
Abstract
Background
Fine needle aspiration (FNA) is a common diagnostic tool used in the initial evaluation of parotid masses. In the literature, variable diagnostic accuracy of FNA is reported. Therefore, when considering clinical management of these patients, the utility of FNA is unclear. The aim of this study was to determine the capability of ultrasound-guided FNA to differentiate between benign and malignant neoplasms. Further, the way in which FNA results affect clinical decision-making was assessed.
Methods
Retrospective data were collected for all patients who underwent parotidectomy at a large Canadian tertiary care center between 2011 and 2016. Patient demographics, preoperative imaging reports, preoperative FNA results, and final pathological diagnosis were analyzed.
Results
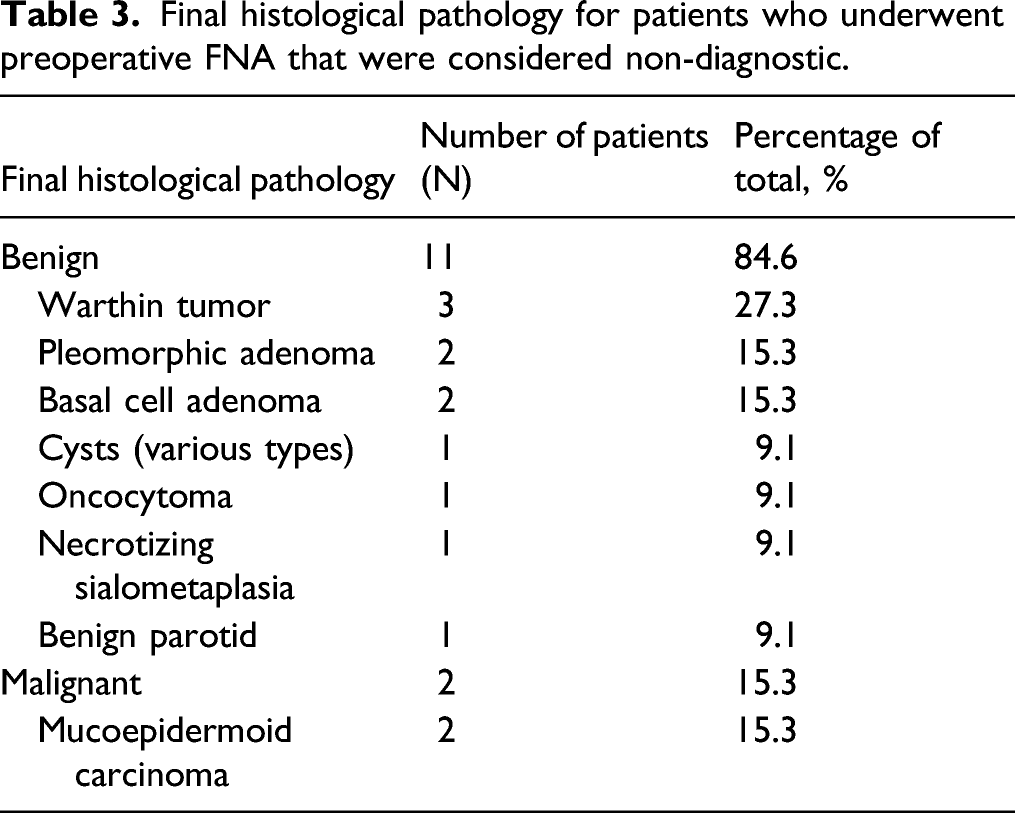
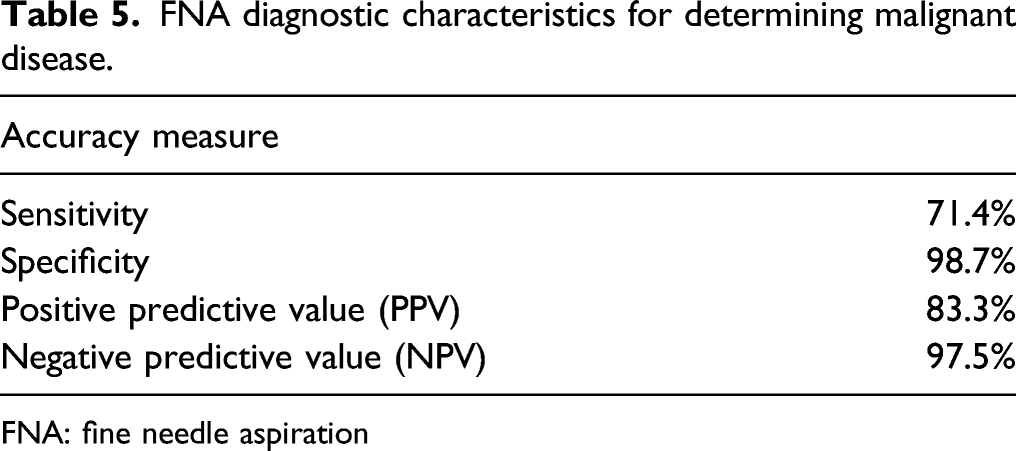
Of the 199 patients who underwent parotidectomy, 184 had preoperative ultrasound-guided FNA. There were a total of 13 non-diagnostic FNAs. In diagnosing malignancy, FNA had a sensitivity and specificity of 71.4% and 98.7%, respectively. The positive predictive value (PPV) was 83.3%. The negative predictive value was 97.5%. Of the non-diagnostic FNAs, 2 out of 13 (15.4%) were deemed malignant neoplasms on final pathology.
