
Abstract
Objective
The present study was designed to investigate whether acellular dermal matrix (ADM) grafts could prevent Frey’s syndrome (FS) and improve esthetic scores following parotidectomy.
Methods
From January 2015 to December 2019, 175 patients underwent parotidectomy. We divided the patients into two groups: the ADM group and the control group. We included in each group 30 patients according to a propensity score matched analysis.
Results
FS was subjective in 1 patient (3%) from the ADM group and 9 patients (30%) from the control group (P=0.015). Patients in the ADM group had a subjective esthetic score of 6.1
Conclusion
The present clinical study suggests that ADM grafts are effective in preventing FS and improving esthetic scores after parotidectomy.
Introduction
Approximately 80% of parotid tumors are benign tumors, and surgical removal is the primary treatment for these tumors. 1 Benign tumors are commonly located in the superficial lobe. Complete excision of benign parotid tumors with an adequate margin of normal tissue is recommended, resulting in partial superficial, superficial, or even subtotal and total parotidectomy.2,3
This parotid surgery has several adverse effects, including facial palsy, sialocele or salivary fistula, sensory deficit, Frey’s syndrome (FS), scars, and facial depression.4,5 Normally, the majority of facial palsy cases are temporary facial paresis. FS is a common complication affecting quality of life. FS, also known as gustatory sweating syndrome, is characterized by gustatory sweating and gustatory flushing. 6 The incidence of FS has been reported in many articles with variable percentages. The overall average FS is between 12.5% and 62% for the subjective method and 86%–98% when objective testing is performed with Minor’s starch-iodine test.7,8 Some patients report even having distressing symptoms. 9 Botulinum toxin A has proved effective in the treatment of FS; however, its therapeutic modalities are rarely permanent in efficacy. 10 Therefore, the trends of treatment have built a barrier between the skin and the parotid gland.8,11
Facial depression in the periauricular and retromandibular areas is almost unavoidable with the removal of the parotid gland and tumors, causing apparent asymmetry. This outcome leads to a low esthetic score, particularly in young people and benign tumor patients.12,13 Therefore, the areas must be reconstructed with other tissues.
Some previous studies have reported a variety of measures to prevent FS and facial depression in the periauricular and retromandibular areas, such as a sternocleidomastoid, superficial muscular aponeurotic system, vascularized free flap, temporoparietal fascial flap, free or vascularized dermal-fat graft.14–16 These measures have advantages and disadvantages. 11
Acellular dermal matrix (ADM) can act as a biological scaffold for re-epithelialization, neovascularization, and infiltration of fibroblasts, but it does not produce an immune response. 17 It acts as an ideal alternative for tissue augmentation and barriers to preventing FS and facial depression after parotidectomy.18,19 The purpose of the present retrospective study was to investigate the complications and esthetic effects of ADM after parotidectomy.
Methods
Our study was performed according to the Declaration of Helsinki regarding the ethics guidelines. The study protocol was approved by the Ethics Committee of the OUR Hospital, which waived written informed consent because of the retrospective nature of our study. Our ethics committee approved the waiver of informed consent for this study.
All consecutive patients undergoing partial superficial, superficial, subtotal, or total parotidectomy between January 2015 and December 2019 were included in this study. All patients underwent preoperative diagnosis by ultrasound or computed tomography (CT). Patients were excluded from the study for the following reasons: 1 postoperative pathology suggesting malignant tumors; 2 previous history of radiation therapy or surgery to the head and neck region; and 3 incomplete medical records or follow-up. We collected all types of data, including sex, age, type of tumor, type of parotidectomy, tumor size, specimen volume, diabetes mellitus, hypertension. Postoperative complications, drainage, and esthetic score outcomes were analyzed. All of the patients were followed up for at least 6 months.
