
Abstract
Objectives
Predicting the need for surgical treatment among patients with chronic rhinosinusitis (CRS) is challenging. The delta neutrophil index (DNI) has been proposed as a useful laboratory marker of immature granulocytes, which indicates infection or severe inflammation in several diseases. This study evaluated DNI as an early predictor of the need for surgery in patients with CRS.
Methods
A total of 117 patients diagnosed with CRS were enrolled in this retrospective and observational study. Medical records, including symptoms data, WBC count, ESR level, LUC count, Lund-Mackay scores, and DNI, were reviewed. The receiver operating characteristic (ROC) curves were analyzed to determine the optimal cut-off values for predicting surgery.
Results
Among 117 patients, 49 patients (41.9%) needed surgical intervention. The areas under the WBC, ESR, LUC, and DNI ROC curves were .571, .600, .592, and .782, respectively. The optimal cut-off value of DNI to predict surgery was .9%. The prognostic precision of DNI showed that the sensitivity was 59.2% and the specificity was 98.5%. In the analysis of risk factors, DNI levels were significantly associated with surgical intervention (odds ratio, 2.22; 95% confidence interval, 1.48-3.34; P < .01).
Conclusions
The level of DNI, which reflects the severity of the disease, may be a useful predictor for determining the need for surgical intervention in patients with CRS. This is the first literature to verify the role of DNI in upper airway disease.
Introduction
CRS is one of the leading causes of surgical intervention among otolaryngological diseases.1,2 CRS can be cured with optimal medical treatment in many cases, while surgical treatment is needed in some refractory patients to medical therapy. However, predicting the need for endoscopic sinus surgery (ESS) in patients with CRS is challenging because clinical courses would be diverse depending on the severity of the disease. To evaluate the severity of the disease, imaging modalities such as plain paranasal x-ray and computed tomography (CT) and laboratory parameters such as serum white blood cell count (WBC), erythrocyte sedimentation rate (ESR), and C-reactive protein (CRP) have been used for the diagnostic evaluation of CRS. A recent study has suggested that the Lund–Mackey (LM) score using CT provides a prognostic role in surgical treatment decisions for CRS. 3 Peripheral blood cell count and inflammation-based markers for CRS have been evaluated in several previous studies.4-6 However, even with these efforts, there are still clinical limitations of radiological tests due to limited sensitivity and specificity or low-cost performance and radiation hazard. 7 Furthermore, previously used laboratory markers could not adequately reflect the local severity of inflammation in the sinonasal area due to systemic characteristics. Therefore, it remains difficult to predict the need for surgery in patients with CRS.
Recently, the impact of neutrophils has been recovered in CRS. Succar et al 8 reported that neutrophils are a paramount, yet underrecognized marker of inflammation, disease severity, and quality of life in CRS. Morse et al 9 asserted that aging in CRS is associated with elevations in neutrophilic tissue inflammation and an increased prevalence of bacterial infection.
The delta neutrophil index (DNI) is the difference in leukocyte subfractions assessed by an automated blood cell analyzer.10,11 DNI has been proposed as a marker of immature granulocytes that indicate the presence of infection or severe inflammation.12,13 DNI has been shown to have a distinct correlation with the severity of the disease in other infectious or inflammatory diseases such as sepsis, prostatitis, pancreatitis, and pneumonia.10,13,14 Therefore, numerous studies have proposed the clinical utility of using DNI as a predictor or indicator of early diagnosis, surgical decision, and prognosis in patients with various inflammatory and infectious diseases.10,12,15 Kim et al 16 reported the usefulness of DNI in differentiating between low-grade community-acquired pneumonia, lower airway complications, and common upper respiratory infection. However, there is a lack of information on the clinical role of DNI in CRS. Therefore, given the strong association with inflammatory severity, the authors evaluated the impact of DNI as a predictor of surgical treatment in patients with CRS.
Patients and methods
Patients and treatment protocol
Among the 4712 patients with CRS diagnosed at Konyang University Hospital between 2002 and 2007, 1838 patients with CRS who underwent the DNI test were identified (Figure 1). In our department, we included ≥15-year-old and <70-year-old patients with rhinologic symptoms diagnosed with CRS. CT or other laboratory tests, and sinus endoscopy were also included to improve diagnostic accuracy. The CT score using the Lund–Mackay system was used to determine the extent of the disease as previously described.
