
Abstract
Objectives
Sphenomaxillary plate (SMP) is an inconstant bony septum separating the maxillary and sphenoid sinuses. Neglecting the SMP during endoscopic sinus surgery may lead to mistaking the sphenoid sinus for the posterior ethmoid cell with potentially dangerous consequences. However, its proper identification may allow planned sphenoidotomy through the posterior wall of the maxillary sinus or to enlarge transnasal or transethmoidal sphenoidotomy. The aim of this study was to evaluate (1) the incidence and morphology of the SMP and (2) possibility and safety of trans-SMP sphenoidotomy.
Methods
In the radioanatomical part of the study multiplanar reconstruction analysis of 117 consecutive paranasal sinus CT scans was conducted. In the clinical part of the research, trans-SMP sphenoidotomy was performed in consecutive patients operated on for chronic rhinosinusitis.
Results
The SMP was found in 25% of sides (34% of patients). It was constantly located superolateral to the posterior insertion of the middle turbinate. The SMP formed the prominence on the posterior wall of the maxillary sinus that could be identified using volume rendering in 11% of sides (19% of patients). 30 trans-SMP sphenoidotomies were performed in 18 patients. The SMP prominence was identified in 15 sides. In absence of SMP prominence, identification of the SMP was still possible using other anatomical landmarks.
Conclusions
The SMP is present in over 30% Caucasian subjects at least on one side. Sphenoidotomy through the SMP is feasible and safe.
Introduction
The most established and commonly performed endoscopic approaches to the sphenoid sinus are transethmoidal, transnasal, and transseptal. Their main principle is to stay close to the midline to prevent injury to the internal carotid artery and the optic nerve. Sphenomaxillary plate (SMP) is a bony septum separating the maxillary and sphenoid sinuses, first described by Onodi. 1 The SMP is cursorily mentioned in textbooks and studies evaluating anatomical variations of the paranasal sinuses.2 –5 However, there is limited data in the literature on its morphology and exact prevalence. 6 Neglecting the SMP during preoperative planning may lead to the inadvertent opening of the sphenoid sinus and mistaking it for the posterior ethmoid cell.3,5,7 This in turn may result in injuring the neighboring vital structures. On the other hand, when properly identified, the SMP can be potentially used for planned sphenoidotomy or to widen the opening of the sphenoid sinus laterally. Maximum enlargement of the sphenoidotomy is important in patients with inflammatory sinus disease to provide adequate aeration, drug delivery, and saline penetration. Current CT imaging software provides 3D and multiplanar reconstructions (MPR), allowing preoperative identification of the SMP.
The aim of this study was to evaluate (1) the incidence and morphology of the SMP and (2) possibility and safety of trans-SMP sphenoidotomy.
Patients and Methods
We analyzed 117 consecutive thin-slice (<0.7 mm) paranasal sinus CT scans using multiplanar reconstruction (MPR). Patients with paranasal sinus or skull base tumors, after previous sinus surgery, of <18 years of age, with a modified Lund–Mackay score of 4 or more were excluded. Two reviewers evaluated the scans independently for the presence of the SMP using Horos software (Horos project, open source medical image viewer). The images were oriented in sagittal, axial, and coronal planes using the nasal floor and the lateral aspects of the orbits as reference points. The cutting planes were further aligned for maximum exposure of the evaluated structures. The SMP was defined as a bony plate with a size of >4 × 4 mm. A virtual image of the posterior wall of the maxillary sinus was created using a 3D rendering tool and assessed for the presence of prominence produced by the SMP.
