
Abstract

Significance Statement
Primary diffuse large B-cell lymphoma of the tongue base is rare, and cases with acute airway obstruction are rarely documented. Patients with lymphoma of tongue base may present with rapid respiratory deterioration due to tumor edema. Herein, we reported a case of diffuse large B-cell lymphoma of the tongue base that presented with dyspnea and required emergent intubation.
A 68-year-old man had a 3-year history of neck swelling. He presented with progressive dyspnea and tongue swelling for 1 month. On physical examination, a 5-cm firm, fixed mass in the right level II/III was noted. Laryngoscopy revealed a prominent mass arising from the base of the tongue with compression of the laryngeal inlet (Figure 1). Computed tomography of the neck revealed extensive invasion of the mass into the tongue base and left parapharyngeal space (Figure 2A). Intravenous injection of dexamethasone followed by nasotracheal intubation was performed for impending airway obstruction. Laryngoscopy view of the tongue base tumor. (A) CT demonstrated a slightly hyperdense mass lesion measuring approximately 6.4 x 6.5 x 6.1 cm in diameter (arrow) located in the tongue base region. (B) T1-weighted MRI demonstrated a huge hypoattenuating mass (arrow) at the tongue base causing posterior displacement of the epiglottis. (C) Positron emission tomography showed the large tongue base tumor and multiple hypermetabolic lesions in other anatomical sites.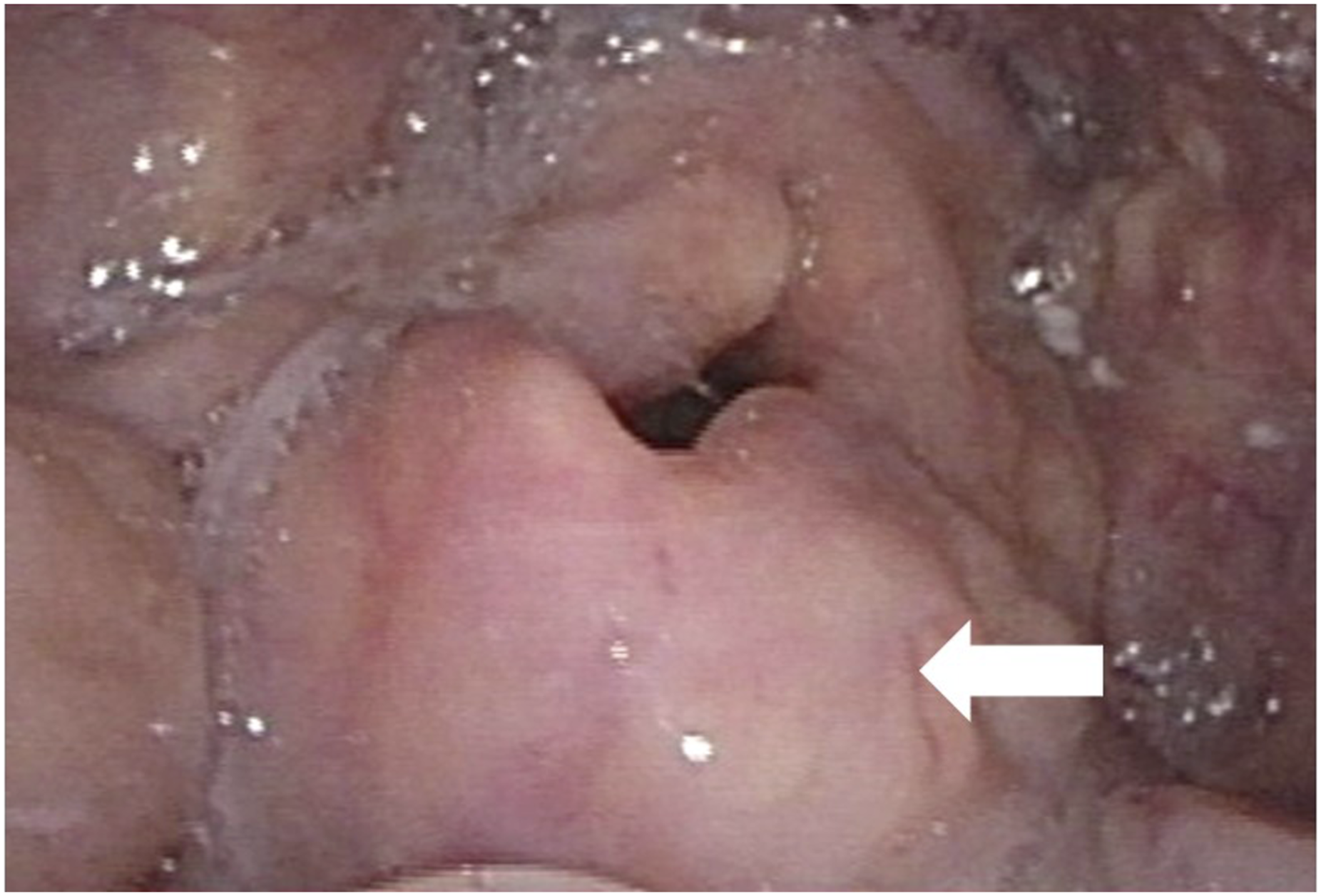