Conclusion
FNA is a useful adjunct in the work-up of parotid masses, but it should be used with caution. Due to limited sensitivity, it should not be relied upon as the sole determinant of a surgeon’s management plan.
Introduction
Fine needle aspiration (FNA) biopsy is a common diagnostic tool in the evaluation of head and neck masses. FNA is generally safe and well tolerated by patients. In the work-up of parotid masses, the reliability of FNA continues to remain unclear despite numerous studies investigating its accuracy.1-4 As the implication of an inaccurate FNA result may have important consequences for patients, it is imperative to understand the diagnostic utility of this tool. In the literature, the sensitivity and specificity of FNA for differentiating between benign and malignant parotid lesions has been reported at 33%–100% and 67%–100%, respectively. 5
The variability of the diagnostic accuracy of FNA can be attributed to many factors including operator expertise, cytopathologist experience, and geographical prevalence of benign and malignant disease.1,5 Despite this, some surgeons consistently use parotid FNA results to guide their surgical management and advise their preoperative counseling. Opponents of such practice cite the low sensitivity and high false negative rate as reasons to re-evaluate the utility of FNA. 6 These surgeons may monitor parotid lesions with serial clinical exams or imaging. Other surgeons may note the anatomical location of the mass as an indication for surgery and subsequently proceed to surgery for every parotid lesion. 3 As parotidectomy is not without risks, most notably facial nerve injury, it becomes imperative to consider surgery only when absolutely necessary. Some lesions, such as Warthin tumors, may require monitoring only. Benign neoplasms, such as pleomorphic adenomas, can be managed by subtotal parotidectomy. Malignant lesions may require extensive parotidectomy. As the management paradigm of parotid masses is so broad, it is important to understand the diagnostic utility of FNA and its limitations.
Within the Canadian population, there has been no study investigating the diagnostic accuracy of ultrasound-guided FNA in the work-up of parotid lesions. In the literature, there is marked heterogeneity of study populations when assessing the diagnostic accuracy of parotid FNA. This, in combination with the highly variable reported accuracy, makes it essential to further evaluate the ability of FNA to distinguish between benign and malignant parotid disease.
Methods
Comparison of the performance of FNA and final pathology results (overall accuracy).
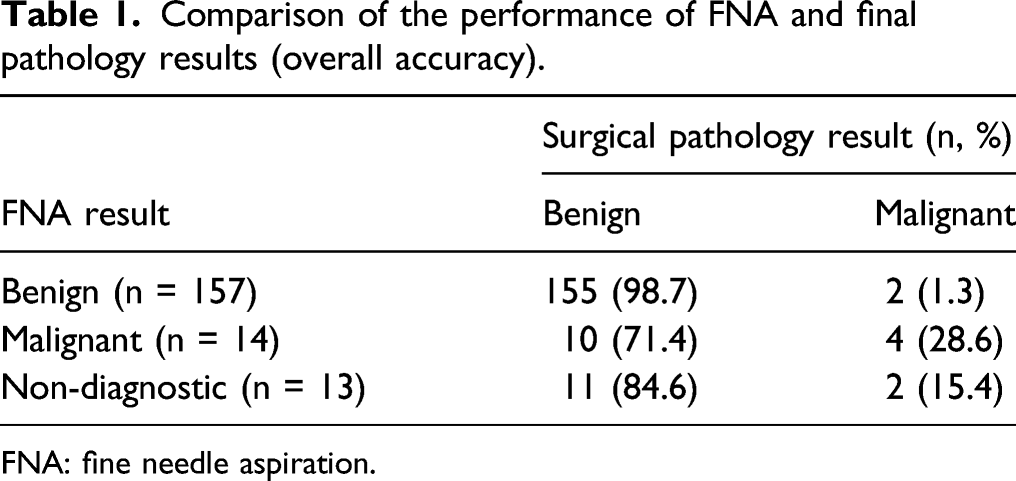
FNA: fine needle aspiration.