The maxillary recess of the sphenoid sinus (MRSS) was defined as anterolateral pneumatization of the sphenoid sinus anterior to the coronal plane perpendicular to the nasal floor through the anterior wall of the pterygopalatine fossa (PPF) at the level of the sphenopalatine foramen (Figure 1A). This plane is further referred to as anterior PPF plane (Figure 1). Parasagittal CT reconstruction. A, MRSS - shaded in green, B, SRMS - shaded in red, O, orbit, M, maxillary sinus, S, sphenoid sinus, white asterisk - optic nerve, red asterisk - internal carotid artery. Yellow line - anterior PPF plane. MRSS, the maxillary recess of the sphenoid sinus, SRMS, the sphenoid recess of the maxillary sinus, PPF, pterygopalatine fossa.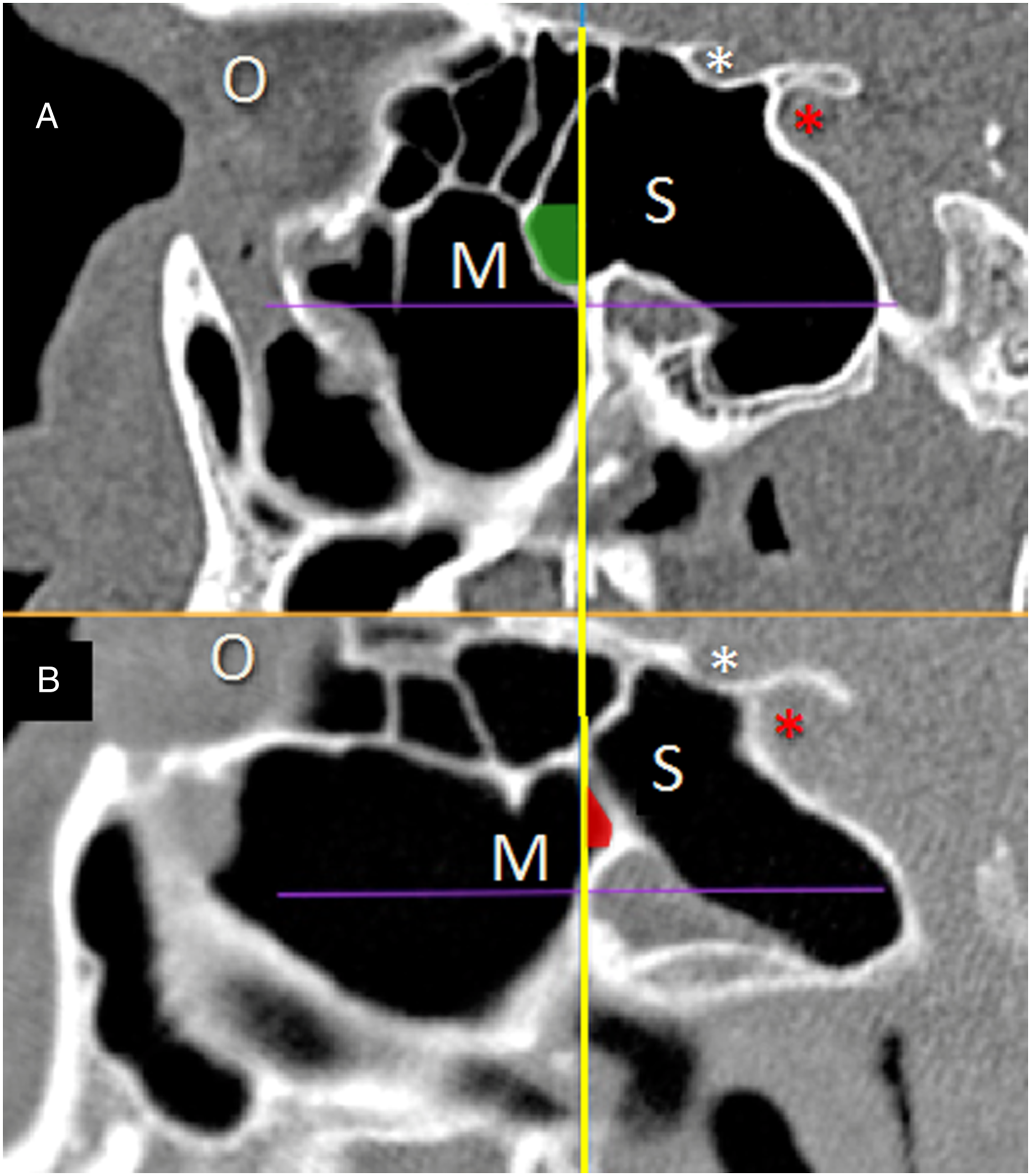
The sphenoid recess of the maxillary sinus (SRMS) was defined as superomedial pneumatization of the maxillary sinus extending toward the sphenoid sinus posterior to PPF plane (Figure 1B).
