
Abstract
Introduction
Despite the presence of clinical practice guidelines for overnight admission of pediatric patients following adenotonsillectomy, variance in practice patterns exists between pediatric otolaryngologists. The purpose of this study is to examine severity of apnea–hypopnea index (AHI) as an independent predictor of postoperative respiratory complications in children undergoing adenotonsillectomy.
Methods
Retrospective chart review of all children undergoing adenotonsillectomy at a large tertiary referral center between January 2015 and December 2019 who underwent preoperative polysomnography and were admitted for overnight observation. Charts were reviewed for total adverse events and respiratory events occurring during admission.
Results
Overall, respiratory events were seen in 50.6% of patients with AHI ≥10 and in 39.6% of patients with AHI <10. The overall mean AHI was 19.2, with a mean of 28.1 in the AHI ≥10 subgroup vs 4.6 in the AHI <10 subgroup. There was no statistical correlation or increased risk between an AHI ≥10 and having a pure respiratory event, with a relative risk of 1.19 (.77–1.83, P = .43). There was a statistically significant difference between the mean AHI of those with any adverse event and those without (21.6 vs 13.4, P = .008). There is additionally an increased risk of any event with an AHI over 10, with a relative risk of 1.51 (1.22–1.88, P < .0001).
Conclusion
Preoperative AHI of 10 events per hour was not a predictor of postoperative respiratory complications. However, there was a trend for those with a higher AHI requiring additional supportive measures or a prolonged stay. Practitioners should always use their best judgment in deciding whether a child warrants postoperative admission following adenotonsillectomy.
Keywords
Introduction
Pediatric adenotonsillectomy is one of the most commonly performed surgical procedures in the world with over 500,000 performed annually, accounting for 16% of all ambulatory surgeries in children up 16 years of age.1,2 Despite the release of clinical practice guidelines by the American Academy of Otolaryngology-Head and Neck Surgery (AAO-HNS) in 2011 and revised in 2019, there remains little evidence to guide clinicians in their postoperative monitoring and management of pediatric patients following adenotonsillectomy. 3 A large variance in practice patterns exists between institutions regarding post-adenotonsillectomy admission criteria,1,4 and there is no current consensus among pediatric providers for severity of preoperative apnea–hypopnea index (AHI) seen on polysomnogram (PSG) which constitutes postoperative admission.
Concern for postoperative airway obstruction and apnea has increased in recent years in conjunction with the observed increase in percentage of adenotonsillectomies performed for obstructive sleep apnea (OSA) rather than recurrent or chronic tonsillitis.1,5 Children with severe OSA often have significant residual obstruction during the first night following their procedure, occasionally manifesting as respiratory compromise when the child falls asleep.6,7 Correlation has been demonstrated between severity of OSA based on AHI and risk of adverse overnight events postoperatively.3,8,9 However, the degree of OSA severity constituting postoperative admission continues to be a subject of debate, and although the AAO-HNS endorses an AHI of 10 events per hour as a cutoff for admission, the AAP endorses an AHI of 24; thus, there remains room for further study amidst a lack of consensus.10,11
The purpose of this study is to examine AHI severity as an independent predictor of postoperative complications in children undergoing adenotonsillectomy. Additionally, we seek to better understand the severity at which overnight admission for patients with sleep-study proven obstructive sleep apnea should be recommended. This would be helpful for other pediatric and general otolaryngologists to make more well-informed decisions regarding the postoperative care of their adenotonsillectomy patients potentially at risk for immediate postoperative complications.
Materials and methods
Retrospective chart review was performed of all patients who underwent adenotonsillectomy at the University of Texas Medical Branch between January 2015 and December 2019. Only pediatric patients were included in this study, with ages ranging from 18 months to 18 years. Charts were independently reviewed by study investigators, and patients were excluded from the study either if they did not have a preoperative sleep study or if they were discharged on the same day as surgery. Next, the following data points obtained: patient age, gender, obesity (BMI >95th percentile), minimum oxygen saturation (%) during admission, reason for adenotonsillectomy (obstructive sleep apnea, recurrent tonsillitis, or other), number of desaturation events (oxygen saturation <90%), supplemental oxygen requirement during the admission, need for PICU admission, need for prolonged stay (defined as > 24 hours), need for supplemental narcotic pain medication during admission, need for supplemental steroids, pulmonary edema, laryngospasm, and bronchospasm. The following data were obtained from preoperative polysomnography: apnea–hypopnea index (AHI), respiratory disturbance index (RDI), and minimum oxygen saturation (%).
