
Abstract
Inflammatory myofibroblastic tumor (IMT) is a tumor composed of differentiated myofibroblastic spindle-shaped cells. It occurs in the soft tissues of the abdomen and lungs, and is very rare in the sphenoid sinus. The diagnosis depends on histopathology and immunohistochemistry, and is easily misdiagnosed. Although metastasis is rare, the recurrence rate is high. Surgical resection is the treatment of choice, and where complete resection is difficult, radiation therapy, hormonal therapy, or molecular targeted drug therapy can be administered. We report a rare case of IMT with a primary origin in the sphenoid sinus, which was entirely resected by nasal endoscopy and confirmed by histological examination.
Introduction
Inflammatory myofibroblastic tumor (IMT) is a tumor composed of differentiated myofibroblastic spindle cells, often accompanied by a large number of plasma cells and/or lymphocytes. 1 The etiology of the disease is unknown; it commonly occurs in the soft tissues of the abdomen and lungs and rarely in the head and neck; if it occurs in the head and neck, it is most often seen in the maxillary sinus, and its primary origin in the maxillary sinus is sporadic in the sphenoid sinus. The clinical manifestations of the disease are varied and lack typical symptoms and signs; specific imaging findings are lacking; and early diagnosis still relies on histopathological and immunohistochemical examinations. Although metastasis is rare, the recurrence rate is high, with some literature reporting local recurrence rates as high as 1525% after surgery.2,3 In this report, we present a case of an adult female patient with IMT originating from the sphenoid sinus.