Interrater agreement was measured with the Kappa statistic using SPSS (version 25). Disagreements were discussed until agreement was reached. The shortest distance between the protuberance of the internal carotid artery (ICA) and the sphenoid ostium, and the distance between the ICA protuberance and medial aspect of the SMP were measured. The results were compared with the Wilcoxon signed rank test with continuity correction.
In the clinical part of the study, consecutive patients undergoing endoscopic sinus surgery requiring sphenoidotomy were evaluated for the presence of the SMP on preoperative CT scans. We attempted to perform trans-SMP sphenoidotomy. Procedures were performed under general anesthesia using a 30° endoscope. The surgery started from uncinectomy, wide middle meatal antrostomy. Further course of the procedure depended on the possibility to identify the SMP.
The university ethics committee approved the study.
Results
Radioanatomical analysis showed the presence of the bony septation between the maxillary and sphenoid sinuses of <4 × 4 mm in size in 52 of 234 sides (22%), in 39 of 117 subjects (33%). The SMP defined as a bony plate of >4 × 4 mm in size was found in 60 sides (25.6%), in 40 subjects (34%). Bilateral SMP was found in 20 subjects (17%). The interrater agreement for the identification of the SMP was fair to good, 0.69 (<0.05).
Analysis of CT scans showed the most constant features of the SMP among the study patients.
On the saggital view, the SMP was inserted to the superior boundary of the pterygopalatine fossa. The SMP ascended anteriorly overhanging the lower posterior wall of the maxillary sinus to join bony partitions of the ethmoid cells (Figure 1A). On the axial oblique view, the