Parotidectomy was performed in the standard manner (Figures 1(A),(B)). All of the parotid operations were performed by 1 of 2 experienced chief physicians. The marginal mandible of the facial nerve was first identified, and then a retrograde dissection of the nerve was performed. The ADM used in our study was J1-ADM (Beijing Jayyalife Biological Technology Co. Ltd, Beijing, China). The ADM size was selected according to the actual needs of the operation. All of the patients were placed on prophylactic antibiotics for the duration that their drain was in place. A: Partial resection of superficial lobe and tumor. B: Acellular dermal matrix implantation.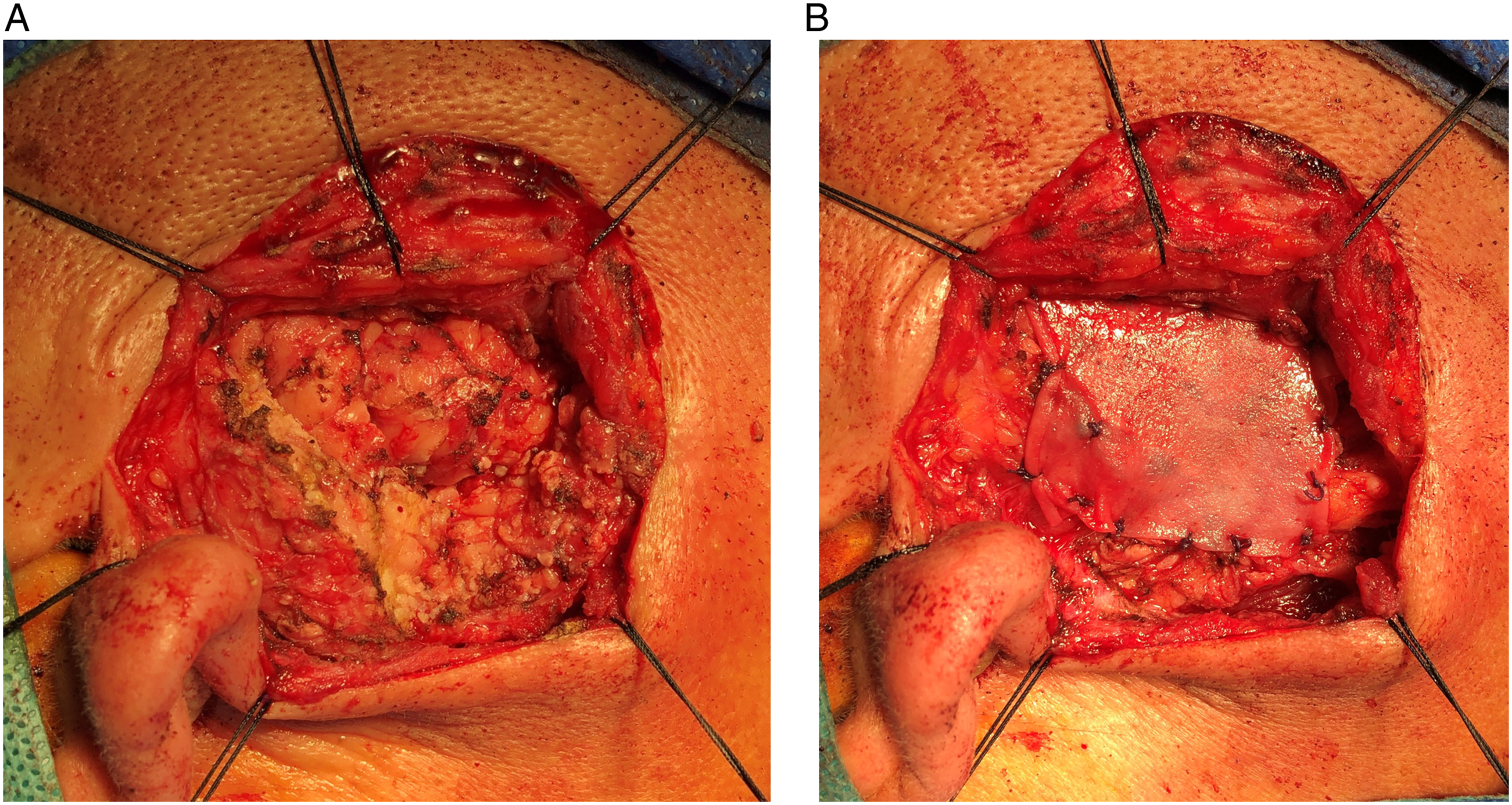
Frey’s syndrome (FS) and esthetic score were evaluated by subjective methods. For the subjective FS evaluation, patients were queried about warming, flushing, or sweating over the preauricular regions during the follow-up period. The subjective esthetic score was achieved by asking patients to complete a questionnaire designed to assess their satisfaction with the resulting scarring and upper cervical and retromandibular contour. The subjective esthetic score ranged from 1 to 10 (1 representing very dissatisfied; 10 representing very satisfied). 20
The mean and variance were used as continuous variables, and n (%) was used for categorical variables. The t test was used for continuous variables, and Pearson’s chi-square test or Fisher’s exact test was used for categorical variables. P < 0.05 was considered statistically significant. Statistical analysis was performed using SPSS software, version 22.0 for Windows.