Case Report
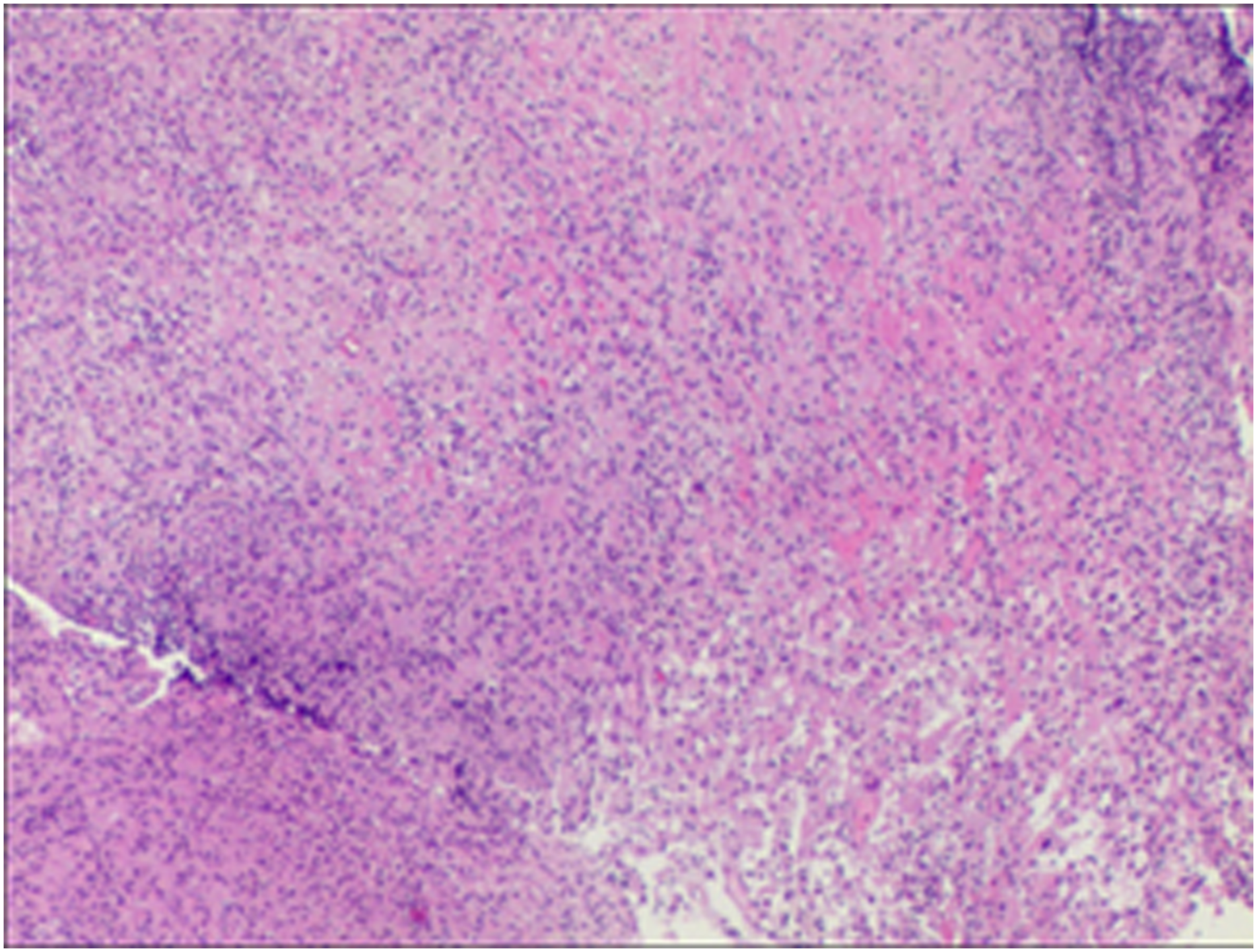
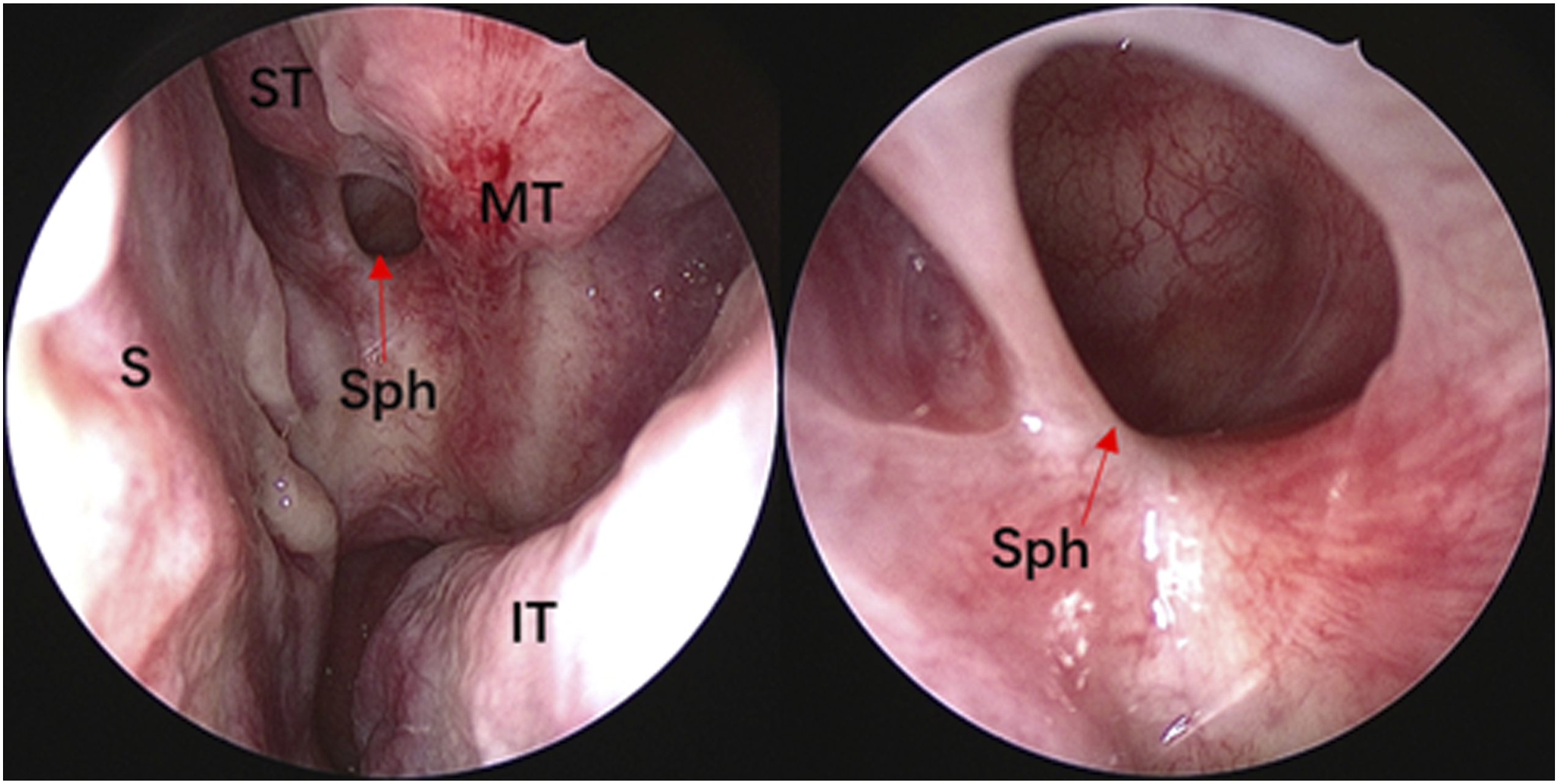
A 38-year-old female patient presented with “a headache for more than half a month.” The headache was evident in the occipital region with no discomfort in other areas. Computed tomography (CT) examination of the sinuses revealed a round cystic lesion in the left sphenoid sinus, measuring approximately 10 × 8 mm, with no abnormal soft tissue density shadow filling the rest of the sinus cavity (Figure 1). The rest of the routine preoperative examination and local examination showed no significant abnormalities. Under general anesthesia, the left sphenoid sinus was opened under nasal endoscopy, and the sphenoid sinus tumor was removed. During the procedure, the anterior part of the left sphenoid sinus bulged forward with a thick-walled cyst-like object with a tough, partially ossified, yellow color. The resected specimen was sent for pathological examination. The cell anisotropy was slight; the nuclear division was rare; and there were primarily lymphocytes, plasma cells, and histiocytes infiltrating, and occasional ossification was seen. Immunohistochemistry was performed: Vimt (+), SMA (+), CD34 (+), CD68 (+), Ki-67 (∼5%+), CK (−), S-100 (−), and Desmin (−). Inflammatory myofibroblastic tumor was diagnosed. (Figure 2).The patient reported the disappearance of headache and stable condition on the first postoperative day. At 6 months postoperatively, our patient was in good condition and disease free with regular clinical endoscopic (Figure 3) and radiological follow-up. Preoperative CT examination of the sinuses: (A) Sagittal bone window with occupancy of the left sphenoid sinus; (B) horizontal bone window with a round cystic lesion in the left sinus; and (C) coronal soft tissue window with occupancy of the left sphenoid sinus with heterogeneous density and dotted high-density shadow. The red arrow shows the location of the tumor. The yellow arrow shows the high-density shadow. Postoperative pathological results (HE staining, 100 × magnification). Nasal endoscopic findings 6 months after surgery: smooth, light red mucosa in the left sphenoid sinus with no signs of tumor recurrence. S: nasal septum; ST: superior turbinate; MT: middle turbinate; IT: inferior turbinate; Sph: enlarged sphenoid sinus opening through the anterior part.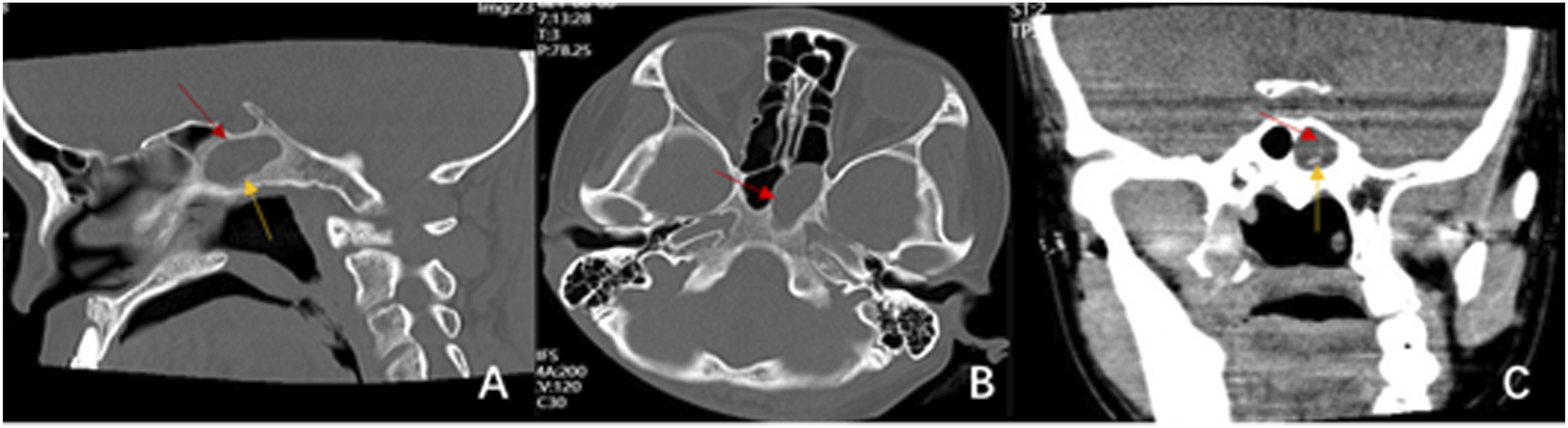
Discussion
Inflammatory myofibroblastic tumor is a unique mesenchymal tumor of variable benignity, and most of the current literature supports that the tumor is a predominantly locally recurrent junctional tumor. 4 The incidence population is nonspecific, with a slight female predominance. In this case, an adult female presented with a headache and a sphenoid sinus lesion was found during a head examination, with no usual nasal discomfort. The main clinical manifestations were mainly local obstructive symptoms such as nasal congestion, facial pain, and swelling due to the growth of the tumor itself, with a few patients presenting with early symptoms of a toothache. Generally, patients do not have systemic symptoms in the early stage of the disease. Inflammatory myofibroblastic tumor occurring in the sinuses is not specific in clinical manifestations and can be easily misdiagnosed.