17
Inflammatory markers, such as blood WBC count, ESR, large unstained cell count (LUC), and DNI, were analyzed as objective tests. Emergent surgery, previous sinonasal surgery, fungal sinusitis, tumor, and autoimmune diseases were excluded. Consequently, a total of 117 patients with CRS were collected for statistical analysis in the present study. The institutional review board (IRB) of Konyang University Hospital approved this study (2020-07-028). The IRB waived the need for informed consent due to the retrospective study design. A schematic chart of the patient selection process. CRS = chronic rhinosinusitis; DNI = delta neutrophil index; CT = computed tomography.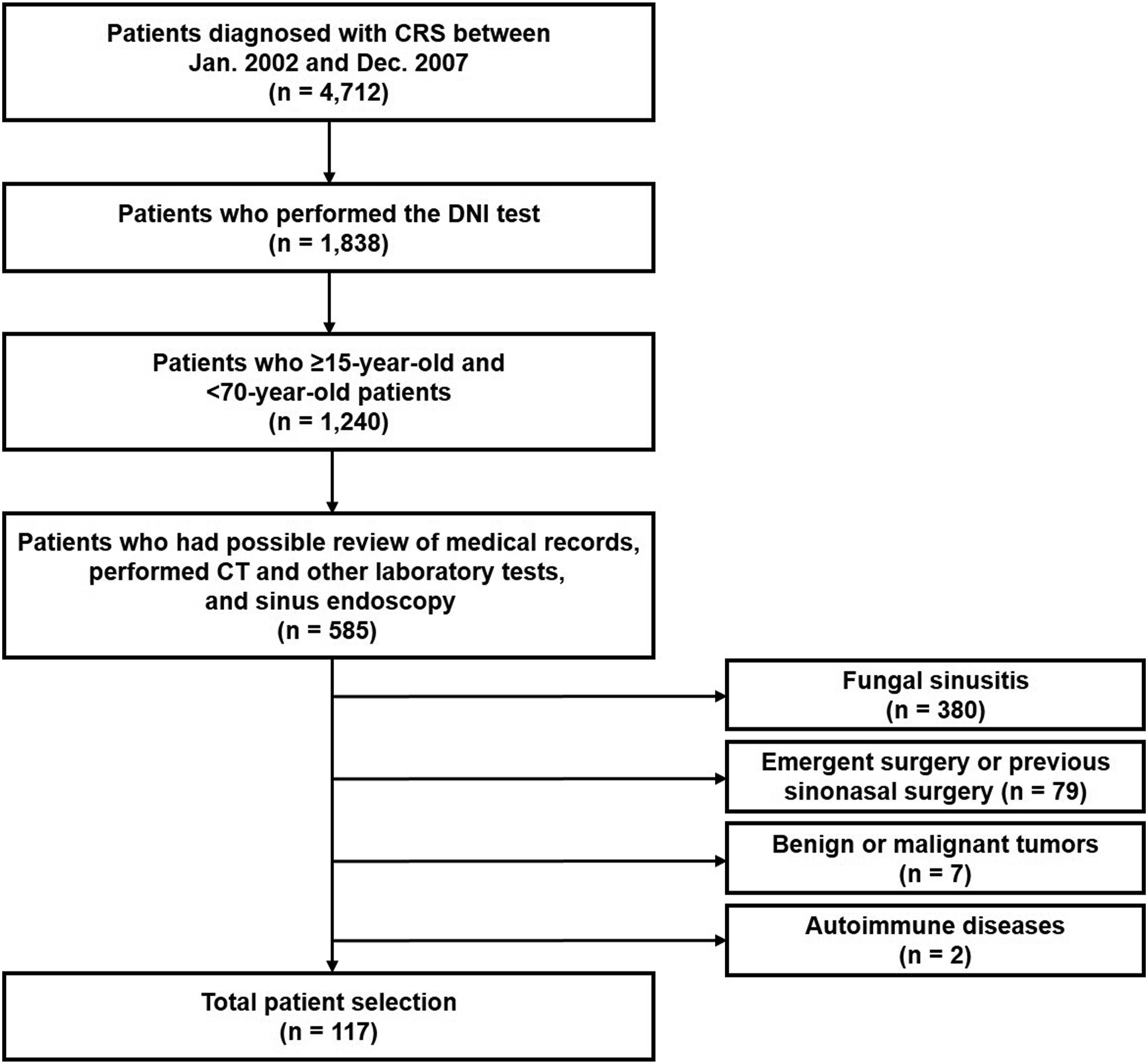
Subjective symptoms include rhinorrhea, nasal obstruction, posterior nasal drip, cough, sputum, sneezing, itching, fever, headache, facial pain, hyposmia, and epistaxis.
All patients had undergone medical treatment with oral antibiotics, topical steroid, oral steroid, and saline irrigation for 4 to 8 weeks. 18 All were treated with oral antibiotics for a minimum of 4 weeks. Amoxicillin/clavulanate (500 mg/125 mg three times daily) or clarithromycin (250 mg twice daily) was generally prescribed. All patients used topical steroid twice daily. The topical steroid brand was not standardized. Patients with nasal polyps or hyposmia symptoms were administered oral prednisolone that was tapered over 2 weeks (40 and 20 mg daily for the first and second week, respectively). Nasal saline irrigation was performed using a commercially available bulb syringe. All patients were educated on the method and posture of saline irrigations. Patients with allergic rhinitis or asthma received oral antihistamine and leukotriene inhibitors. Intravenous antibiotics, topical antibiotics, and topical antihistamines were not prescribed to patients in the present study. Despite the 8-week medical treatment protocol, the patients were defined as failure–relapse, or persistence of symptoms or signs. Therefore, they decided to undergo surgery. Detailed indications for surgery were based on close monitoring of clinical symptoms and endoscopic and radiological findings. The final decision was made by the patient’s treating surgeon based on the overall clinical status.
Delta neutrophil index
DNI is the difference between leukocyte subfractions identified by a cytochemical myeloperoxidase (MPO) reaction and a nuclear lobularity assay. It corresponds to the subfraction of immature granulocytes in peripheral blood. The DNI values were determined using a hematology analyzer (ADIVA 120 hematology system, Siemens, Inc, Erlangen, Germany). The values were calculated automatically by the hematology analyzer using the formula below.
