
Abstract
Orbital schwannoma is a rare benign tumor, originating from the Schwann cells of the orbital peripheral nerve sheath. Orbital schwannoma is easily misdiagnosed if the patient shows atypical presentations and atypical appearance on MRI imaging. A 56-year-old male experienced hyposmia for 1 year and was misdiagnosed with cavernous hemangioma pre-operation. This case was treated by surgery through the endoscopic trans-nasal approach. After operation, the patient had no recurrence or complications. Preoperative diagnosis for these cases remains difficult. Combined imaging modalities including computed tomography (CT) and magnetic resonance imaging (MRI) can help in differential diagnosis. Surgery is the main treatment modality for treating orbital schwannoma. Outcomes in most cases are favorable without complications or recurrence.
Keywords
Introduction
Orbital schwannoma is a rare tumor, originating from Schwann cells of the orbital peripheral nerve sheath.1,2 Orbital schwannomas are commonly benign and slow-growing with a long disease course. In some cases, orbital schwannoma with a cyst formation may grow rapidly. 3 Preoperative diagnosis of orbital schwannomas is still difficult, which depends on multiple imaging modalities including ultrasonography, computed tomography (CT), and magnetic resonance imaging (MRI). Due to the varied appearances of lesions on various imaging modalities, imaging results should be comprehensively considered for differential diagnosis.
Complete surgical excision is the main treatment for orbital schwannoma. Orbital surgery is complex because of the anatomic restrictions and related vital anatomic structures. The endoscopic trans-nasal approach has been used for treating various orbital tumors including orbital schwannoma.4-7 Endoscopic approach is minimally invasive which has advantages in improving visualization and accessing to the medial and inferior orbit safely.