Each of the data points was subcategorized as either “respiratory events” or “non-respiratory adverse events.” Respiratory events were defined as the following: desaturation events (SpO2 < 90%), supplemental oxygen requirement, administration of inhaled medications (ie, albuterol, racemic epinephrine), pulmonary edema, laryngospasm, or bronchospasm. Non-respiratory adverse events were defined as prolonged hospital stay (>24 hours), need for unplanned PICU admission, need for supplemental narcotics, steroids, or antibiotics. “Total events” included respiratory events plus non-respiratory adverse events. Additional subgroup analysis was performed for patient comorbidities including obesity, asthma/reactive airway disease, Down syndrome/developmental delay, and cerebral palsy.
This study met Institutional Review Board (IRB) approval, and all patient information and data were collected and protected following guidelines set forth by both our institution’s IRB and HIPPA regulations. Data and statistical analysis were performed using SAS 9.4 (SAS Institute, Cary, NC) and Prism 8 (GraphPad Software, San Diego, CA). Averages and percentiles were calculated for all data. Pearson’s r coefficients were calculated. Unpaired T-test was used to determine the statistical significance between continuous variables; relative risk values and two-tailed Fisher’s exact test were calculated for categorical variables. P values less than .05 were considered significant.
Results
Summary of data obtained via chart review including patient demographic information as well as sleep study data, overnight events, and calculated events per patient. Data are additionally grouped according to AHI ≥10 and AHI >10.
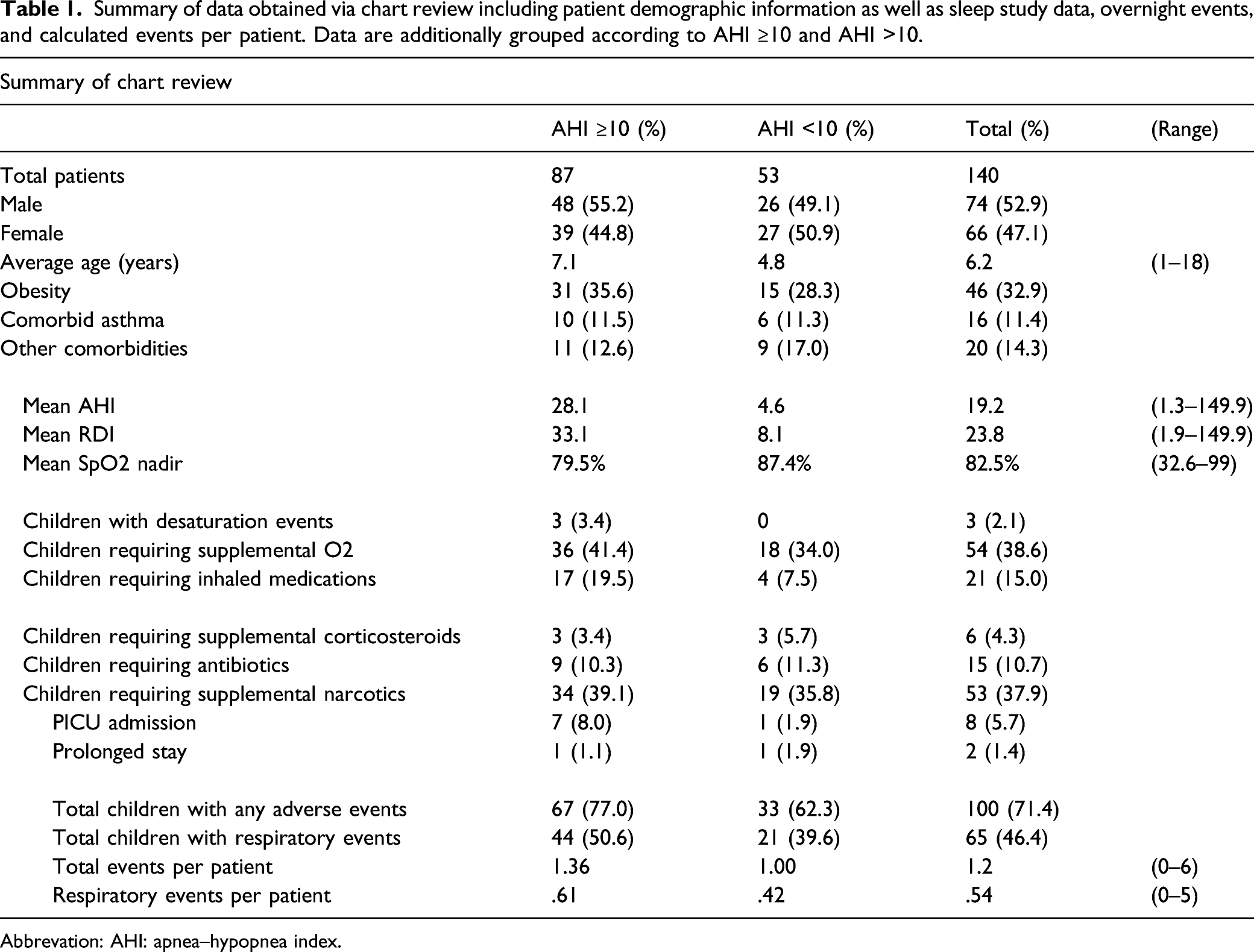
Abbrevation: AHI: apnea–hypopnea index.
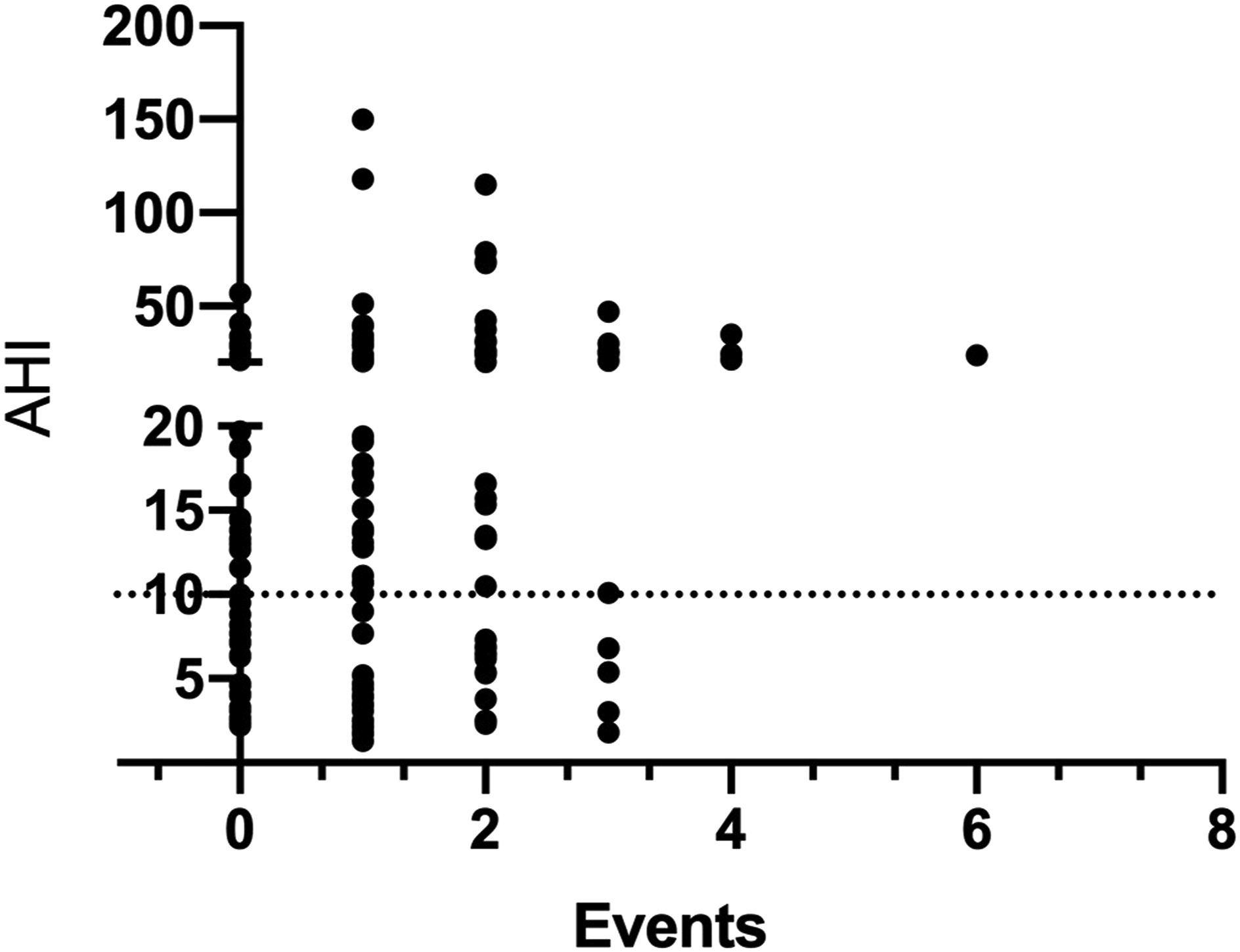
Scatterplot depicting pooled distribution of total overnight events vs AHI. The dotted line signifies an AHI of 10. AHI: apnea–hypopnea index.