DNI = [% neutrophils plus % eosinophils measured in the MPO reaction channel]—[% polymorphonuclear leukocytes measured by light beam in the nuclear lobularity channel].
Statistical analysis
The R software version 3.4.3. (R Foundation for Statistical Computing, Vienna, Austria) was used for statistical and graphical analyses. Differences with a P-value of <.05 were considered statistically significant. Continuous variables were analyzed using the t-test and categorical variables were analyzed using Pearson’s chi-square test or Fisher’s exact test. The prediction performance was assessed using the value R. 2
The receiver operating characteristic (ROC) curves and the area under the curve (AUC) were analyzed to evaluate the optimal DNI cut-off value of each objective variable for predicting surgery. The optimal cut-off value was determined by drawing a line connecting the points closest to the left upper corner. A subgroup analysis of each objective variable was performed according to the DNI cut-off value. The risk factor analysis for the objective parameters was performed using a multivariate logistic regression model. Finally, the optimal predictive modality using CT was investigated through a comparison between AUCs.
Results
Characteristics of the patients.
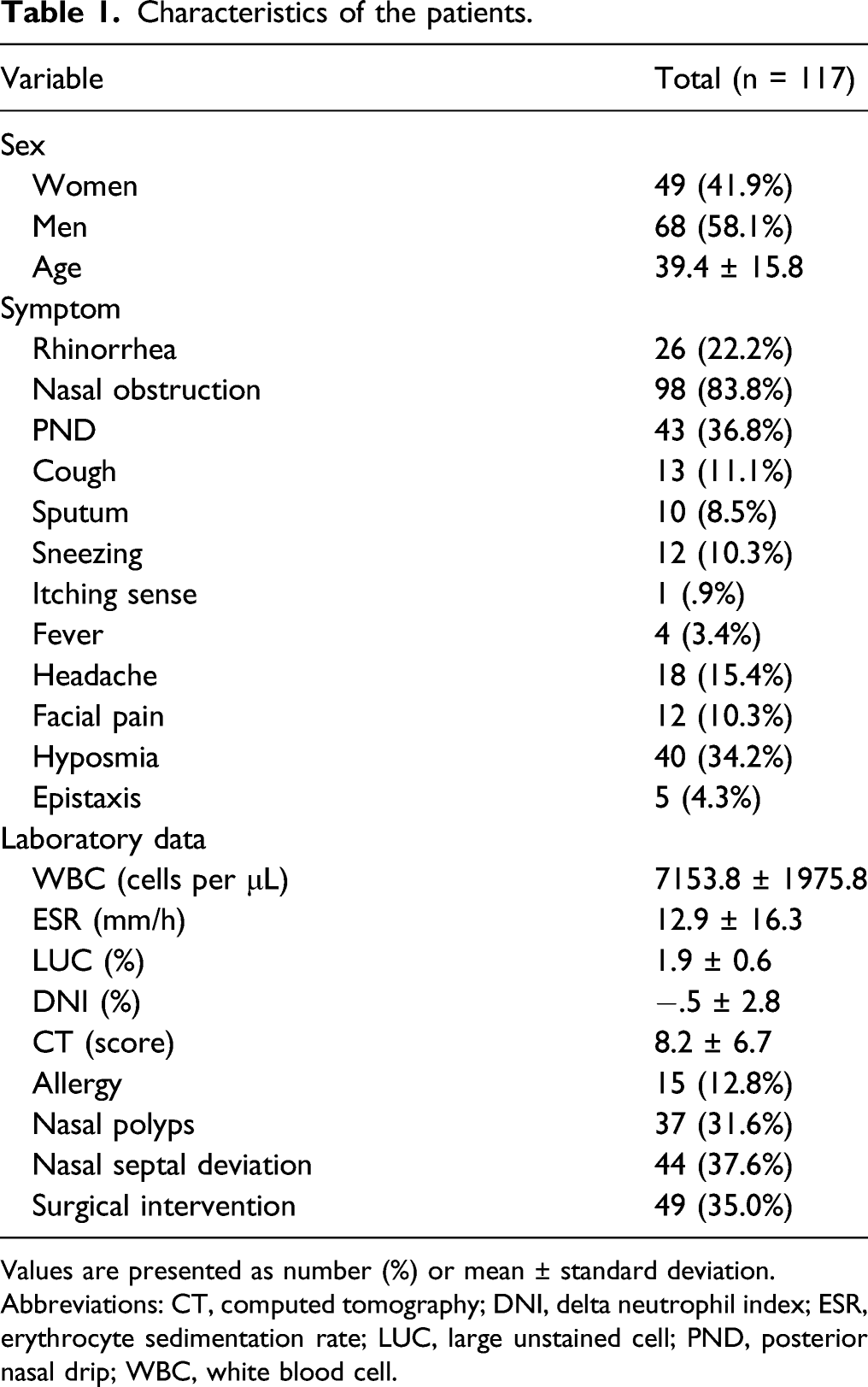
Values are presented as number (%) or mean ± standard deviation.
Abbreviations: CT, computed tomography; DNI, delta neutrophil index; ESR, erythrocyte sedimentation rate; LUC, large unstained cell; PND, posterior nasal drip; WBC, white blood cell.