lateral attachment to the lower posterior aspect of the medial orbital wall was found at the level of the inferior orbital fissure. The SMP transversed the upper-posterior angle of the maxillary sinus in the anteromedial direction to join the posterior aspect of the lateral wall of the nasal cavity (Figure 2A and C). When looking at the posterior wall of the maxillary sinus from anterior and below in 3D images, the superomedial part of the circumference of the SMP was closer to the observer than its inferolateral part (Figure 2B and D). Convex (A, B) and concave (C, D) SMP: A and C, axial CT reconstruction. Distances between: ICA and sphenoid ostium, ICA and SMP marked in green. B and D, 3D reconstruction of the posterior wall of the maxillary sinus: B, The SMP protuberance on both sides, D, SMP concave on both sides. SMP - sphenomaxillary plate, ICA - internal carotid artery.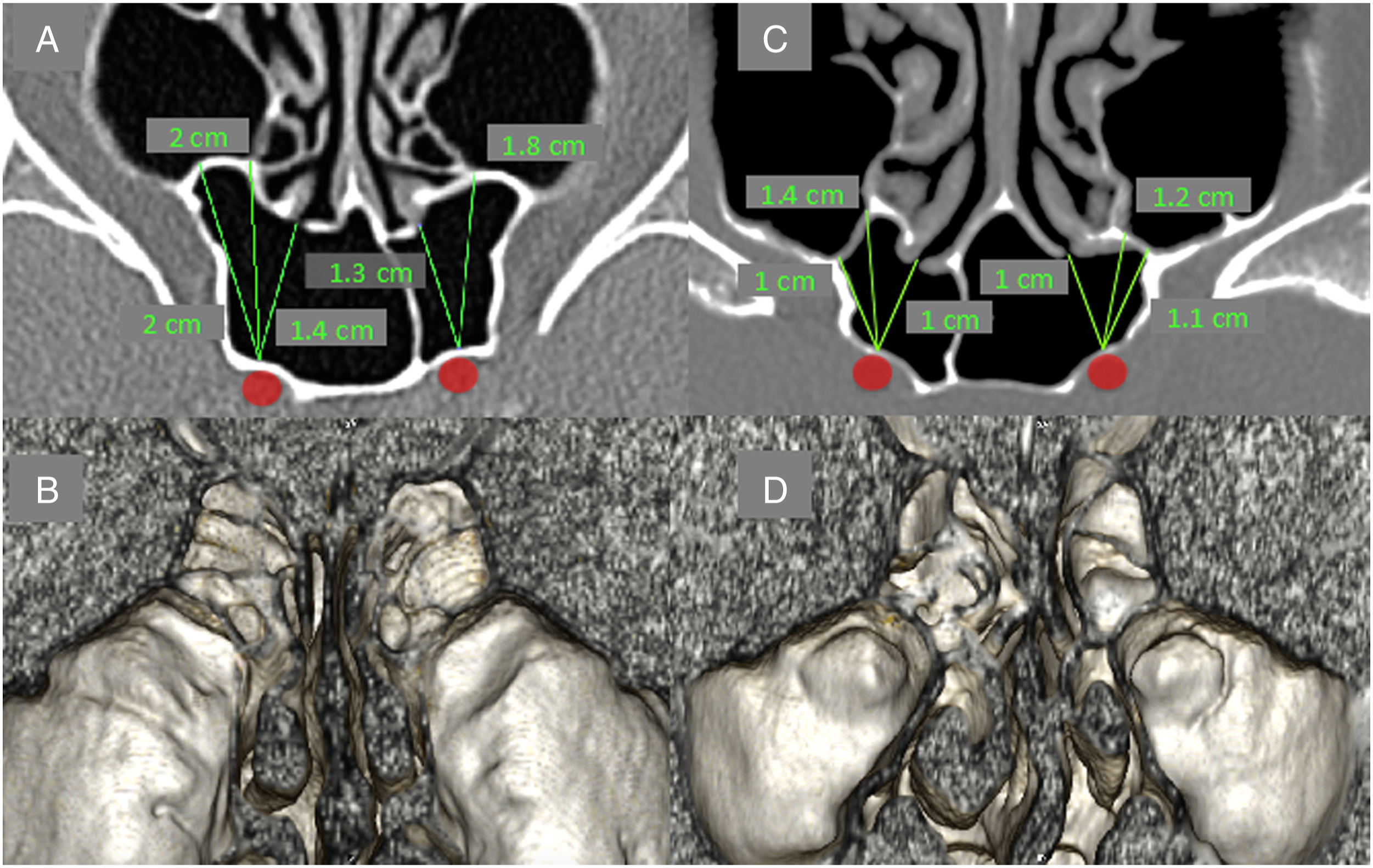
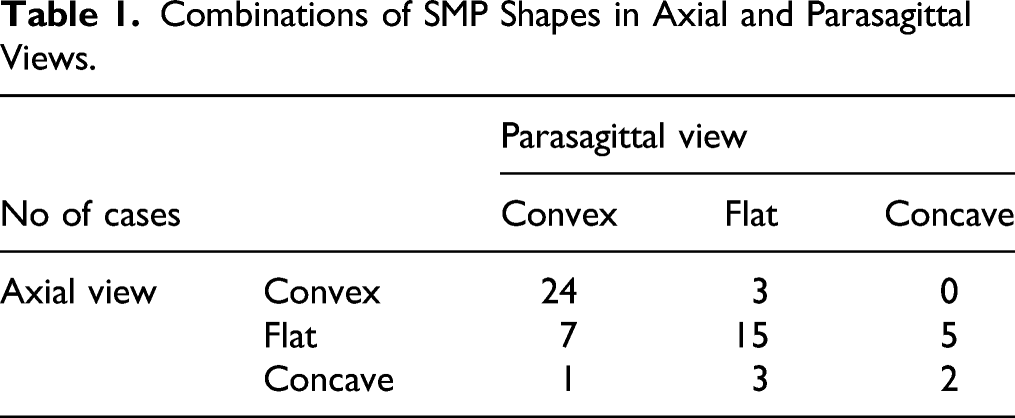
On the axial view, the medial insertion of the SMP was located more anterior to the lateral insertion in 91% of cases (55/60), and in the remaining cases, both insertions were placed in one coronal plane, or the lateral attachment was located anteriorly to the medial one in the upper part of the SMP (2 cases).
The mean antero-posterior span of the SMP (the distance between the first and last coronal scan with visible SMP) was 3.8 mm (range 2–7). The mean vertical span (the distance between the first and last axial scan with visible SMP) was 5.3 mm (range 2.4–10).
Combinations of SMP Shapes in Axial and Parasagittal Views.
The MRSS was present in all but one SMP. The mean anterior extension of the MRSS from the anterior PPF plane was 3.7 mm (range 1–7 mm).