Only patients who had preoperative FNA were included in the study. At our institution, parotid FNAs are completed by pathologists, radiologists, general surgeons, and otolaryngologists. Standard procedure involves use of ultrasound-guided technique, although this may not always be the case. In this study, only ultrasound-guided FNA biopsies were included. Further, patients with a pre-established pathological diagnosis (from previous surgery) were excluded.
The results of preoperative FNA were compared to final postoperative pathology. The diagnostic utility of FNA was evaluated using various statistical parameters including sensitivity (ability of the test to identify a positive result), specificity (ability of the test to identify a negative result), positive predictive value (the proportion of positive FNA results that are actually found to be positive on final pathology), negative predictive value (the proportion of negative FNA results that are actually found to be negative on final pathology), and overall accuracy (the percentage of correctly classified cases).
Categorical variables were compared using Fisher’s exact test, with a P-value of <.05 being considered statistically significant. All statistical analyses were carried out using SPSS® version 26.0 (SPSS, Chicago, IL).
Results
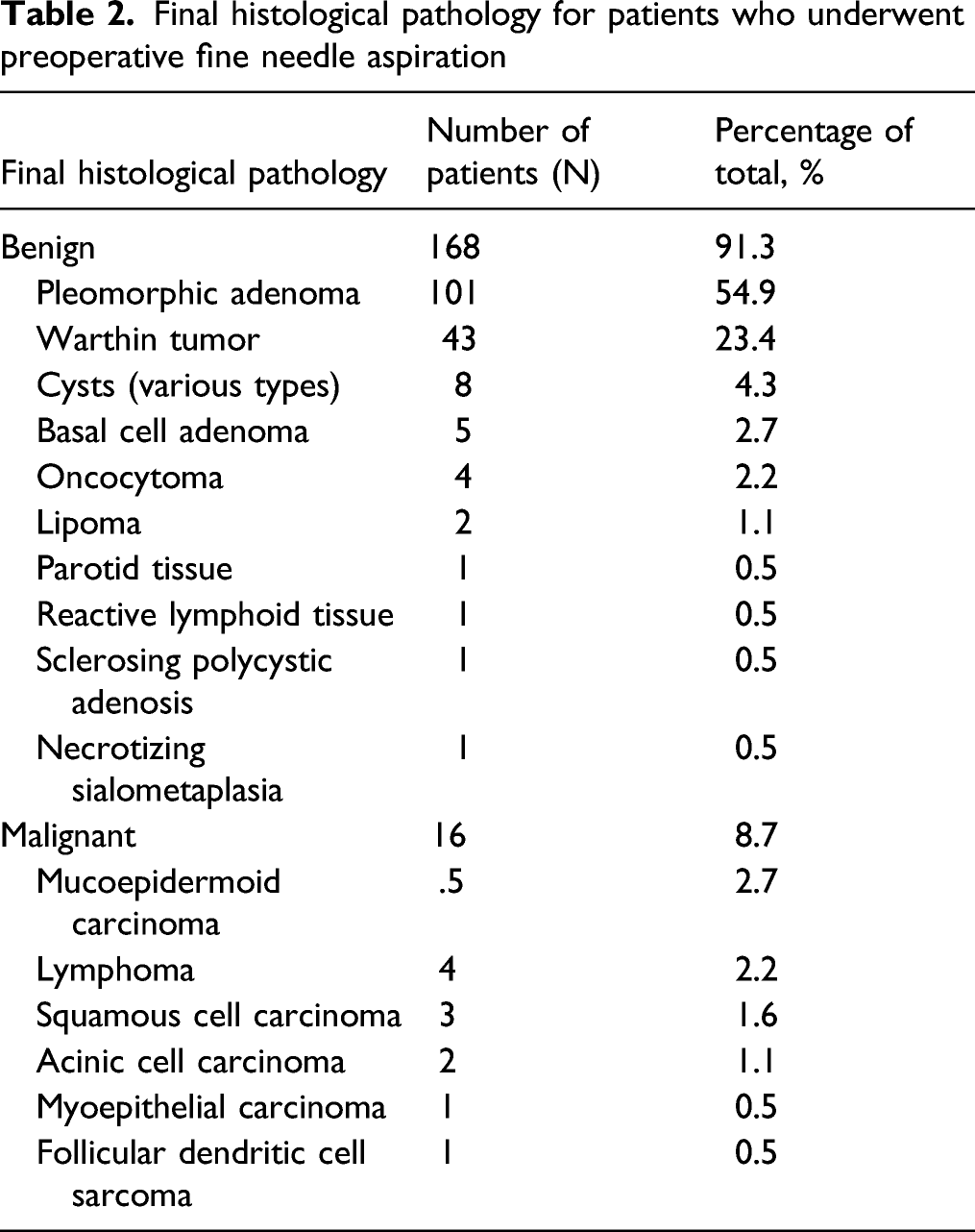
Final histological pathology for patients who underwent preoperative fine needle aspiration
Final histological pathology for patients who underwent preoperative FNA that were considered non-diagnostic.