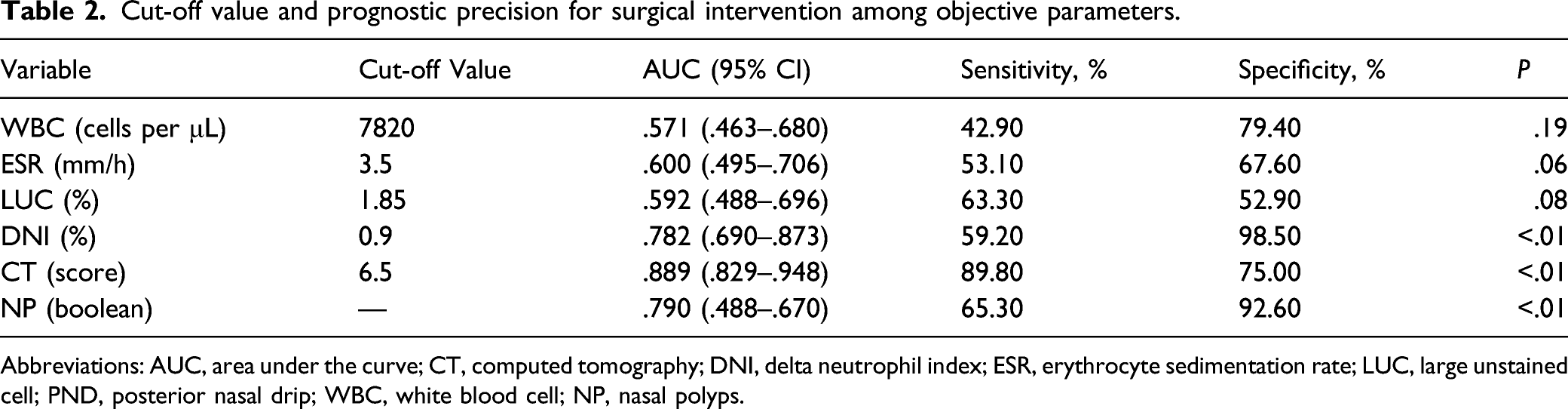
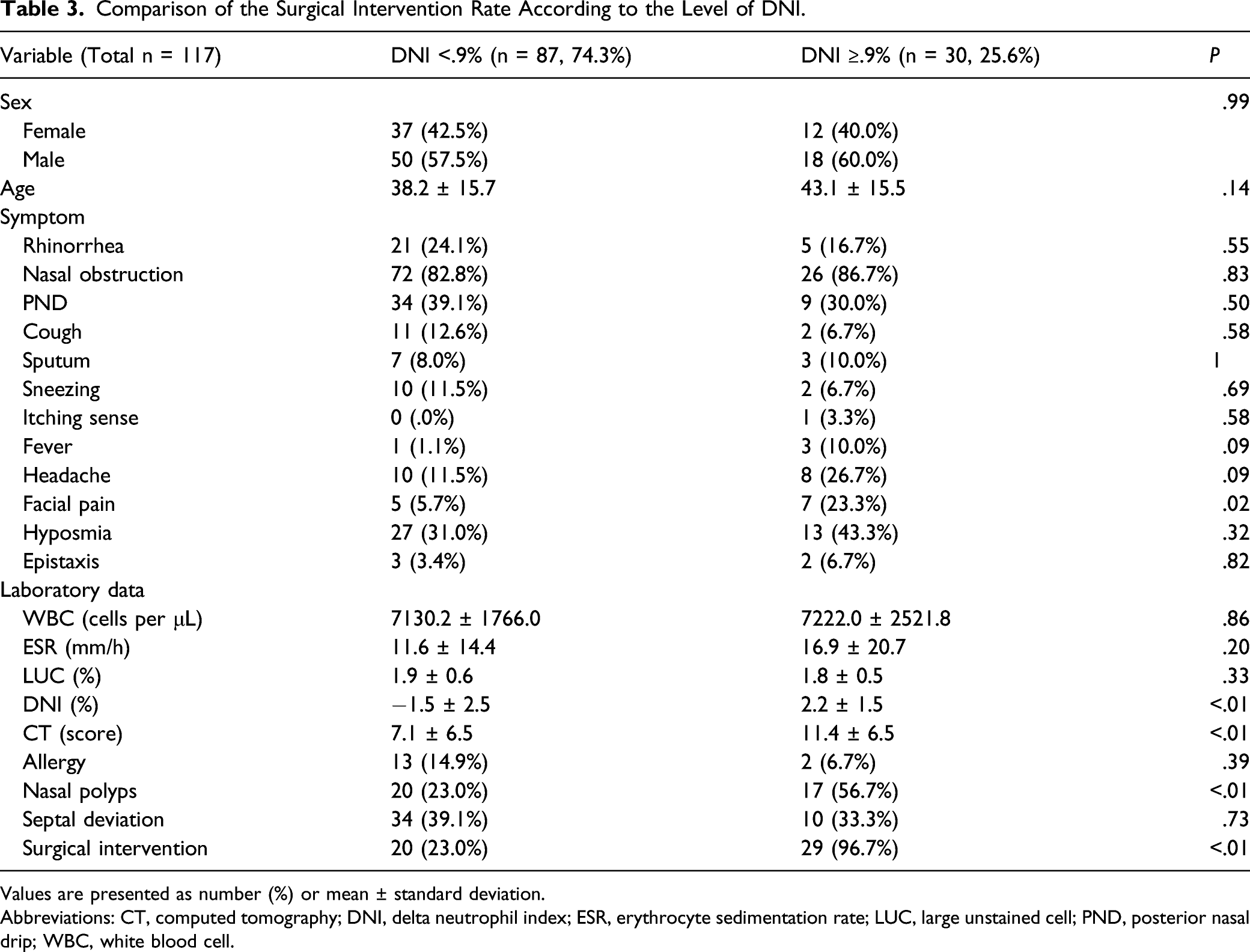
The ROC curve analyzed that the optimal cut-off value of DNI to predict surgery in patients with CRS was .9% (Figure 2). This cut-off value of DNI revealed a sensitivity of 59.2%, a specificity of 98.5% with an AUC of .78 (95% confidence interval [CI] .69-.87, P < .01) (Table 2). Additionally, the CT cut-off level was 6.5 score, with an AUC of .89 (95% CI .83-.95, sensitivity = 89.8%, specificity = 75.0%, P < .01). The prognostic precision of NP showed a sensitivity of 65.3%, a specificity of 92.6% with an AUC of .79 (95% CI .49-.67, P < .01). However, the other objective markers in the peripheral blood test, namely the WBC count, ESR, and the LUC count, did not show predictive power in the ROC curve and the AUC analysis. Based on the cut-off level, patients with DNI ≥.9% showed a higher CT score and a higher prevalence of facial pain and nasal polyps (NP) than patients with DNI <.9% (Table 3). Interestingly, future surgery was significantly different between patients