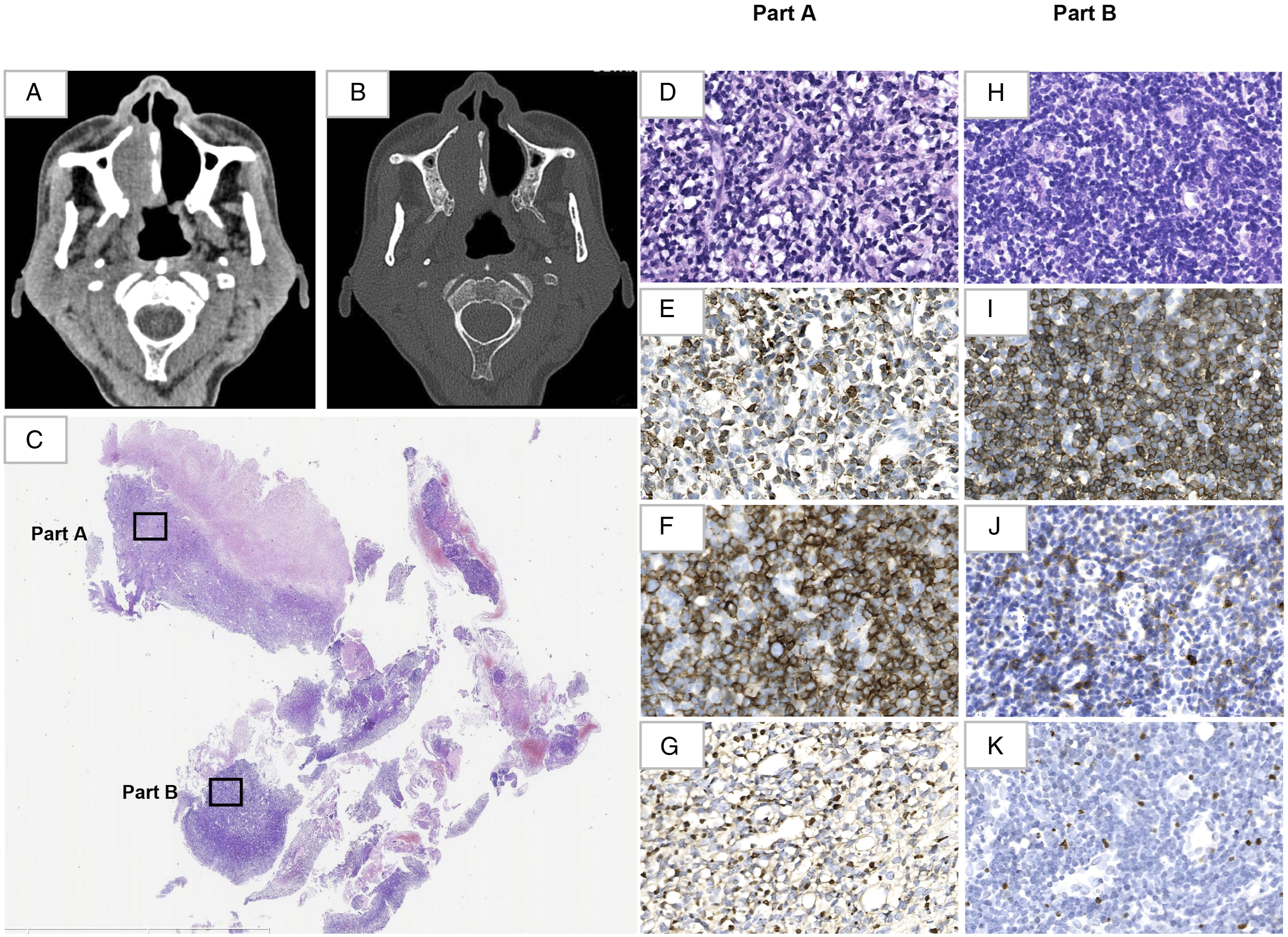
Incidentally, CLL mainly affects blood, bone marrow, and secondary lymphoid tissues. Even though extranodal involvement occasionally occurs in the skin, 1 gastrointestinal tract, 2 or central nervous system, 3 nasal cavity involvement is rare (<1%). Therefore, it can be easily misdiagnosed as chronic rhinosinusitis, resulting in ineffective treatments. 4 Interestingly, this case not only demonstrates the occurrence of CLL in such a rare site, but also reveals the co-occurrence of ENKTL in the same location. Usually, CLL patients have an increased risk of developing secondary cancers, such as other lymphohematopoietic neoplasms, cutaneous neoplasms, and solid cancers, like malignant melanoma and carcinoma. 5 The frequency of other lymphomas secondary to CLL ranges from 1 to 25%, with an annual incidence of approximately .5%. 6 A few studies have reported the concurrence of CLL and T-cell lymphomas, mainly peripheral T-cell lymphoma, not otherwise specified (PTCL-NOS), anaplastic lymphoma kinase (ALK)positive anaplastic large-cell lymphoma (ALCL), ALK-negative ALCL, and angioimmunoblastic T-cell lymphoma (AITL). 7 Interestingly, till date, there have been only 2 cases reporting the simultaneous presentation of CLL and ENKTL, and in both, CLL was restricted to the bone marrow, without any ENKTL tissue involvement. 6 Therefore, this is the first case to demonstrate the synchronous coexistence of CLL and ENKTL in the same location.
Although the CLL and ENKTL components of this patient were clonally unrelated, we speculated that his immunosuppressed condition may have caused the coexistence of these 2 types of lymphomas. It was reported that impaired physiological immune surveillance resulting from CLL and/or its therapy may lead to the activation of EBV, 8 which, in turn, might induce various EBV-related lymphomas of B-, T-, and NK-cell origin. Other studies have reported that the complex interaction between B- and T-cells in CLL may interfere with the normal functioning of the T-cells, and this has been confirmed by the increased expression of inhibitory receptors, such as programmed cell death protein 1 and CD244, on T-cells in peripheral blood of CLL patients. 7 These changes may contribute to T-cell function deficiency, 8 and hence, they are closely related to the occurrence of T/NK lymphomas.