Overall, the most common respiratory-related adverse event was requirement of supplemental oxygen (n = 54, 38.6%) followed by requirement of supplemental inhaled respiratory medications (n = 21, 15.0%), with 19.5% of patients with AHI ≥10 requiring inhaled medications vs 7.5% of patients with AHI <10. There were 6 desaturation events of SpO2 < 80% reported in 3 patients. There were no reports of bronchospasm, laryngospasm, or pulmonary edema.
The most common non-respiratory-related adverse event was requirement of supplemental narcotic pain medications (n = 53, 37.9%), which were administered either in the PACU by the anesthesia team, on the pediatric floor, or in the PICU. Due to presumed upper respiratory infection or tonsillitis either at the time or surgery or in the immediate postoperative period, 15 children (10.7%) required oral or intravenous antibiotics, and 6 children (4.3%) required supplemental corticosteroids. A total of 8 children were admitted to the PICU, with 5 of these being planned PICU admissions (62.5%) and 3 being unplanned (37.5%). The mean AHI of children admitted to the PICU was 82.8 (range 6.5–149.9). There were no reported cases of postoperative bleeding in this cohort.
AHI ≥10 Versus AHI <10
Subgroup analysis was then performed for patients with AHI ≥10 events per hour and AHI <10 events per hour. There was no statistical association between an AHI ≥10 and having a pure respiratory event, with a relative risk of 1.19 (.77–1.83, P = .43). There was no difference in the mean AHI between those with a respiratory event and those without (P = .82). However, there was a statistically significant difference between the mean AHI of those with any adverse event and those without (21.6 vs 13.4, P = .008). There is additionally an increased risk of any event with an AHI over 10, with a relative risk of 1.51 (1.22–1.88, P < .0001).
Relationship between AHI and adverse events
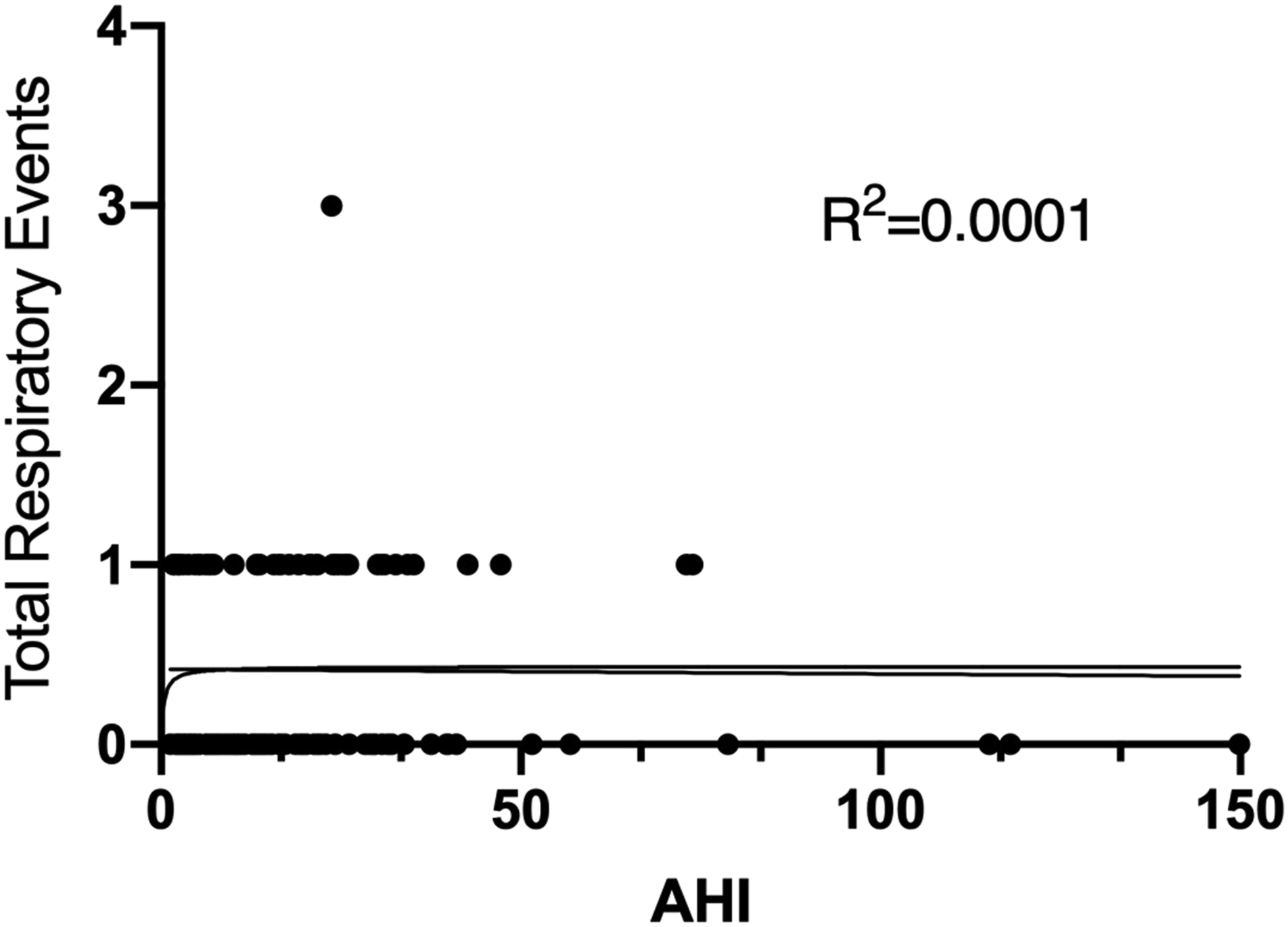
Linear and logistic regression modeling was performed based on AHI vs total adverse events and respiratory events, respectively (Figure 2 and Figure 3). Pearson product-moment correlation coefficients were calculated, revealing a weakly positive correlation between AHI and total adverse events (r = .13). However, the slope of this data was not significantly different than zero, showing no trend or predictive model. There was no correlation between AHI and respiratory events (r = −.01). Linear and logistic regressions modeling AHI vs total adverse events (respiratory events plus non-respiratory adverse events). There was no predictive model or significant trend. AHI: apnea–hypopnea index. Linear and logistic regressions modeling AHI vs respiratory events (oxygen desaturation, need for supplemental oxygen, laryngospasm/bronchospasm, and need for inhaled medications). As with total adverse events, there was no predictive model or significant trend. AHI: apnea–hypopnea index.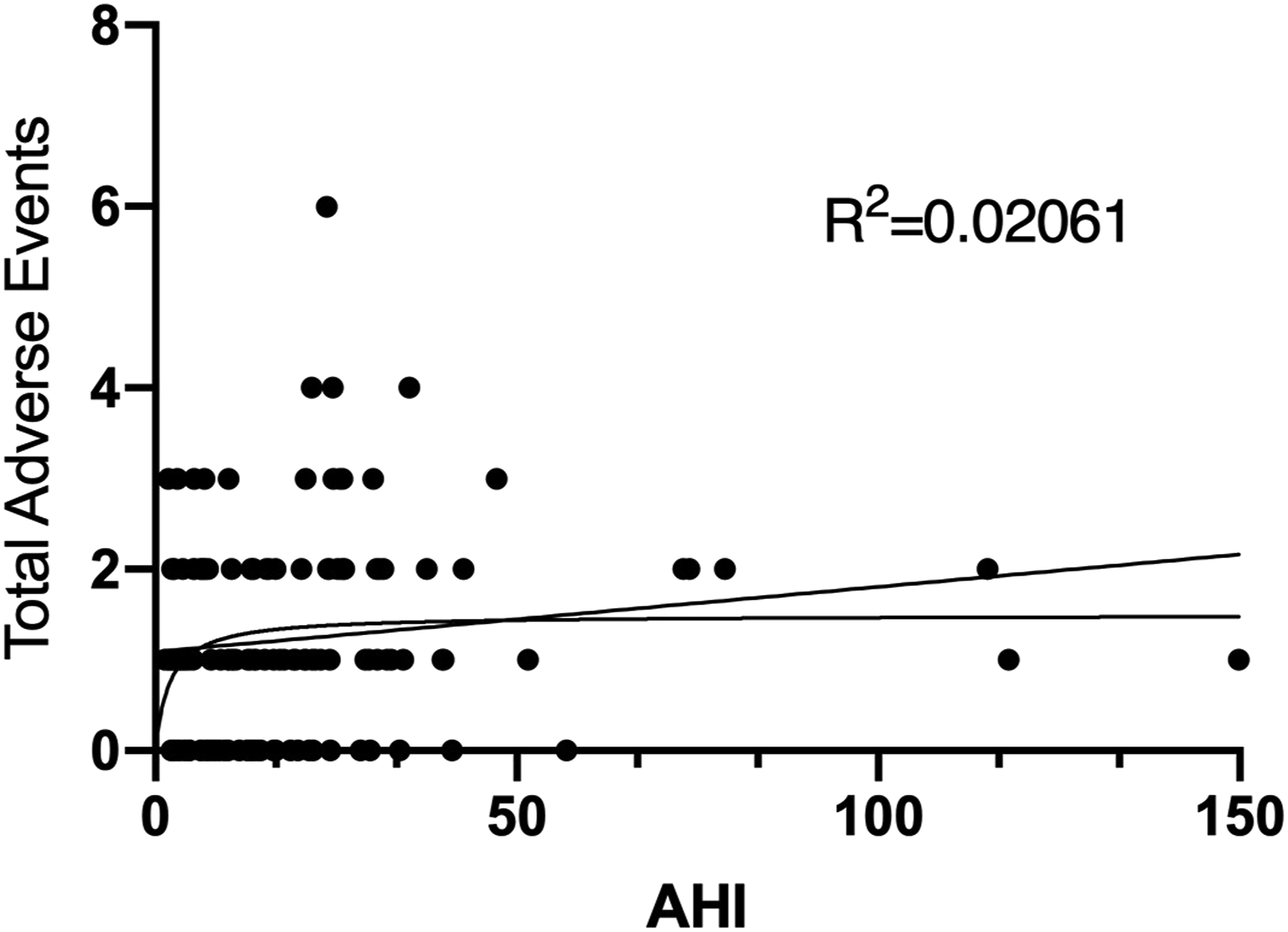