Initial formal radiological examination completed prior to ultrasound-guided FNA.
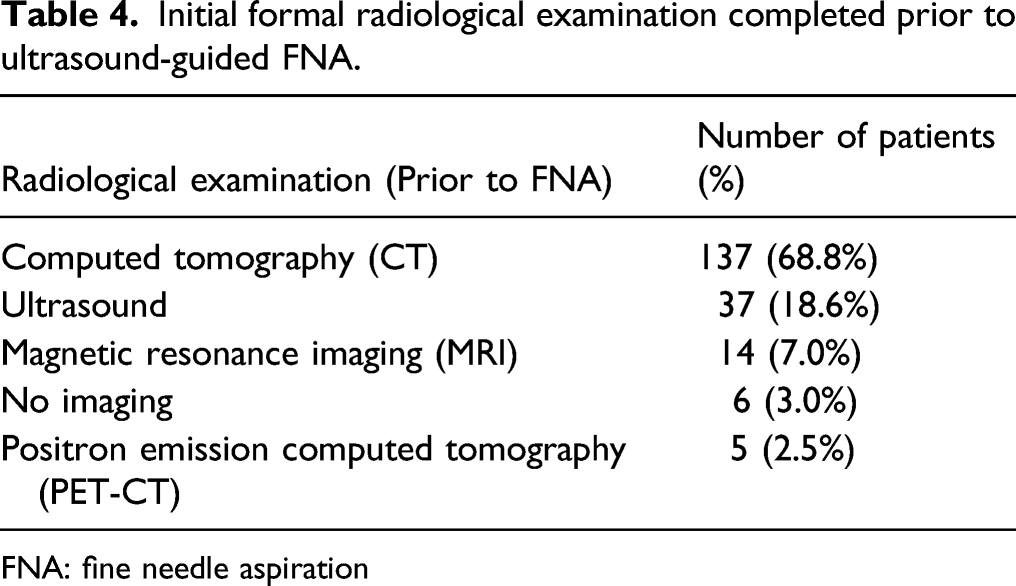
FNA: fine needle aspiration
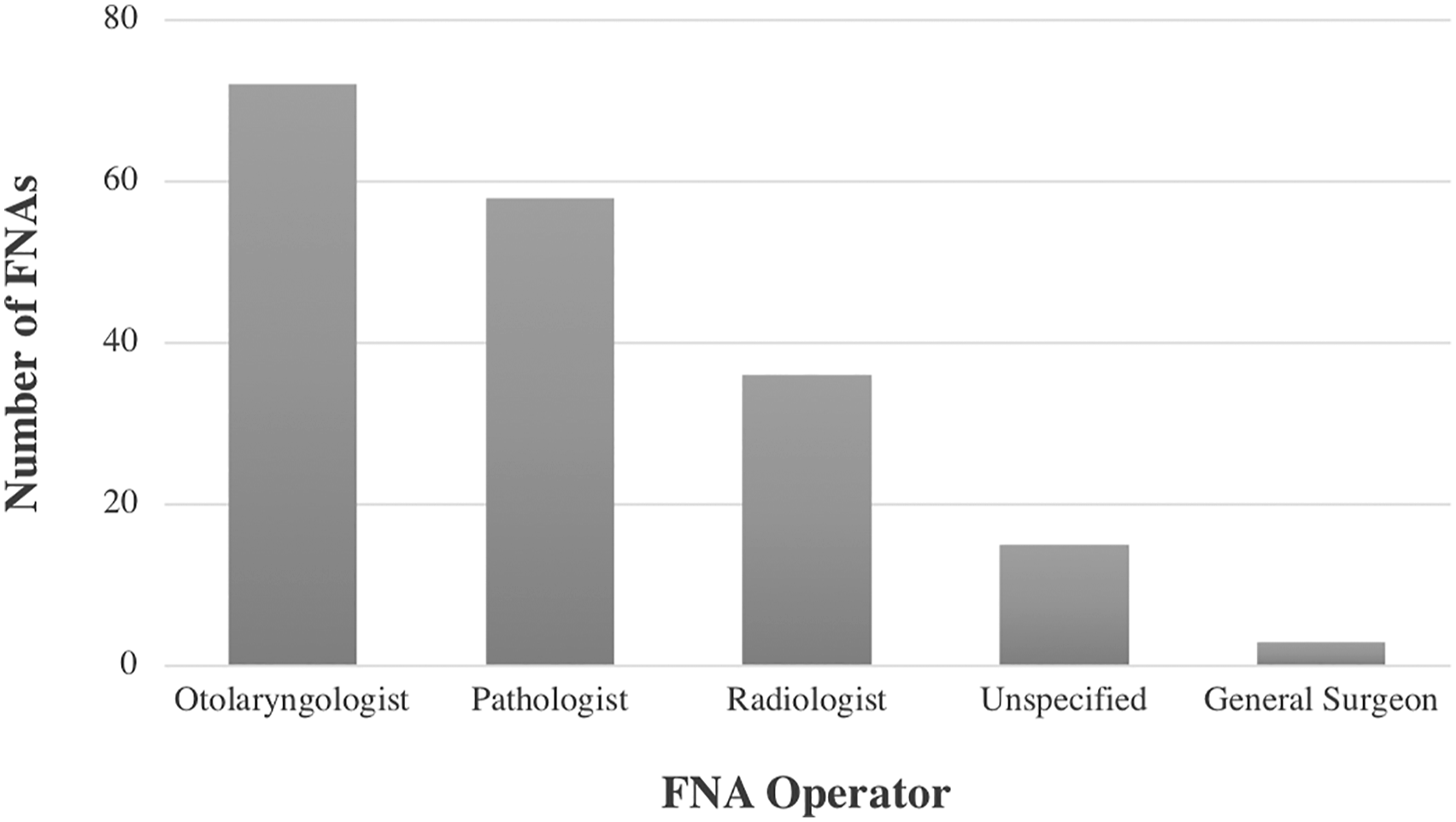
Fine needle aspiration operator by specialty.
FNA diagnostic characteristics for determining malignant disease.
FNA: fine needle aspiration
Within the study cohort (those who had preoperative FNA), neck dissection was performed in 19 patients (10.4%): 10/168 (6.0%) of benign cases and 9/16 (56.4%) of malignant cases (P = .0001).
Of all 199 patients who underwent parotidectomy, facial nerve injury was reported in 2.0% (4/199). Operative reports indicated that the nerve was knowingly sacrificed due to malignant invasion in 2 of these cases. In the other 2 cases where injury was documented, final pathology indicated benign disease (2/199).
Discussion
FNA is an important component of the diagnostic work-up of parotid masses. The results of FNA commonly inform preoperative patient counseling and surgical plan. This study sought to investigate the clinical accuracy of FNA in correctly diagnosing benign and malignant disease. Moreover, the importance of FNA in the overall work-up of parotid masses was evaluated by assessing the frequency and type of adjunct diagnostic procedures, such as formal imaging.
In this cohort, 91.3% of patients had final pathological diagnoses that were benign, which is higher than what is reported in the literature (80–85%). 2 The most common benign diagnosis was pleomorphic adenoma (54.9%), followed by Warthin tumor (23.4%). This aligns with previous studies on a global level.1-4 It is possible that the overrepresentation of benign disease in this cohort is due to the case selection at this tertiary care center. Surgery requiring more extensive craniofacial reconstruction is not typically undertaken at this site, but rather at an affiliated institution by the same set of surgeons. Of note, the pathology reports evaluated in this study did not utilize the Milan System for Reporting Salivary Gland Cytopathology (MSRSGC). 7 This system was created in order to standardize cytopathological classifications and guide clinical management. Previous studies utilizing the 7-category scheme found high inter-rater agreement between cytopathologists. 8 Moreover, the risk of malignancy attributed to each category within the Milan system may have served to inform surgeon–patient discussions and clinical decision-making.