Herein, we report a case of orbital schwannoma with atypical presentations. This case was treated by surgery through a trans-nasal endoscopic approach. We also made a literature review focusing on differential diagnosis and treatment of orbital schwannoma.
Case presentation
A 56-year-old male patient visited the otolaryngology department in a local hospital because of hyposmia for 1 year. CT imaging of paranasal sinus revealed a mass in the left intracanal area. The patient then was transferred to our hospital. He had no other medical conditions except hypertension and a blood pressure of 144/81 mmHg upon admission. No abnormal swelling was found on the face or his left eye. Nasal endoscopy examination revealed no abnormal results. Neurological examination detected no neurological deficits. Blood routine, chemistry, and tumor markers’ tests were all normal. Ophthalmic examination, visual fields, pupillary responses, color vision, ocular movement, and fundus examinations were all normal in both eyes. He underwent a computed tomography (CT) scan which revealed a well-defined dumb-bell mass (size: .8 cm x .6 cm) in the extraconal and intraconal compartment of the orbital superomedial quadrant (Figure 1(A)). Further orbital enhanced MRI revealed a mass in the orbital region and across the extraconal and intraconal compartments. Cranial CT showed no other abnormal results. The mass was suspected to be a hemangioma. (A) Preoperative computed tomography scanning of the mass. The asterisk indicates a well-defined dumb-bell mass in the left intracanal area; (B) Postoperative computed tomography showing the tumor completely removed.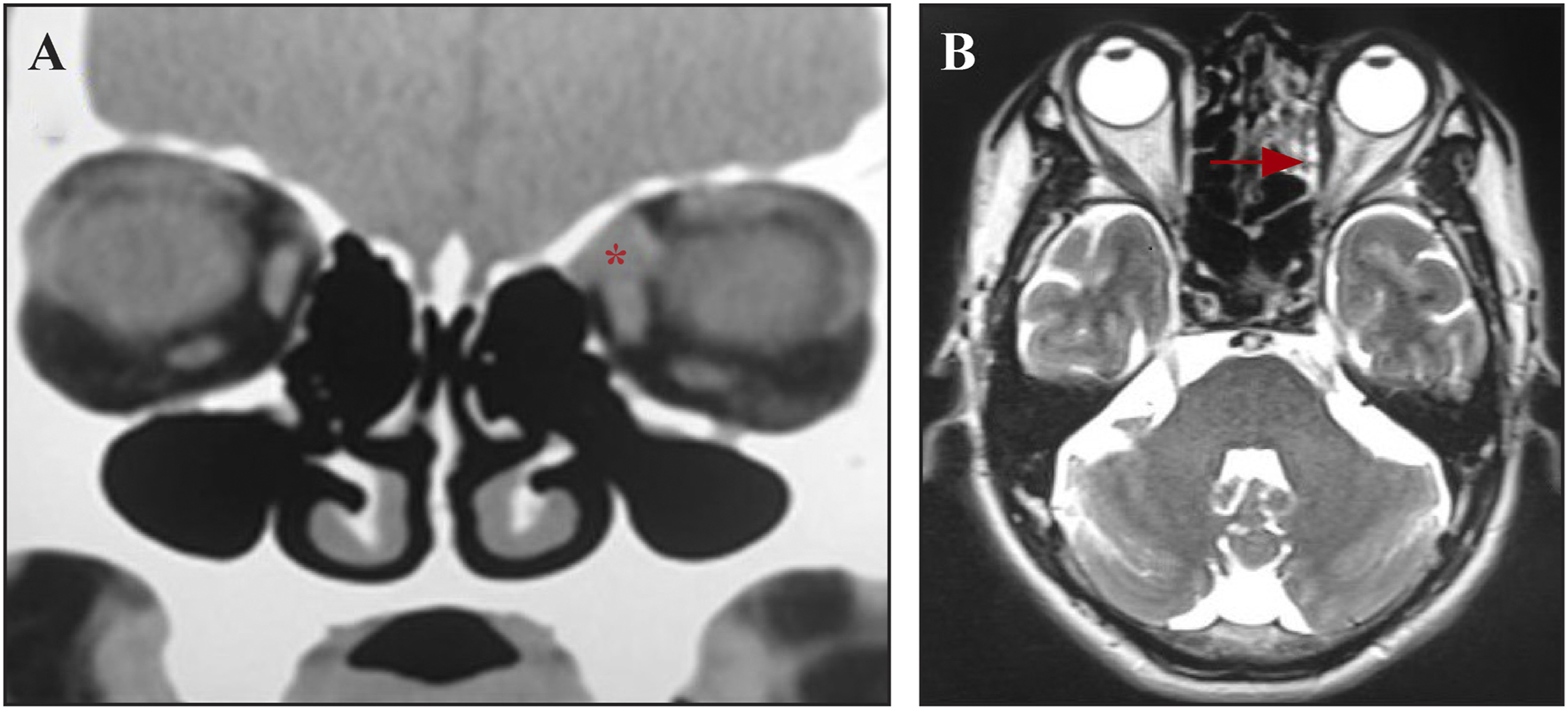
An intranasal endoscopic ethmoidectomy was undertaken to expose the medial orbital wall. During the operation, a mass was found located in the medial orbital wall with some extension into the intraconal space. The lamina papyracea was removed, and the periorbita was incised; then, a blunt probe dissector teased apart the mass and