
Abstract

Significance Statement
We report a case of nasopharyngeal choristoma with features consistent with hairy cell polyp and compound odontoma arising from the skull base in a premature newborn. No such lesions in humans have been reported in the literature. The lesion presented as a mass arising from the nasopharynx and protruding from the oral cavity through a cleft palate defect. Successful resection through an endoscopic-assisted and trans-oral approach was performed at 20 days of age.
Pediatric Clinic
Institutional review board (IRB) approval has been obtained from West Virginia University to conduct this study. We report a case of nasopharyngeal choristoma with features consistent with hairy cell polyp and a compound odontoma arising from the nasopharynx in a premature newborn. A cleft palate was diagnosed prenatally, and a fetal lip mass was suspected based on ultrasound. The ultrasound exam was limited by maternal body habitus. The pregnancy was also complicated by type II diabetes mellitus, polyhydramnios, and severe preeclampsia leading to delivery by Cesarean section at 33 weeks’ gestation. At birth, a mass protruding from the oral cavity through a cleft palate defect was noted (Figures 1A and 1B). The patient was orally intubated initially for surfactant administration, with easy movement of the soft mass to the lateral aspect of the oral cavity, and then extubated to continuous positive airway pressure (CPAP). Karyotype analysis demonstrated standard male karyotype (46, XY). Pre-operative imaging, including MRI with and without contrast and a CT scan without contrast, demonstrated a soft