The SRMS was present in 5 sides (1.9%). Its mean posterior extension from the anterior PPF plane was 1.4 mm (range 1 to 2 mm). In 4 of these sides, both MRSS and SRMS were present. In all these cases, the MRSS was medial to the SRMS. Among 5 cases with the SRMS, there were 2 SMPs concave in the sagittal plane and flat in the axial plane, the remaining 3 SMPs did not show any concavity.
The prominence of the posterior wall of the maxillary sinus (SMP prominence) was identified on the 3D images in 35 sides (58% of the SMPs). All these SMPs were convex on axial scan (Figure 2A and B).
The most anteromedial part of the SMP was located just below the ethmoid cell neighboring the lamina papyracea in 48 of 60 SMPs (80%). In the remaining cases, the superior continuation of the SMP (anteromedial wall of the MRSS) transformed into the posterior wall of this cell or the medial aspect of the SMP was attached to the middle orbital wall.
Various air spaces located medial to the superior part of the SMP pneumatizing between the maxillary and sphenoid sinuses were found in 17 sides (28% of the SMPs). These air spaces included the ethmoidal cells draining under the superior or supreme nasal turbinate or invagination of the superior nasal meatus. Four of these air spaces were pneumatizing behind the deepest part of the posterior wall of the maxillary sinus.
The mean shortest distance between the ostium of the sphenoid sinus and the ICA protuberance was 13.4 mm. The mean shortest distance between the ICA protuberance and the medial insertion of the SMP was 18.3 mm. The difference between these 2 distances was statistically significant (P < 0.05). In all the cases, the ICA-ostium distance was shorter than the distance between the ICA and medial insertion of the SMP.