Prior studies have described variable accuracy in FNA for detecting parotid malignancy. Reported sensitivities range from 33% to 100% and specificities range from 67% to 100%. 5 These measures of accuracy tend to improve when FNA is guided by ultrasound. 9 Unique to this study in comparison with previous literature, all FNAs were completed under ultrasound guidance. We found a sensitivity of 71.4% and a specificity of 98.7% for detecting malignancy. These findings are in line with previous studies.1-5 A high specificity indicates that a preoperative FNA result that shows malignancy is highly reliable (low rate of false positives). This is important in counseling patients on the operative management of their disease, as they may require more extensive surgery. The finding of a lower sensitivity than specificity underscores the importance of clinical judgment when FNA results indicate benign disease.
FNA often guided the selection of which patients underwent neck dissection. 56.4% of patients with malignancy underwent neck dissection, while only 6.0% of those with benign disease did. This important finding illustrates the importance that FNA results may have on surgical planning. Addition of neck dissection significantly increases the risk of morbidity to the patient due to increased anesthesia time and risk of injury to important structures in the neck. 10 These results indicate that preoperative FNA results are instrumental in informing patient selection for more extensive surgery. Moreover, it may serve to help manage patient expectations in the treatment of their disease.
The main risk of parotid surgery is injury to the facial nerve. Generally, parotidectomy is a safe procedure when completed by experienced surgeons. In our study, 2.0% of patients had intra-operative facial nerve injury. This is slightly less than what is reported in the literature, up to 6%.11,12 In 2 out of the 4 documented injuries in our study, the nerve was sacrificed due to involvement of the preoperatively determined malignant tumor (by FNA). This highlights the importance of FNA as an adjunct in intra-operative decision-making. As the risk of post-operative facial nerve paralysis is higher in malignant cases, a preoperative malignant diagnosis may serve to better prepare the patient for potentially life-altering facial nerve dysfunction.12,13
There are several important limitations to this study. As patients were evaluated from only 1 center, this may reduce the generalizability of our results. Moreover, a sample size of 199 patients may be viewed as insufficient to draw strong conclusions. The variability of FNA operator may also be seen as a limitation. In our study, otolaryngologists, radiologists, pathologists, and general surgeons were all noted to have performed ultrasound-guided FNAs. This inconsistency may not present a correct representation of true diagnostic accuracy. In future studies, it may be beneficial to perform a sub-group analysis comparing the respective accuracies of FNA operators, as each discipline has varying levels of training in the procedure. Similar to other studies, our population was composed entirely of patients who proceeded to surgery. This is a direct result of our study design. There is a large cohort of individuals who received FNA but did not undergo surgery who have been excluded from this study. Inclusion of these patients may have altered the study results when evaluating overall diagnostic accuracy. Last, this study did not take into account factors other than FNA that may have affected the surgical plan. These include clinical history, physical examination findings, or imaging. Diagnostic work-up of parotid masses is multi-modal and a management plan is often informed by many sources of information.
Conclusions
This is the first study in a Canadian population evaluating the diagnostic utility of ultrasound-guided FNA for parotid masses. Our findings suggest that FNA is a useful adjunct in the work-up of parotid masses, owing to its high specificity for diagnosing malignancy. However, due to limited sensitivity, it should not be relied upon as the sole determinant of a surgeon’s management plan.
Footnotes
Authors' contributions
AH led data acquisition and wrote the manuscript. DO made significant contributions to design of the study. VB made significant contributions to design of the study. VL made significant contributions to manuscript revision and study design. MA made significant contributions to study design. RS made significant contributions to study design. JH made significant contributions to study design. HS made significant contributions to study design. DC made significant contributions to data acquisition, study design, and manuscript revision.All authors have approved the submitted version and to have agreed both to be personally accountable for the author’s own contributions and to ensure that questions related to the accuracy or integrity of any part of the work, even ones in which the author was not personally involved, are appropriately investigated, resolved, and the resolution documented in the literature.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics approval
Ethics approval for this retrospective study was obtained from the Health Research Review Board at the University of Alberta (Pro00076247).
Availability of data and materials
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.