tissue mass measuring 5 x 4 x 1.5 cm in size, arising from the nasopharynx and extending through a cleft palate. The mass contained bony tooth-like structures (Figures 1C and 1D), raising suspicion for a congenital teratoma. Agenesis of the corpus callosum was also noted. Nasopharyngeal mass protruding through a cleft palate defect in a premature newborn (panels A and B). Panel C shows pre-operative MRI T1 post-gadolinium sagittal cuts and panel D shows CT scan bone window sagittal cuts demonstrating a mass containing numerous areas of bone and teeth (asterisks) originating from the nasopharynx with no intracranial extension (arrow head).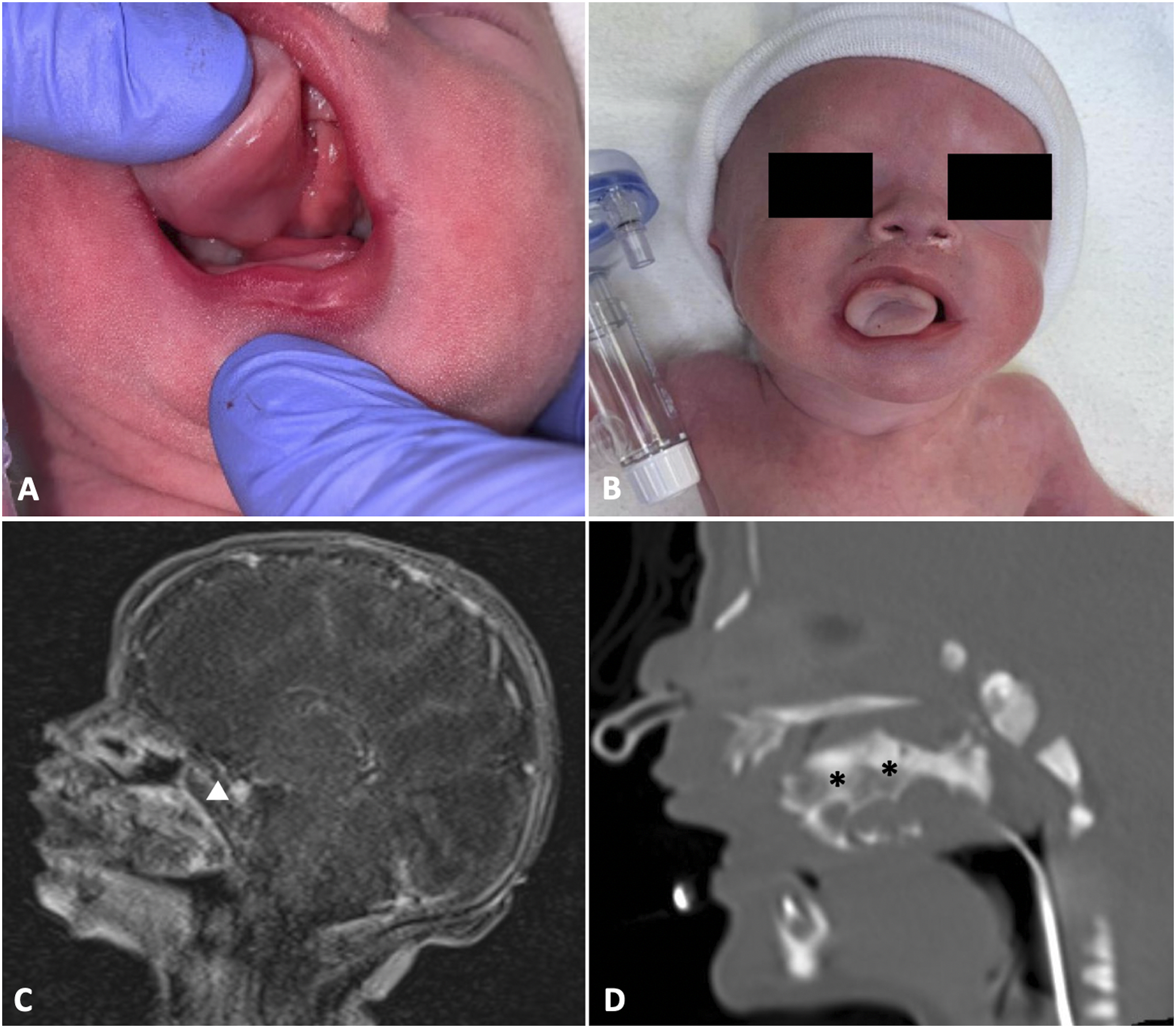
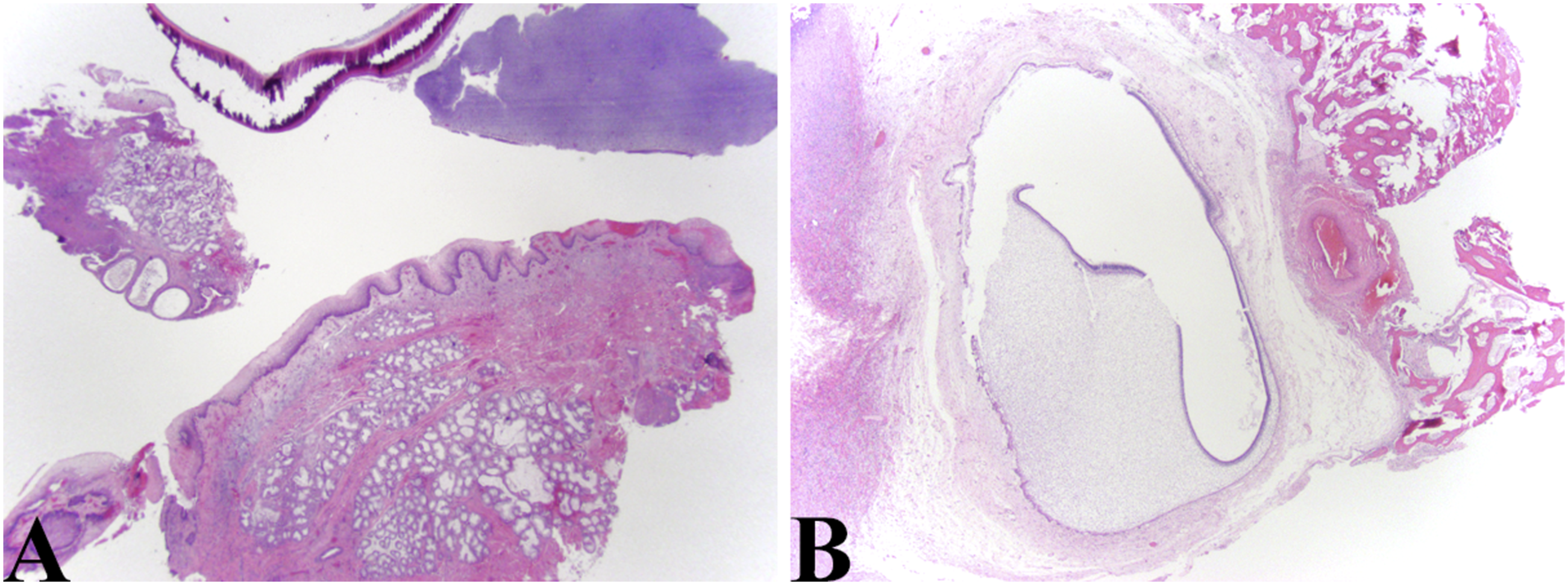
The mass was excised without complication at 20 days of age using a combined endoscopic endonasal and oral approach (Figure 2). Surgery timing was selected to allow maturation of the patient’s temperature control and apnea of prematurity and allow him to have more reserve to tolerate operative stressors. He also did not show significant airway obstruction at baseline, as he was able to transition to high-flow nasal cannula support with normal blood gases. The mass appeared to arise from the midline of the nasopharynx. Otologic microsurgical instruments were used to dissect the tumor at the base and sides of the nasopharynx and floor of the nose, and regular instruments were used to release the intraoral component. Minimal bleeding was encountered. The base of the stalk in the nasopharynx was cauterized with electrocautery (suction Bovie at the setting of 10). Direct laryngoscopy and rigid bronchoscopy