Results
Patient profiles
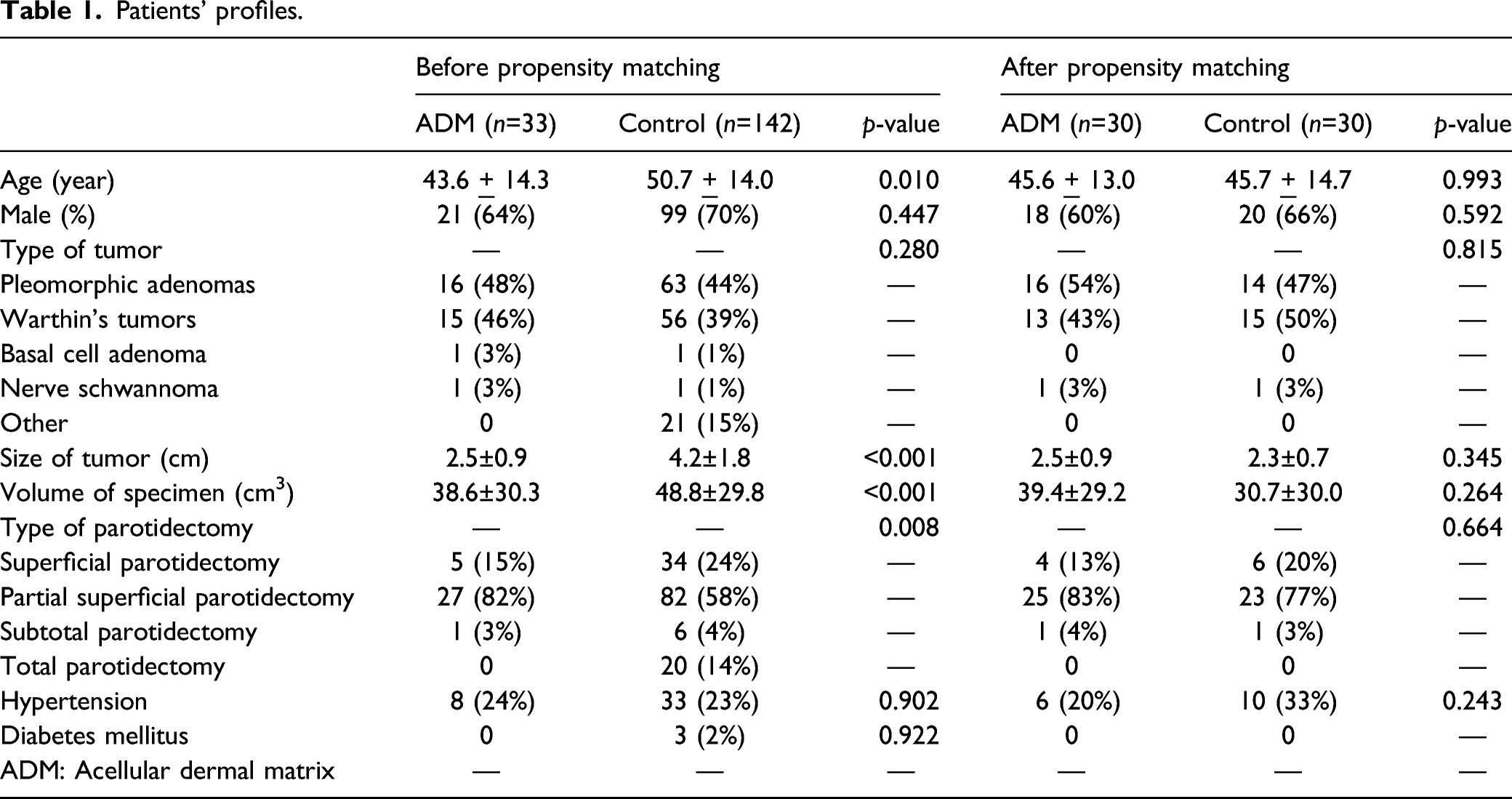
Patients’ profiles.