with DNI ≥.9% and patients with DNI <.9%. Receiver operating characteristic curves of laboratory markers and CT score. CT = computed tomography; DNI = delta neutrophil index; NP = nasal polyps; ESR = erythrocyte sedimentation rate; LUC = large unstained cell; WBC = white blood cell. Cut-off value and prognostic precision for surgical intervention among objective parameters. Abbreviations: AUC, area under the curve; CT, computed tomography; DNI, delta neutrophil index; ESR, erythrocyte sedimentation rate; LUC, large unstained cell; PND, posterior nasal drip; WBC, white blood cell; NP, nasal polyps. Comparison of the Surgical Intervention Rate According to the Level of DNI. Values are presented as number (%) or mean ± standard deviation. Abbreviations: CT, computed tomography; DNI, delta neutrophil index; ESR, erythrocyte sedimentation rate; LUC, large unstained cell; PND, posterior nasal drip; WBC, white blood cell.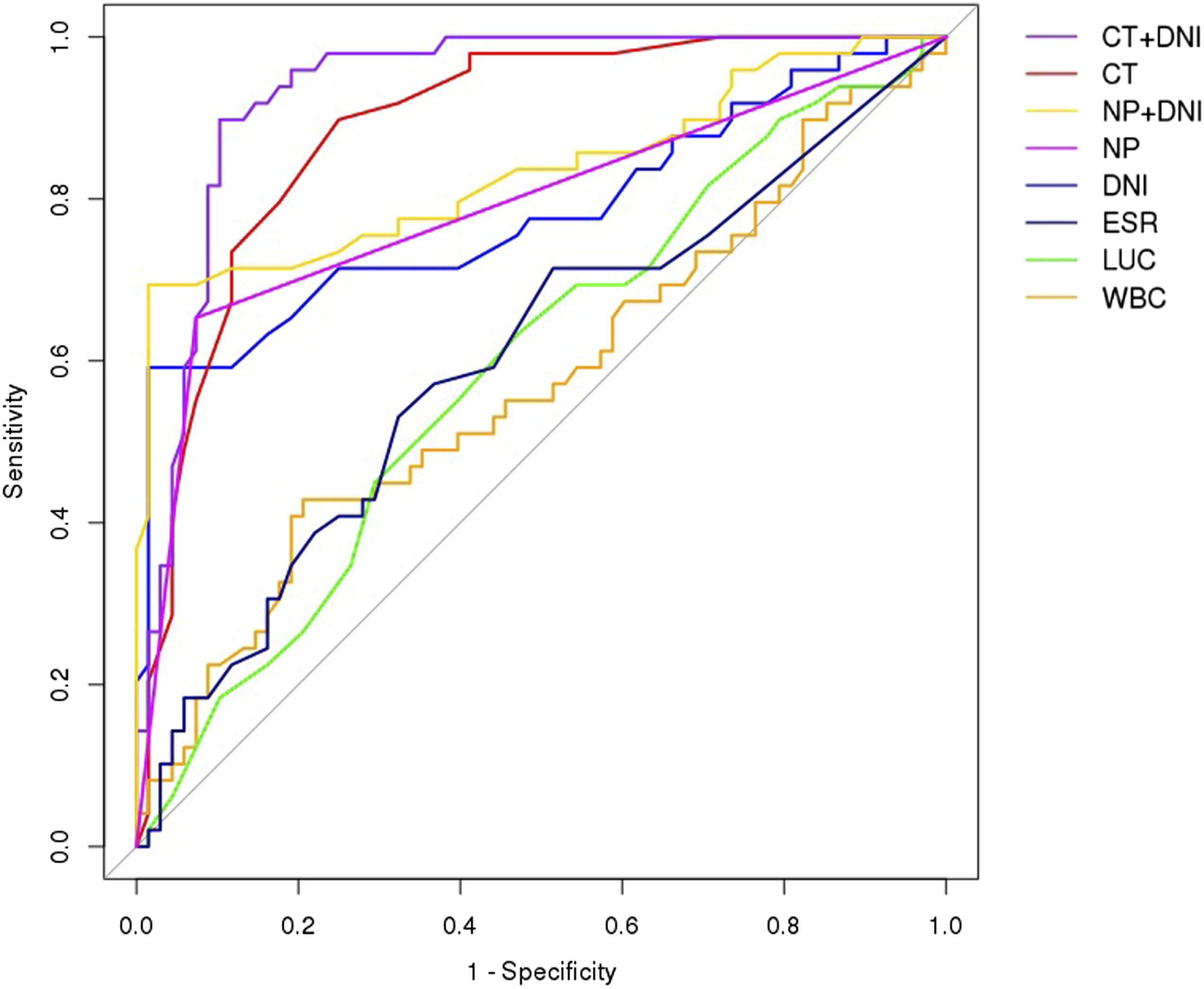
Comparison of the Surgical Intervention Rate According to the Presence or Absence of Nasal Polyps.
