
Abstract

Temporomandibular joint (TMJ) herniation is a rare condition and was first described by Hawke et al in 1987. 1 Patients with TMJ herniation may have symptoms such as hearing loss, otorrhea, clicking tinnitus, ear fullness, squeaking noise sound, and facial swelling. 2 Here, we report a patient diagnosed with left TMJ herniation.
A 59-year-old man with a history of hypertension and dyslipidemia under regular control came to our department with a complaint of left ear clicking sound at mouth opening and closing. He denied any trauma, infection, or operation history. Otoscope revealed a protruding mass over the anterior wall of his left external auditory canal when his mouth closed. (Figure 1A) The protruding mass became flattened when his mouth was opened. (Figure 1B) Audiometry appears to be completely normal. (Figure 1C) Temporal bone computed tomography was arranged and revealed dehiscence at the anterior wall of the left external auditory bony canal (Figure 1D, arrow). Conservative management was recommended, and the patient is asked to avoid heavy chewing and reduce his left TMJ load. The patient’s tinnitus disappeared within 4 weeks after this management, and under otoscopy, the extent of herniation decreased with the extrusion part of the ear canal no longer in touch with the tympanic membrane. (A) Otoscope revealed a protruding mass over the anterior wall of his left external auditory canal when the mouth closed. (B) The protruding mass became flattened when his mouth is opened. (C) Audiometry appears to be completely normal. (D) Temporal bone computed tomography was arranged and revealed dehiscence at the anterior wall of the left external auditory bony canal (arrow).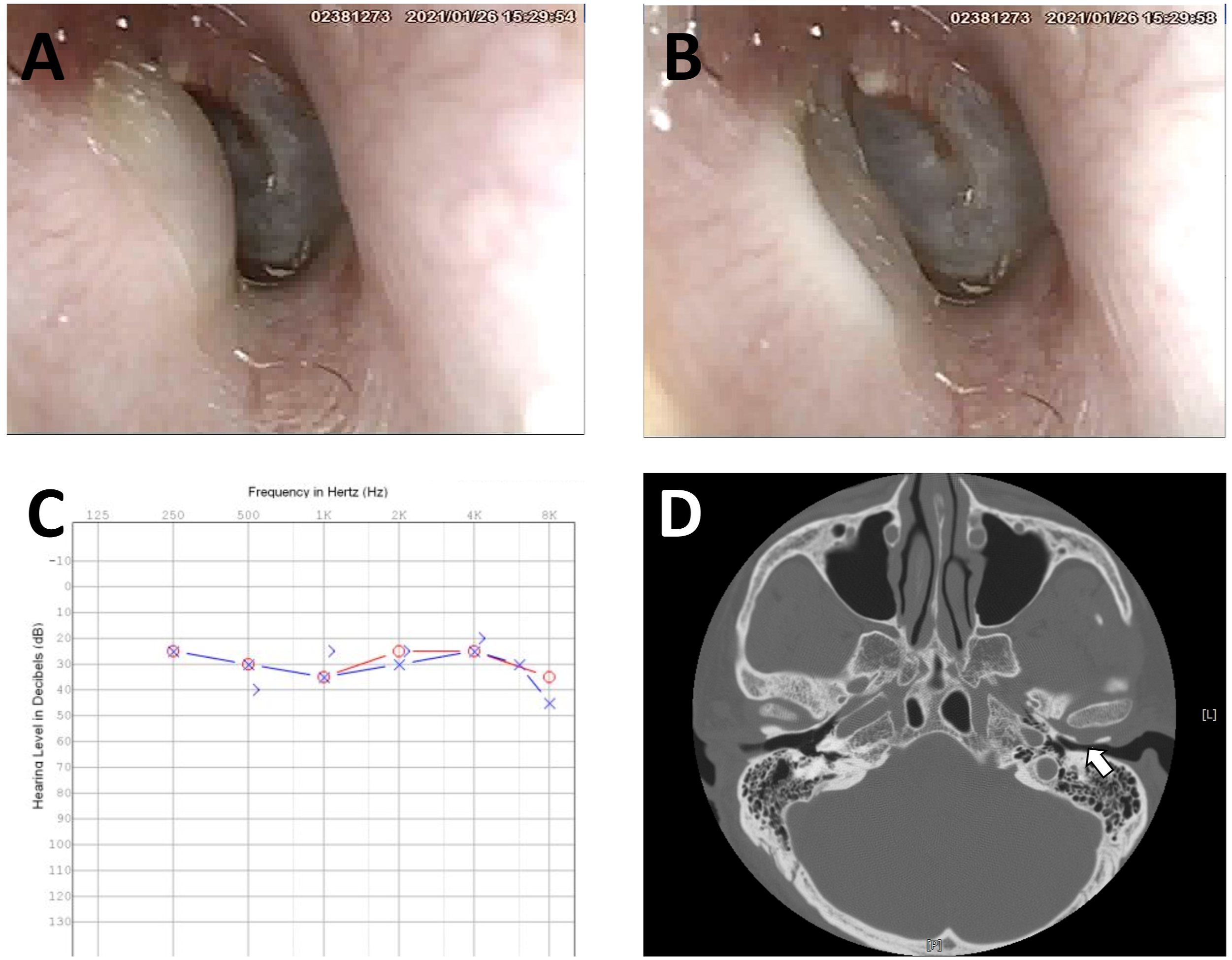
The etiology resulting in the TMJ herniation includes trauma, inflammation, iatrogenic, and spontaneous herniations. 2 The presence of the foramen of Huschke, occurring with an incidence of 4.6% of the population, could be a significant factor in developing spontaneous TMJ herniation. 3 Diagnostic examination of TMJ herniation can be made with dynamic otoscopy, computed tomography (CT), or magnetic resonance imaging. 4 The bony defect could be readily visualized through temporal bone CT, and under dynamic otoscopy; typically, a mass protruding anteriorly from the posterior ear canal during mouth opening and closing can be easily observed.
Management of the TMJ herniation depends on the symptoms and cause of the herniation. Surgical repair with tragal cartilage, polypropylene implant, or titanium meshes can be considered in severe cases. 5 Conservative management often includes avoiding chewing foods on the affected side and can be a good alternative. There were less than 60 cases of TMJ herniation reported in the related English literature. In most cases, the mass appeared to be with a smooth surface and rarely to be polypoid. 2 Although whether a polypoid appearance of this lesion suggests a non-congenital nature remains to be debated, to the best of our knowledge, the case reported here appears to be the first Taiwanese case with a smooth surface TMJ ear canal herniation in the existing literature.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.