Complications
Complication rate in each group.
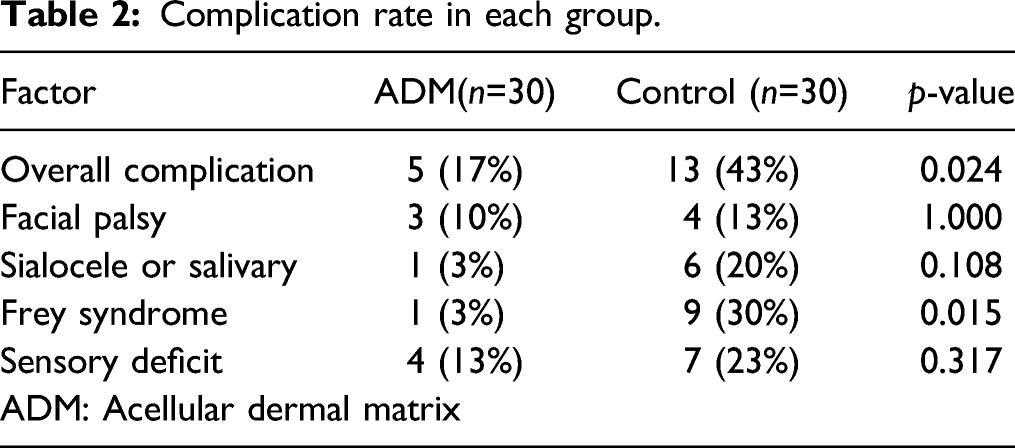
Postoperative facial function was graded on the House-Brackmann scale in all patients. Three patients (10%) in the ADM group and four patients (13%) in the control group had facial palsy, which was initially found on the first day after the operation. Postoperative facial palsy did not show statistical significance between the two groups. All of the patients except for two nerve schwannoma patients fully regained normal facial function within 6 months. The two nerve schwannoma patients in either group developed grade IV permanent facial palsy.
One patient (3%) in the ADM group and six patients (20%) in the control group developed a sialocele or salivary fistula. No significant difference was found between the two groups (P=0.108).
One (3%) patient in the ADM group and 9 (30%) patients in the control group experienced sweating over the preauricular regions 6 months after the operation. There was a statistically significant difference between the two groups in subjective Frey syndrome (FS) (P=0.015).
The most common complication was sensory deficit in both groups. Numbness in the infraauricular region occurred in four patients (13%) in the ADM group and in 7 patients (23%) in the control group (P=0.317). Nine of the 11 patients with sensory deficits recovered sensation within 6 months after the operation.
None of the patients in the ADM group experienced complications at the donor site. No patient in either group had tumor recurrence or seromas during the follow-up period.