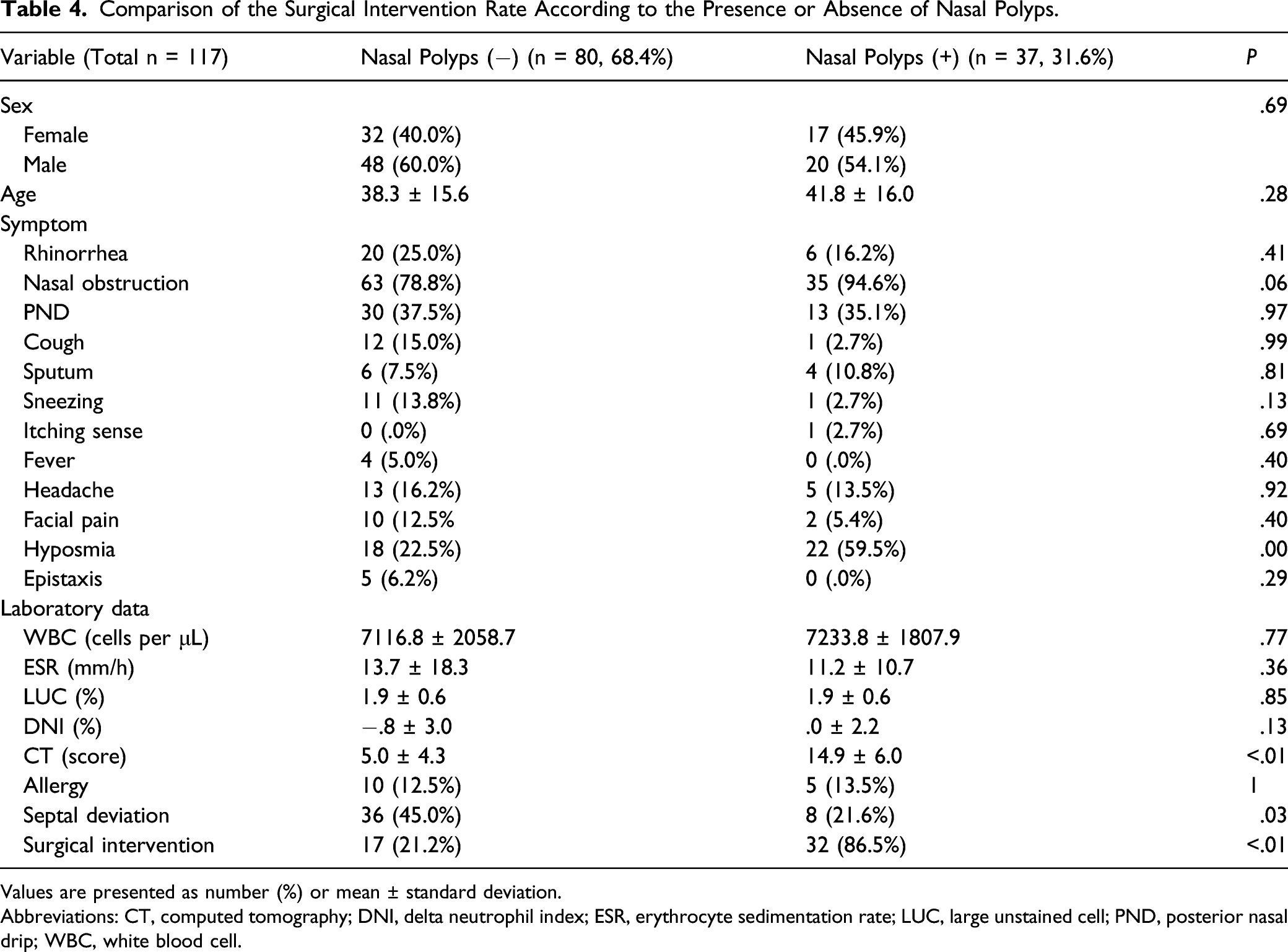
Values are presented as number (%) or mean ± standard deviation.