CT scans of IMT mostly show soft tissue masses with or without bone destruction in the nasal cavity and sinuses. Inflammatory myofibroblastic tumor originates from the maxillary sinus often has bone destruction and mild development on enhancement scans, suggesting a tendency for infiltrative growth, making it difficult to distinguish it from other sinus tumors on imaging. 5 The preoperative CT examination of the sinus in this patient only showed a round cystic lesion in the left sphenoid sinus, with an intact bone in each sinus wall and no signs of hyperplasia, sclerosis, or destruction; and the patient had no special clinical manifestations, so it was misdiagnosed as a benign sphenoid sinus cyst before surgery and enhanced CT and magnetic resonance examination were not performed. During surgery, the shape and texture of the left sphenoid sinus cyst were found to be peculiar. It was different from the usual mucinous cysts. Therefore, the mucosa of the sphenoid sinus at the base of the mass was peeled off and excised based on complete excision of the sphenoid sinus mass. The preoperative review showed a small amount of high-density shadow in the left sphenoid sinus, which was considered a cyst formation in the left sphenoid sinus, and the possibility of fungal infection could not be excluded. This is consistent with the postoperative pathological finding of “episodic ossification.” It can be seen that IMT should be differentiated from a fungal sinus infection in addition to sinus malignancy in order to avoid misdiagnosis and mistreatment leading to overtreatment or local recurrence due to inadequate resection during surgery.
Pathologic examination remains the primary means of differentiating IMT. Because the tumor cells that constitute IMT have morphological characteristics of smooth muscle and fibroblasts, they must be pathologically distinguished from tumors of both cellular origins. Pathological examination of IMT is histomorphological, composed of proliferating fibroblasts and myofibroblasts in a dendritic or woven arrangement, in which collagenization and mucinous edema can be seen. In immunohistochemistry, most cases were positive for Vimentin, Desmin, and SMA and negative for S-100. 6 The pathological examination showed a large number of spindle-shaped hyperplasia in an inflammatory background, requiring consideration of the morphological differentiation between inflammatory hyperplasia and inflammatory myofibroma. Combined with immunohistochemistry Vimt (+), SMA (+), and S-100 (−), which showed a predominance of myofibroblasts, the diagnosis was IMT.
The treatment of IMT includes surgical resection, hormone therapy, radiotherapy, and chemotherapy. 7 Most scholars believe that surgical resection is the treatment of choice, and radiotherapy or hormonal therapy can be administered in cases where complete resection is complex. The molecularly targeted drug crizotinib, which has emerged in recent years, has also shown good efficacy. 8 The literature has reported a significantly higher proliferation index of Ki-67 in cases considered to be malignant. 9 In the present case, Ki-67 (approximately 5%+), combined with the mild heterogeneity of tissue cells and rare nuclear divisions in the sent specimen, was considered a low-grade malignant junctional tumor, so the patient was given no other adjuvant treatment based on complete surgical resection of the tumor and was closely followed for 6 months with no signs of recurrence. Due to the lack of characteristic clinical manifestations and imaging features, the ENT surgeons were not sufficiently aware of this disease and were prone to misdiagnosis. If the first surgical lesion was not completely excised, this might be an essential factor contributing to the high rate of local recurrence of the tumor. Therefore, a long-term follow-up of the case is also needed to prevent a recurrence.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.