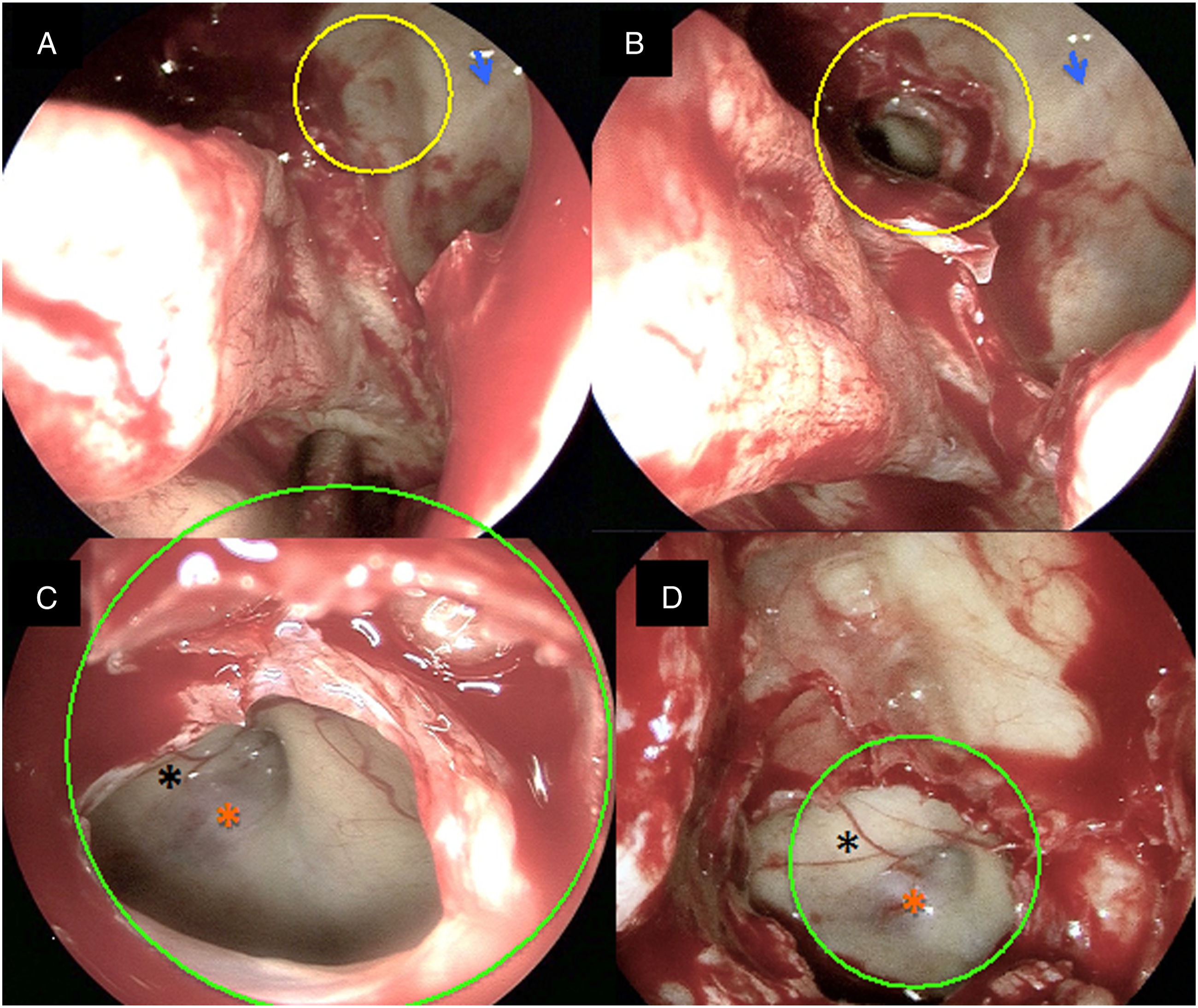
In the clinical part of the study, the trans-SMP approach to the sphenoid sinus was performed in 30 sides (18 patients). In one patient, it was used to open the hypoplastic sphenoid sinus with well-pneumatized MRSS. There were 15 SMPs with the SMP prominence in this group. The preoperative 3D images of the SMP prominence in non-opacified maxillary sinuses were similar or identical to the intraoperative endoscopic view in all cases (Figures 3 and 4). Due to opacification of the maxillary sinus, in 2 cases, the quality of the 3D images was unsatisfactory but allowed for identification of the SMP prominence. In all of these patients, trans-SMP sphenoidotomy was performed without the need of prior posterior ethmoidectomy. In patients without the SMP prominence, the most useful anatomical landmarks were insertion of the basal lamella of the middle turbinate located below the SMP, orbital floor located above the SMP, and the prominence of the infraorbital canal pointing to the pterygopalatine fossa. There were no intraoperative complications. Preoperative planning: A–C, 3D images: red arrow - sphenopalatine foramen, blue arrow - infraorbital nerve. A, SMP protuberance (yellow circle), B and C, virtual dissection of the SMP exposing the optico-carotid recess (red circle). D, parasagittal and E, axial CT reconstruction. White asterisk - optic nerve, red asterisk - internal carotid artery. SMP - sphenomaxillary plate. Intraoperative photographs of left-sided trans-SMP sphenoidotomy (the same patient as in Figure 3). A, wide middle antrostomy: SMP in yellow circle, blue arrow - infraorbital nerve. B, Perforated SMP, C and D, optico-carotid recess - green circle. SMP - sphenomaxillary plate.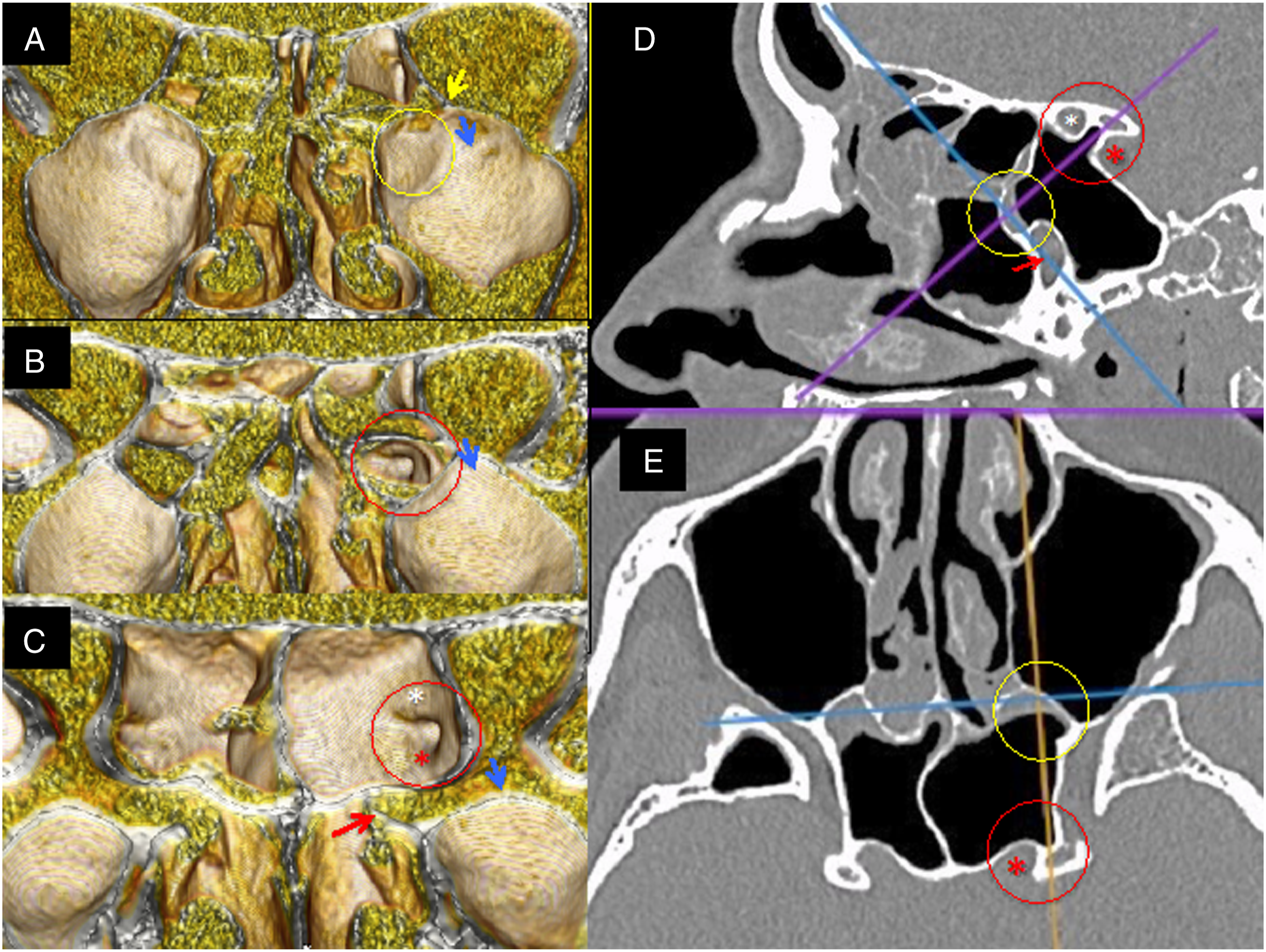