were performed and demonstrated no additional airway anomalies. Surgical pathology found a choristomatous lesion consisting of skin with dermal adnexal structures, salivary gland tissue, and multiple tooth bells at varying stages of development resembling a compound odontoma (Figure 3). These characteristics, as well as the absence of endodermal elements, led to the diagnosis of a hairy polyp with features consistent with compound odontoma. Endoscopic intraoperative pictures of the tumor before excision (A) at its attachment in the nasopharynx and (B) after excision. Microsurgical instruments were used for excision (A). The site of attachment was cauterized after complete excision using suction Bovie at the setting of 10 (B). (A) Low magnification view of a polypoid mass covered by squamous epithelium with adnexal structure reminiscent of that seen in pre/post auricular skin tags. The top of the photo shows a portion of tooth (HE, 20X). (B) Photo depicts early developing tooth bell found in association with the polypoid soft tissue mass representing the hairy polyp (HE, 20X).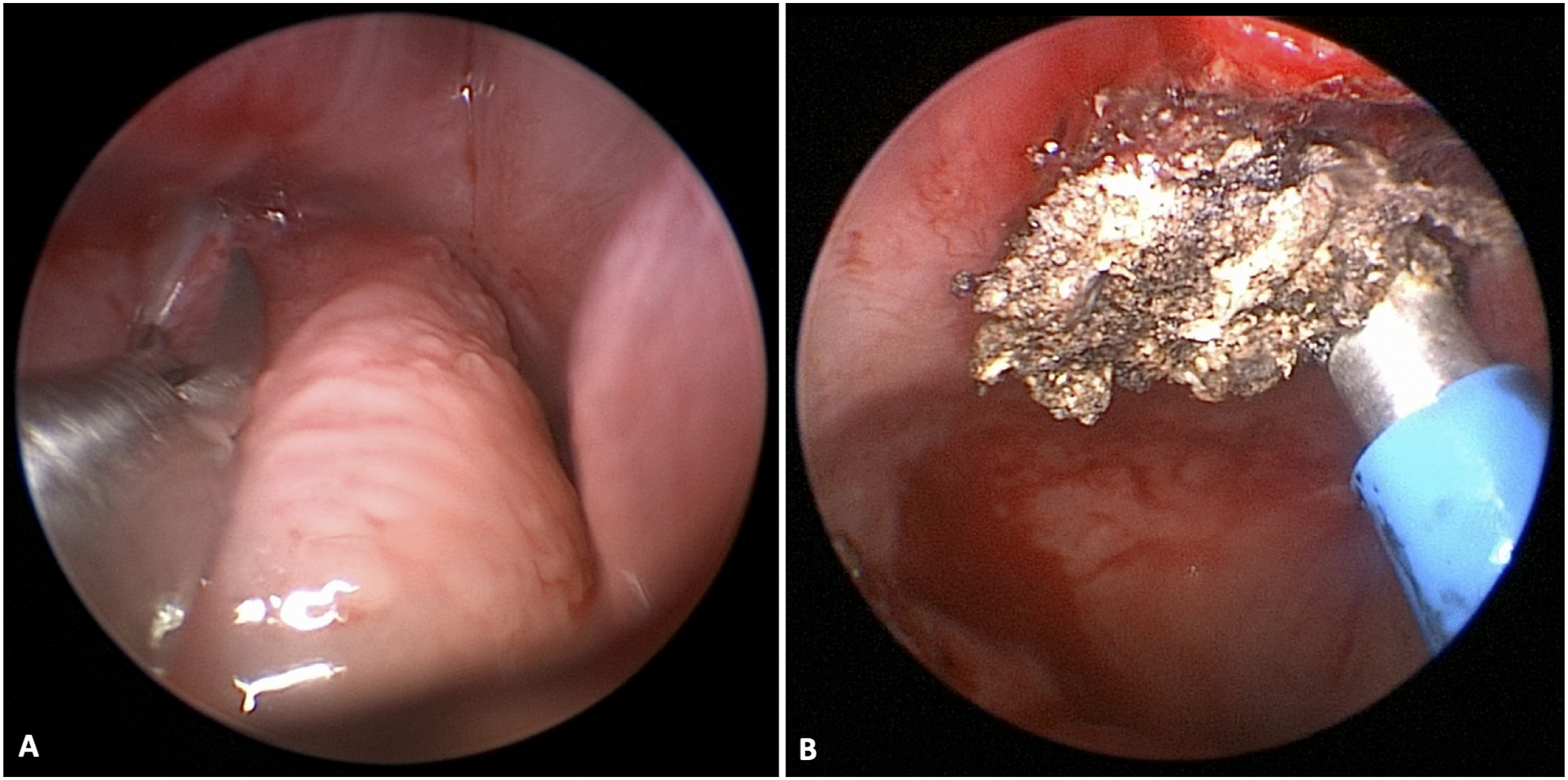
Patient did extremely well post-operatively. He was transitioned to room air within 2 days after mass removal. He was able to take adequate oral feeds using a specialty cleft palate bottle. After gaining weight well on oral feeds, he was discharged home on post-operative day twelve (32 days of age). He was last seen at 18 months post-operatively with no evidence of tumor recurrence.
Discussion