Abbreviations: CT, computed tomography; DNI, delta neutrophil index; ESR, erythrocyte sedimentation rate; LUC, large unstained cell; PND, posterior nasal drip; WBC, white blood cell.
Analysis of Risk Factors for Surgical Intervention among Objective Parameters.
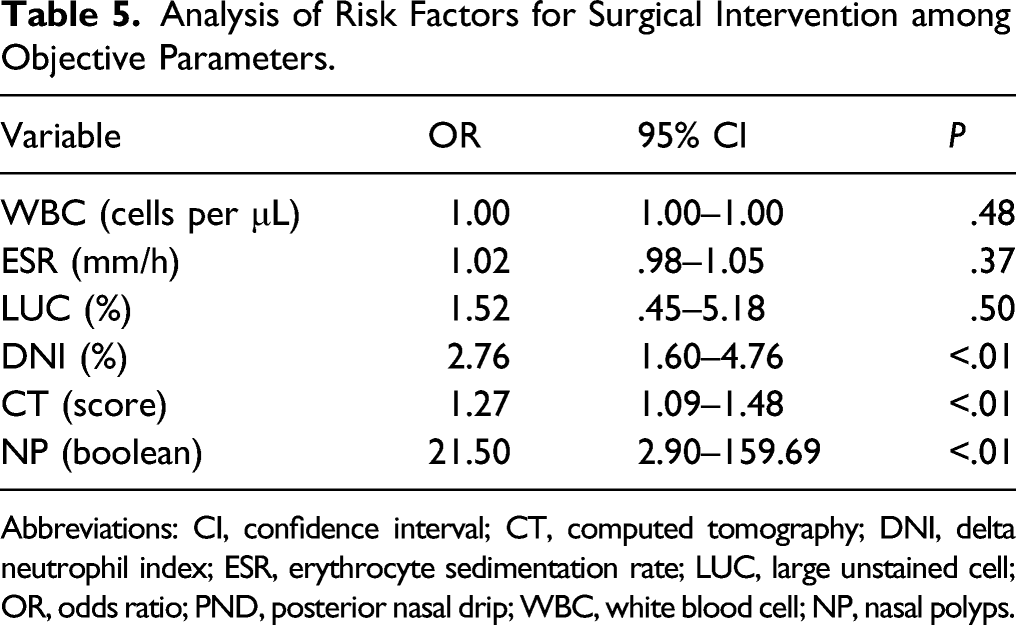
Abbreviations: CI, confidence interval; CT, computed tomography; DNI, delta neutrophil index; ESR, erythrocyte sedimentation rate; LUC, large unstained cell; OR, odds ratio; PND, posterior nasal drip; WBC, white blood cell; NP, nasal polyps.
Comparison of Combined CT Modalities, Nasal polyps, and Laboratory Marker to Predict Surgical Intervention.
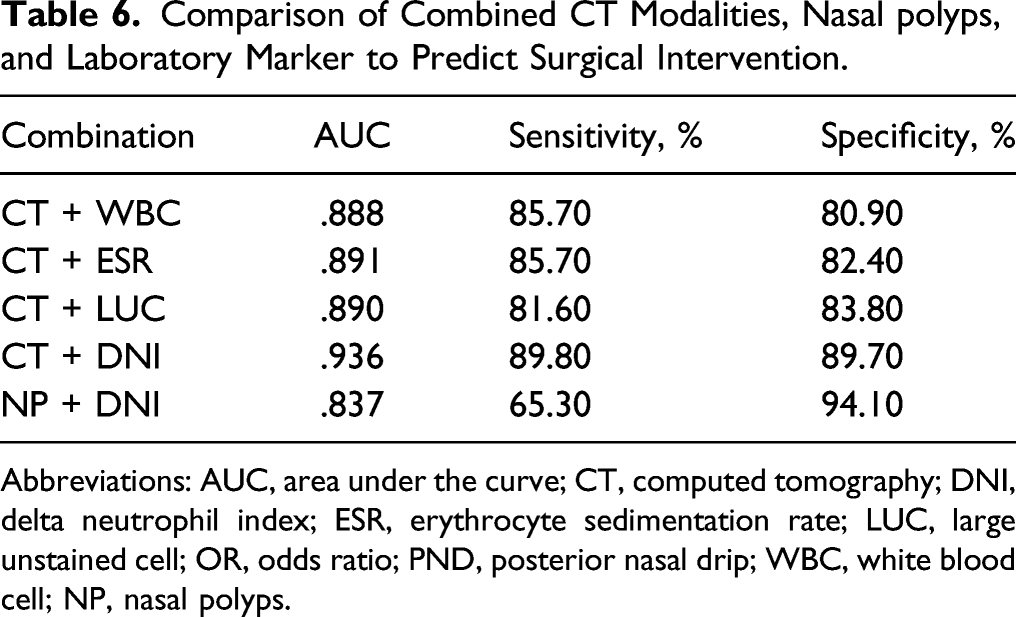
Abbreviations: AUC, area under the curve; CT, computed tomography; DNI, delta neutrophil index; ESR, erythrocyte sedimentation rate; LUC, large unstained cell; OR, odds ratio; PND, posterior nasal drip; WBC, white blood cell; NP, nasal polyps.