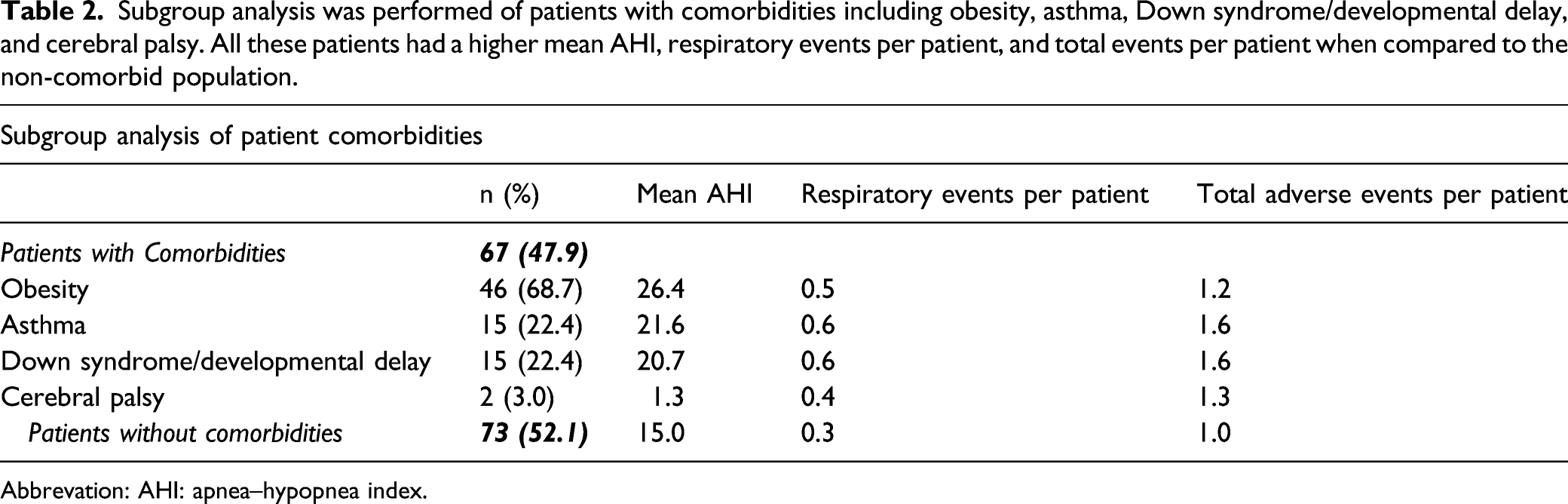
Subgroup analysis of comorbidities
Subgroup analysis was performed of patients with comorbidities including obesity, asthma, Down syndrome/developmental delay, and cerebral palsy. All these patients had a higher mean AHI, respiratory events per patient, and total events per patient when compared to the non-comorbid population.
Abbrevation: AHI: apnea–hypopnea index.
Discussion
Polysomnography has become an indispensable tool in preoperative evaluation of children with OSA undergoing adenotonsillectomy, since it can be used to predict which children are at risk of devastating postoperative respiratory complications.3,8,9 Per Key Action Statement 12 of the 2019 Clinical Practice Guideline: Tonsillectomy in Children (Update), inpatient admission is recommended by the AAO-HNS for all children with severe OSA, defined as documented AHI ≥10 events per hour.10,11 The guideline authors noted in their recommendations that debate persists regarding what should be considered as truly severe sleep apnea. Disagreements continue as providers look to use AHI as a reference that not only describes current severity of OSA but also predicts post-surgical respiratory complications and potential need for admission following surgery.