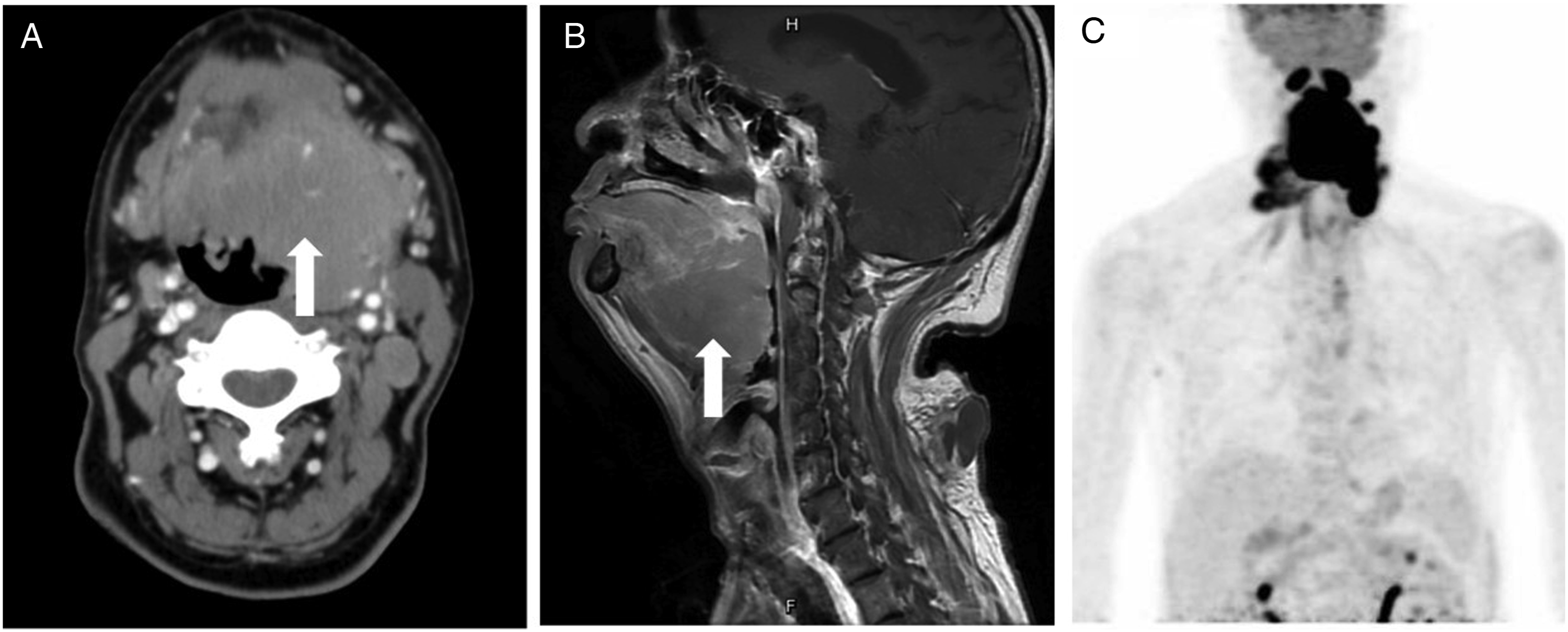
Subsequently, he received a tracheostomy and biopsy of the tongue base mass. Histopathology showed atypical B lymphoid cells in a diffuse growth pattern with large nuclei and discohesive cells infiltrating the tongue tissue that were positive for Bcl6, CD10, CD20, and MUM1 (Figure 3). Magnetic resonance imaging showed the mass involving the base of the tongue, oropharynx, and pre-epiglottic space, which appeared hypointense on T1-weighted images (Figure 2B). Positron emission tomography showed a mass involving the tongue, oral cavity, nasopharyngeal regions, neck, mediastinum, and lung (Figure 2C). The final diagnosis was a stage IV diffuse large B-cell germinal-centertype lymphoma (DLBCL) of the tongue base. The patient was subsequently referred to receive chemotherapy. Histopathological results of the tongue base tumor. (A) Diffuse sheets of atypical B lymphoid cells with large nuclei and discohesive cells infiltrating the tongue tissue (x40 magnification). (B) Immunostaining for Bcl6 (x100 magnification). (C) Immunostaining for CD 10 (x100 magnification). (D) Immunostaining for CD 20 (x100 magnification).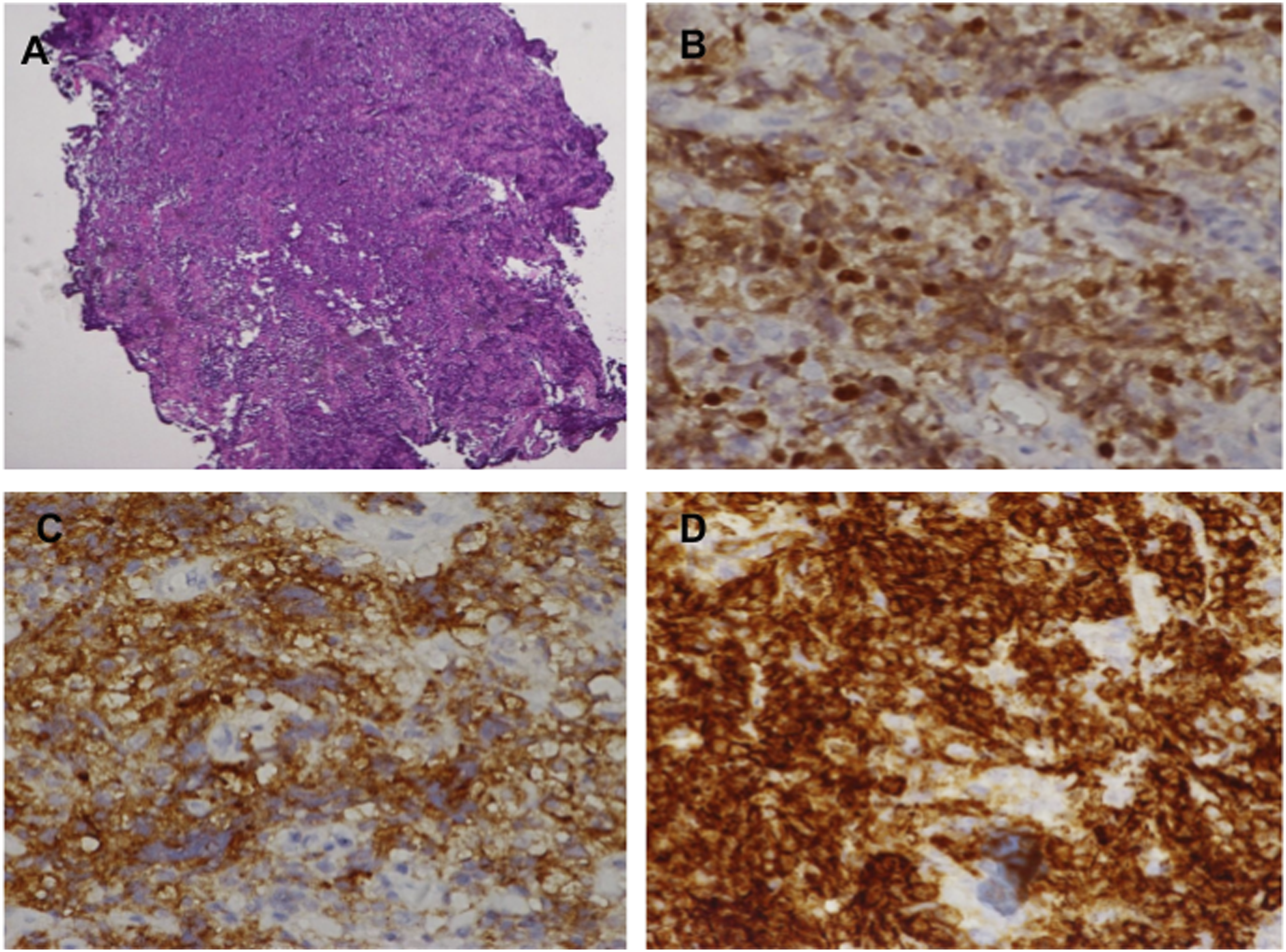