Congenital hairy polyps are rare benign lesions of ectodermal and mesodermal origin that most commonly arise as pedunculated masses in the oropharynx and nasopharynx.1,2 Given their location, clinical manifestations may include airway and/or feeding difficulties. 2 These can be associated with other abnormalities, such as cleft palate. 3 Hairy polyps that include features consistent with compound odontoma have been reported in veterinary literature. 4 However, no such lesions have been previously reported in humans.
Nasopharyngeal and oral cavity tumors are rare in neonates, and these tumors are of particular importance due to their potential for airway obstruction. These tumors may be benign or malignant and include congenital granular cell tumors, teratomas, rhabdomyosarcomas, nasal neuroglial heterotopia, vascular malformations, craniopharyngioma, and others.
We report the first known human case of nasopharyngeal choristoma with features of both congenital hairy polyp and compound odontoma. Absence of endodermal elements distinguished this lesion from the more common diagnosis of teratoma, which is also rare and are composed of all three germinal layers—ectoderm, mesoderm, and endoderm. 5 As is often observed with congenital nasopharyngeal teratomas, our patient’s mass was noted to be pedunculated and protruding through a cleft palate into the oral cavity. 5 Early surgical intervention was pursued in our patient given the size and location of the lesion and the resulting airway obstruction. The patient was doing well with no evidence of recurrence at most recent follow-up. Repair of the patient’s cleft palate will be performed at approximately 1 year of age.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.