In conclusion, this report describes an extremely rare case of co-existent ENKTL and CLL in the same location, and this expands the spectrum of ENKTL/CLL co-occurrence. It also highlights the importance of clinical history, histological observations, and appropriate immunohistochemical investigations in correctly diagnosing the patient. In future, more cases should be accumulated for a detailed study of the relationship between CLL and ENKTL.
Supplemental Material
Supplemental Material - The Effect of Tongue-Tie Release on Speech Articulation and Intelligibility
Supplemental Material for The Effect of Tongue-Tie Release on Speech Articulation and Intelligibility by Jonathan Melong, Michael Bezuhly and Paul Hong in Ear, Nose & Throat Journal
Supplemental Material
Supplemental Material - The Effect of Tongue-Tie Release on Speech Articulation and Intelligibility
Supplemental Material for The Effect of Tongue-Tie Release on Speech Articulation and Intelligibility by Jonathan Melong, Michael Bezuhly and Paul Hong in Ear, Nose & Throat Journal
Supplemental Material
Supplemental Material - The Effect of Tongue-Tie Release on Speech Articulation and Intelligibility
Supplemental Material for The Effect of Tongue-Tie Release on Speech Articulation and Intelligibility by Jonathan Melong, Michael Bezuhly and Paul Hong in Ear, Nose & Throat Journal
Footnotes
Author Contributions
YY and QZ contributed to the figures. WD contributed to clinical data. YY completed the manuscript. SZ made pathological diagnosis of this case and revised the manuscript. All authors read and approved the final manuscript.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by Sichuan Science and Technology Program (2018JY0612), 1·3·5 project for disciplines of excellence–Clinical Research Incubation Project, West China Hospital, Sichuan University (grant number 2021HXFH027).
Ethical approval
The study was approved by the Ethics Committee on Biomedical Research, West China Hospital of Sichuan University. The committee waived the requirement for informed consent as the data for the patient included in the study were retrospectively analyzed.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.