Discussion
We found that surgical intervention was performed more frequently among patients with DNI ≥.9% than among those with DNI <.9%. We also verified that the predictive value of DNI was higher than that of other objective inflammatory measures such as the WBC count, ESR, or LUC count. Furthermore, a combination of CT and DNI showed the highest discriminatory power to predict future surgical intervention in patients with CRS. This outcome is meaningful because CT provides a predictive role in the preoperative surgical decision and the postoperative prognosis of ESS. Singh et al 3 Reported that the cut-off value of the Lund–Mackey score, which reflects the extent of the disease, was 13.1. However, conventional CT could not be frequently evaluated due to cost and radiohazard. 7 On the other hand, DNI provides an automated count of serum immature granulocytes and has the advantages of being rapid and highly reproducible.16,19 Importantly, DNI can be obtained from routine sampling for complete blood count without additional examinations or costs. 19 We also found that a combination of NP and DNI was associated with surgical therapy and was an excellent indicator for predicting patients who need surgery. Therefore, radiological CT, endoscopic NP, and laboratory DNI could compensate for each other clinically.
Surgical treatment should be considered in refractory cases when optimal conservative treatment is unable to contain the disease. 20 Hopkins et al 21 reported that early intervention could provide symptomatic improvement and be beneficial for future health care visits and reduce the prescription of medications. A multicenter cohort study by Yip et al 22 found that the improvement of symptoms is better after a longer preoperative treatment than after a shorter preoperative treatment. A meaningless delay in surgical intervention can adversely affect long-term postoperative outcomes. 23 Thus, it is essential to determine the appropriate surgical treatment time for CRS. However, there is a lack of clarity on the right time for surgical intervention and the ability to predict the future surgical management of CRS.23-26 The authors suggest using a DNI cut-off value of .9% as an indicator of the need for surgery in clinical practice.
DNI can be used as a marker of sepsis in severe inflammatory conditions. 27 Researchers explained the scientific mechanism of DNI that there is an extensive release of cytokines during inflammation, leading to an increase in the number of immature cells. Therefore, DNI, which constitutes a simple measure of immature granulocytes in peripheral blood, could be a valuable clinical tool to evaluate systemic inflammation. In CRS, the proportion of immature granulocytes in the peripheral blood increases when CRS is aggravated in the sinonasal area in association with excessive cytokine release and polypogenesis, for which surgical treatment is needed. Therefore, DNI might be associated with NP because NP was developed by a severe inflammatory response. It should be noted that the DNI levels in our study were lower than in other diseases.11,13,15 Diagnostic criteria for DNI were reported to be higher in other systemic diseases such as intestinal obstruction (4.3%), acute prostatitis (3.5%), and Kawasaki disease (5.5%).13,15,19 This can be explained by the characteristics of CRS, which are characterized by mild manifestations and seldom progress to systemic complications such as sepsis. This is in agreement with previous studies on airway diseases (DNI values of 1.7% and 1.8% in pneumonia and the common cold, respectively).11,16 DNI values were also validated in several lower respiratory diseases such as chronic obstructive pulmonary disease, pulmonary tuberculosis, and community-acquired pneumonia.16,28,29 Meanwhile, Kang et al 12 reported that the DNI cut-off level for deciding to proceed with emergent surgery in acute diverticulitis is .7%. A combination of DNI and CT imaging could provide optimal diagnostic precision in patients with acute diverticulitis who visit the emergency department. However, there is still a lack of clarity on upper respiratory disease. The authors suggest that the .9% DNI cut-off value and a combination of DNI plus CT are the best modality, similar to the Kang study.
The systemic WBC count and the CRP are common laboratory markers that reflect an infectious status. However, these markers are not used for decision-making or as an accurate prognostic tool due to their nonspecific characteristics. Rather, they are used only to determine a prognostic trend. ESR has a known association with a late reaction in acute inflammation, which is why systemic ESR has a limited diagnostic role in CRS. Moreover, the LUC count could increase in several viral infections in a more pronounced manner than in bacterial infections.
Although the strengths mentioned above are strong, this study has several limitations. First, this study was limited by methodology, such as its retrospective design and small sample size. Second, we did not consider subclassification of CRS according to immunological endotype. DNI levels could be different between eosinophilic and non-eosinophilic CRS. Third, we did not evaluate the test timing and did not have follow-up results after surgery. Last, our study period is from 2002 to 2007 because the type of auto-analyzer has been changed and DNI is not available in our hospital.
Conclusions
The authors believe that the DNI can help to decide the surgical intervention for CRS at the right time. Furthermore, this novel laboratory marker could accentuate its prognostic power when combined with a CT score. To our knowledge, this is the first study on DNI in the field of otorhinolaryngology. The authors suggest promising and intriguing results in the limited samples. Future prospective studies with a larger number of patients are needed to clarify our current knowledge and overcome the limitations of the present study.
Footnotes
Authors note
The institutional Review Board (IRB) of Konyang University Hospital approved this study (2020-07-028). The need for informed consent was waived by the IRB due to the retrospective study design. This study was presented as an oral presentation at the Annual Meeting of the American Rhinologic Society on 10-12 September 2020.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by Research Resettlement Fund for the new faculty of Konyang University Hospital. And, this work was supported by the Konyang University Myunggok Research Fund of 2019.