its surrounding normal tissue carefully. The intraconal fat was extracted to expose the tumor completely, and the mass was removed completely (Figure 2(A)). The final histopathological examination revealed spindle-shaped tumoral cells in the mass which confirmed an orbital schwannoma (Figure 2(B)). (A) Macroscopic view of tumors after surgical removal; (B) Histopathological analysis showing dense spindle cells palisading, with oval and fusiform nucleus.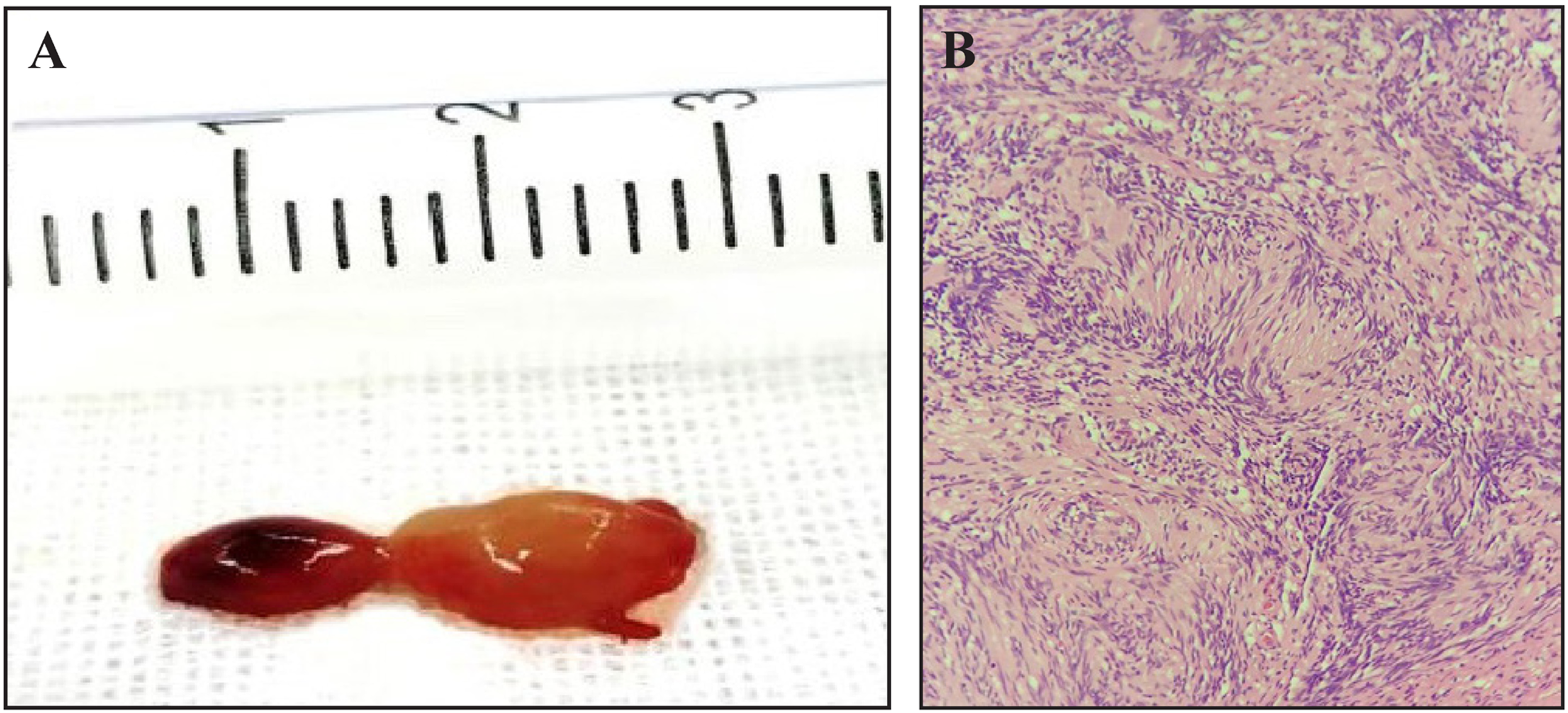
The patient had an uneventful postoperative clinical course. CT examination revealed a total resection of the mass (Figure 1(B)). Olfactory function recovered 1 month after operation. No recurrence or any complications were found at 13 months after operation.
Discussion
Schwannoma is a benign neoplasm, originating from Schwann cells of cranial, intraspinal, peripheral, and autonomic nerve sheaths, which accounts for 1%–8% of head and neck tumors. 8 Orbital schwannomas are rare, accounting for 1% to 4% of orbital tumors. 7 Early diagnosis is very important for early treatment and better outcome.
Orbital schwannoma commonly presents as chronic progressive protopsis, orbital mass and vision loss, visual impairment, and painful eye. 8 Our patient only presents with hyposmia which is rarely reported in previous cases.
CT and MRI characteristics of orbital schwannomas and orbital cavernous hemangioma.
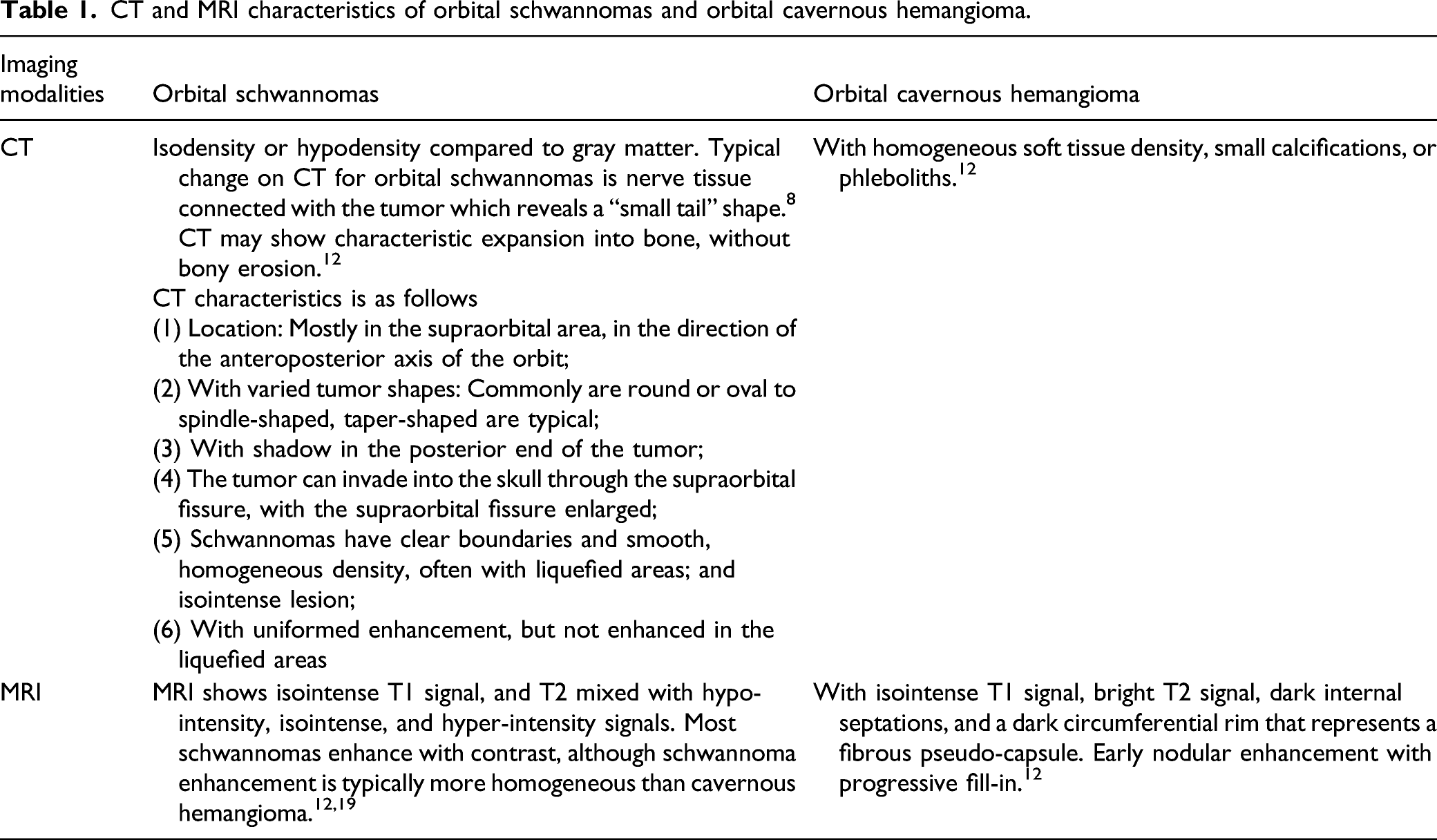
Orbital MRI may be better than CT for accurately qualitative diagnosis of orbital schwanoma. And MRI can detect the clearer and more accurate lesion location and involving area. Based on different density signals, MRI can differentiate orbit schwannoma from cavernous and meningiomas or other soft tissue tumor. Compared with cavernous hemangioma, schwannoma has a lower T2 signal and volume effect in MRI. 14 Schwannoma enhancement is typically more homogeneous than cavernous hemangioma. 