Diffuse large B-cell lymphoma is the most common type of non-Hodgkin lymphoma and often presents with rapid symptom development. Primary diffuse large B-cell lymphoma of the tongue base (BOT) is a rare entity and may present with regional symptoms such as dysphagia, foreign body sensation, or progressive dyspnea.1-3 The elderly are most affected, especially after the sixth decade of life. The etiology may be associated with infections, immunodeficiency states, and chronic inflammation.3,4 Diagnosis of BOTs is most often made by biopsy and immunohistochemical analysis, whereas imaging cannot reliably differentiate BOTs from other head and neck neoplasms. 3 The germinal-center subtype of DLBCL can be distinguished by 3 markers including CD10, Bcl6, and MUM1. 5 Very large BOTs may cause rapid respiratory deterioration due to tumor edema and/or mucositis. 2 Osto, M., et al reported BOT with acute respiratory failure and patients were treated with intravenous steroid administration and awake tracheostomy followed by R-CHOP chemotherapy. Our case also demonstrated the importance of early intubation and steroid administration followed by chemotherapy to treat airway distress. In a previous study, use of steroids provided benefits for reducing laryngeal edema. 6 Although BOT is very uncommon, it should always be considered in differential diagnosis from other head and neck neoplasms in this region. Considering its aggressive natural history, a definitive airway should be established and corticosteroids administration should be provided for patients with BOTs initially presenting with obstructive symptoms.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.