Discussion
Van Alyea 8 found contact between the sphenoid and maxillary sinuses in 15 out of 100 half-heads. Bulging of the sphenoid sinus in the posteromedial wall of the maxillary sinus was observed in only two of these cases. He also commented on transantral approach to the sphenoid sinus described by Mosher in 1903: “Such an operation naturally has a limited scope and is applicable only in those few cases in which walls of the two cavities come together.”
The prevalence of the SMP in different studies on anatomical variations of the paranasal sinuses ranges between <14% and 17% of patients.3–5 These turn-of-the-20th-century studies most probably underestimated the prevalence of the SMP due to technical limitations; CT scans were assessed in standard axial and coronal planes without the MPR, while the SMP is best exposed in axial oblique and parasagittal views. In a recent study on the anatomy of the posterior angle of the maxillary sinus, Craiu et al., 6 who used the MPR, reported the presence of the SMP in 28% of the sides. The MRSS was found in 24% of the sides and SRMS in 4% of the sides, which is similar to our results. Bulging of the posterior wall of the maxillary sinus was present in only 2 cases (7% of the SMPs). Similarly to Van Alyea, the authors most probably regarded a small prominence on the posterior wall of the maxillary sinus as irrelevant and did not report it. We found it useful in localizing the SMP. The SMP prominence was present in 58% of the SMPs on 3D images obtained using a volume rendering tool.