12 MRI also shows mixed hypo-, iso-, and hyper-intensity signals in T2-weighted images. Our experience from this misdiagnosed case is that pre-MRI should be performed and carefully evaluated. MRI maybe considered as the initial imaging modality for diagnosis and treatment of orbital schwannomas. Preoperative examination with CT and MRI is valuable for diagnosis and treatment of orbital schwannomas.
For treatment of orbital schwannomas, surgical removal of the tumor remains a major option. Appropriate approaches should be selected by the extent and location of the tumors. Several surgical approaches to the orbit tumors have been reported, such as lateral orbitotomy, trans-conjunctival, supraorbital, pterional, contralateral pterional, and the endonasal approaches.15-18 In our case, the mass was located in the intracanal area, so we used intranasal endoscopic ethmoidectomy. Endoscopy permits wide angle and high brightness, leaving no facial scar, and complete tumor removal. However, the surgical procedure should be performed by experienced nasal surgeons who are familiar with nasal and eye-related anatomy.
Most cases with orbital schwannomas have good outcome without recurrence and malignant transformation. Our case had no complications or recurrence after 13 months of follow-up. Therefore, complete resection of the tumor is important for better outcome.
Though with a rare entity, orbit schwannoma should be considered as a differential diagnosis with other orbital tumors. Preoperative CT and MRI should be performed for early diagnosis and better treatment. The endoscopic endonasal approach can completely remove the orbit schwannoma leaving no complications or scar.
Footnotes
Author contributions
Lou XY conceptualized this study, made the literature review, and wrote the first draft of this paper; Jiang B, Zhong JG, Zhong JG, and Wang HB made the literature review. All authors revised the paper and approved the final version for submission.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.