Evidence of lack of consensus regarding post-adenotonsillectomy admission is illustrated well by adherence rates to current AAO-HNS guidelines. Many tertiary care children’s hospitals in the United States do not have an official policy regarding which patients require inpatient admission following adenotonsillectomy, despite the existence of clinical practice guidelines.1,12,13 A cross-sectional study by Nardone et al 1 in 2016 showed that 40% of pediatric otolaryngology chiefs at tertiary care children’s hospitals used the AAO-HNS polysomnographic criteria for severe OSA as post-tonsillectomy admission criteria. 1 This was corroborated by a similar 2019 cross-sectional study showing a 37% adherence rate to these criteria. 12 Conversely, the Nardone study showed only 15% of respondents used the American Academy of Pediatrics (AAP) criteria for severe OSA, 1 which they define as AHI >24 or oxygen saturation nadir <80%. Indeed, the 2012 recommendations endorsed by the AAP include an AHI cutoff of 24 rather than 10 events per hour, as endorsed by the AAO-HNS. 13 The authors note that this recommendation was based on the limited evidence available at the time, with most studies reporting a wide variation in postoperative respiratory events or complications. This may be at least in part explained by varying proportions of patients included with syndromes, craniofacial abnormalities, neuromuscular disorders, and obesity, and studies define respiratory complications in a non-standardized way.