Most manuals of endoscopic sinus surgery recommend to enter the sphenoid sinus through the lower medial quadrant of the anticipated anterior wall of the sinus during a transethmoidal approach. Some authors advise to combine transethmoidal and transnasal approaches using the superior nasal turbinate as a landmark for identification of the sphenoid ostium. These techniques are effective and safe. If present, the SMP can be used for an additional or alternative approach. Breaching the prominence of the SMP enables early identification of the sphenoid sinus, which may accelerate the procedure. Although the SMP is located at a safe distance from the ICA protuberance, it may pose a higher risk of inadvertent penetration of the sphenoid sinus with the surgical tool compared to widening of the natural ostium. Using cutting tools and avoiding pushing movements can prevent this complication. The shape of the SMP dictates the most convenient direction of dissection.
We performed 30 trans-SMP sphenoidotomies without any complications. The SMP prominence was easy for preoperative and intraoperative identification. In absence of the SMP prominence, trans-SMP sphenoidotomy is still possible but can be more challenging. Anatomical landmarks useful in locating the SMP in these cases are insertion of the basal lamella of the middle turbinate to the lateral wall of the nasal cavity, infraorbital nerve, and middle orbital floor. Staying above the insertion of the middle turbinate prevents injuring the sphenopalatine artery and pterygopalatine fossa, which should not be challenging for surgeons familiar with the sphenopalatine ligation/coagulation technique. Another landmark helping to stay above the sphenopalatine artery is the medial part of the infraorbital nerve pointing at the pterygopalatine fossa (Figures 3 and 4). Further widening of the antrostomy above the insertion of the middle turbinate and below the middle orbital floor in the posterolateral direction should finally breach the SMP. If there is still no certainty regarding the location of the SMP, opening the posterior ethmoid cell neighboring to the orbit that extends above the MRSS may help to identify lamina papyracea and expose the superomedial wall of the MRSS.
Prominent MRSS extending anteromedially can be inadvertently entered during FESS. In these cases, inaccurate preoperative planning may lead to surgical disorientation and mistaking the sphenoid sinus for the posterior ethmoidal cell.3–5 Experienced endoscopic surgeons are familiar with the endoscopic view of the optico-carotid recess and sella turcica, which are key landmarks within the sphenoid sinus. However, these landmarks may be absent or hidden behind the bony septum, due to hypoplasia of the sphenoid sinus or the presence of the sphenoethmoidal (Onodi) cell.
Among the 117 analyzed CTs, bony partitions separating the maxillary and sphenoid sinuses smaller than 4 × 4 mm were present in 52 sides (22%). Most of them are thicker compared to those greater than >4 × 4 mm. Due to their dimensions, they would be rather difficult to find intraoperatively without prior transnasal or transethmoidal sphenoidotomy.
Pneumatization patterns of the air spaces located between the maxillary and sphenoid sinuses were described by Craiu. 6 In the current study, we analyzed only those associated with the superior part of the SMP. Among these air spaces, there were 9 ethmoid cells that drained into the superior meatus and 2 cells draining into the supreme meatus. The ethmoid cells draining into the supreme nasal meatus were first described by Van Alyea, who named them as postreme cells. 9 A recent radioanatomical study using CT volume rendering and MPR confirmed their presence in 45% of the sides in adult Caucasians. 10
In our opinion, the air spaces medial to the superior part of the SMP facilitate its identification, especially when they produce characteristic shape patterns on the surface of the posteromedial wall of the maxillary sinus. However, they must be recognized with the MPR and volume rendering tools before surgery. These 2 methods of CT reconstruction provide unparalleled planning. Unfortunately, in patients with opacification of the maxillary sinus, 3D images are often far from perfect, and the surgeon must rely mainly on the MPR.
A possible disadvantage of trans-SMP sphenoidotomy is that if the natural ostium is not included in the dissection, there is a possibility of mucous recirculation. All our patients required wide opening of the sphenoid sinus including the natural ostium, and we did not observe this phenomenon.
We found this method useful, safe, and time-saving in patients with the SMP prominence requiring wide opening of the sinuses. In one of our patients with a hypoplastic sphenoid sinus and well-pneumatized MRSS, we found it easier to breach the SMP than to perform any other type of sphenoidotomy. In patients without the SMP prominence, trans-SMP sphenoidotomy can be more time-consuming and may require a near bloodless operative field.
Conclusion
The SMP is present in approximately 35% of Caucasian subjects at least on one side. Proper preoperative planning with the MPR and volume rendering in these patients enables safe sphenoidotomy through the SMP.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The publication was financed by the Medical University of Warsaw.