Incidence of major post-adenotonsillectomy respiratory complications has been reported between 1.4% and 5%. 5 One retrospective cohort study of 167 patients found preoperative AHI of 44 as an identifiable risk factor for respiratory complications 14 —however, this study was performed at an elevation over 2500 m, and it is difficult to determine generalizability given these environmental variables. One of the largest studies to date examining risk factors for postoperative desaturation after tonsillectomy identified OSA as one of seven independent risk factors, also including obesity, trisomy 21 or another syndrome, cardiac or neurologic comorbidity, and pulmonary disease. 15
A 2011 retrospective study by Hill et al. reviewed 83 children with severe obstructive sleep apnea who were admitted overnight after adenotonsillectomy with major and minor airway complications occurring in 4.8% and 19.3% of children, respectively. 5 The authors found AHI >24, age <2 years, intraoperative laryngospasm, oxygen desaturation in the PACU, and prolonged PACU stay as predictive of postoperative airway complications. Nonetheless, the authors did not find AHI ≥10 as a predictor of complications. Similarly, another retrospective review from 2016 examined 86 patients who underwent overnight admission after adenotonsillectomy, and the authors found a statistically significant association between AHI ≥40 and postoperative respiratory complications. 16 The association between postoperative respiratory complications and AHI ≥25 was only marginally significant, and no respiratory complications were found in children with an AHI <10. Another 2015 retrospective review similarly examined 157 patients and found an AHI ≥15 to be an independent predictor of postoperative desaturation below 90% SpO2 and prolonged length of stay. 3 However, this study found polysomnographic SpO2 nadir <80% to more strongly predict postoperative complications than AHI.
This study showed no significant association between AHI and postoperative respiratory events following adenotonsillectomy in children. Although a weakly positive correlation was seen between AHI and total adverse events, this should be interpreted with caution, given that total events included supplemental measures for non-respiratory-related complications and may not be significant when interpreted in this context. Another notable finding seen was the higher number of both respiratory events per patient and total adverse events per patient in those with comorbidities including obesity, asthma, Down syndrome/developmental delay, and cerebral palsy. Although the sample size of these patients was too small to reach statistical significance, these findings could be suggestive of a greater likelihood of respiratory complications in these patients.
The present study is not without weaknesses. As with any retrospective chart review, data analysis and interpretation rely on the accuracy and completeness of the electronic medical record. Since only patients with preoperative PSGs were included, there was a possible selection bias against cases in which adenotonsillectomy was performed but no preoperative PSG was obtained. This could be due to PSG being deferred by the provider due to the diagnosis of OSA being clinically apparent, or it could be due to surgery being performed for a reason other than OSA, such as recurrent tonsillitis. Therefore, these data must be interpreted with the context in mind that this population of patients all had confirmed OSA shown by preoperative PSG. Additionally, this study was limited by relatively small sample size, and larger studies, perhaps with pooled patient populations or meta-analyses, would allow for a more robust interpretation. Several confounding factors were not controlled for including obesity, comorbidities, and perioperative analgesic protocol. Finally, data regarding non-respiratory-related adverse events should be interpreted with caution, as the severity of OSA might not necessarily contribute to these events, such as need for supplemental narcotics, steroids, or PICU admission.
Although our study showed no statistically significant difference in respiratory events when using AHI of 10 as a cutoff, further investigation is needed to definitively recommend a specific AHI as criteria for admission. We advocate for a holistic approach, one that not only considers AHI but also intrinsic patient factors such as age, comorbidities, and complicating social history, or adverse events observed upon awakening and recovery, when determining which children require post-adenotonsillectomy admission. When determining the need for preoperative PSG prior to tonsillectomy, however, the authors would generally advocate this study in all children with craniofacial abnormalities and in those children with a discordance in their physical examination and reported severity of symptoms, as recommended in the AAO-HNSF Clinical Practice Guideline: Polysomnography for Sleep-Disordered Breathing Prior to Tonsillectomy in Children.
Conclusions
In this limited study population, preoperative AHI of 10 events per hour was not a predictor of postoperative respiratory complications. More research will be needed for more complete understanding of the significance of the severity of AHI in the post-adenotonsillectomy setting. However, we would advocate for an individualized patient-centric approach that not only utilizes the AHI but also considers other factors such as comorbidities, distance of the patient’s home from the hospital, and age, as the AHI cutoff of 10 events per hour might not be sufficient to determine need for admission in all scenarios. Practitioners should always use their best judgment in deciding whether a child warrants postoperative admission following adenotonsillectomy.
Footnotes
Acknowledgment
The authors acknowledge the University of Texas Medical Branch Department of Otolaryngology-Head and Neck Surgery for academic support of this project.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.