Postoperative drainage
The postoperative drainage volume in the ADM group was 59.7 ± 26.0 mL, whereas the postoperative drainage volume in the control group was 110.0 ± 78.7 mL. Postoperative drainage was significantly decreased in the ADM group compared with the control group (Figure 2(A)) (P=0.002). The postoperative drainage time in the ADM group was 3.6 ± 0.8 days, whereas the postoperative drainage time in the control group was 4.7 ± 1.7 days. The postoperative drainage time was significantly shorter in the ADM group than in the control group (Figure 2(B)) (P=0.001). A: Comparison of postoperative drainage between the two groups. B: Comparison of postoperative drainage time between the two groups.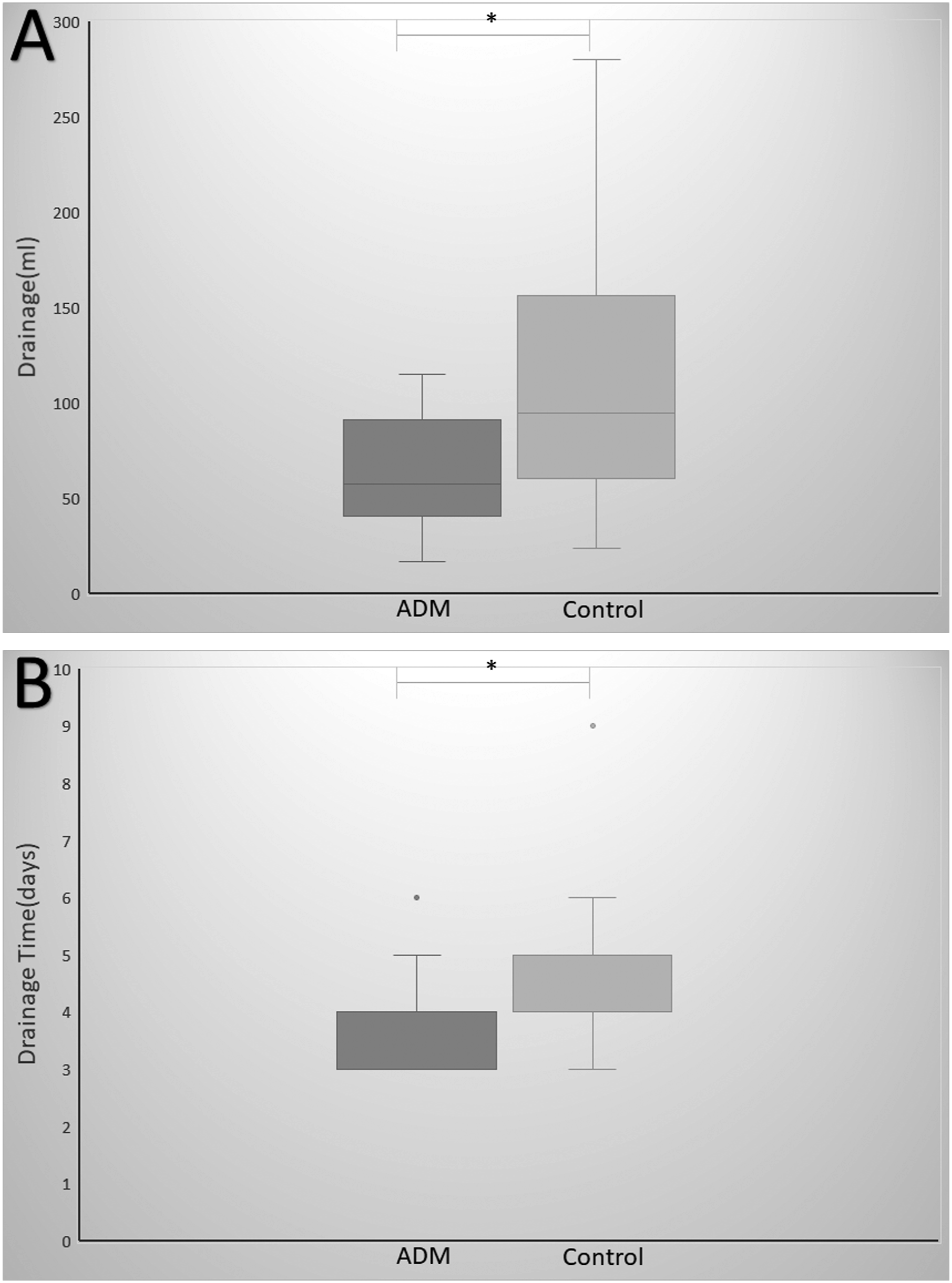
Except for sialocele or salivary fistula patients, the postoperative drainage volume in the ADM group (29 patients) was 58.3 ± 25.3 mL, whereas the postoperative drainage volume in the control group (24 patients) was 95.3 ± 72.6 mL. Postoperative drainage was also significantly decreased in the ADM group compared with the control group (P=0.013). The postoperative drainage time in the ADM group was 3.6 ± 0.8 days, whereas the postoperative drainage time in the control group was 4.5 ± 1.6 days. The postoperative drainage time was also significantly shorter in the ADM group than in the control group (P=0.010).
Subjective esthetic score
Patients in the ADM group had a subjective esthetic score of 6.1 Comparison of esthetic scores between the two groups.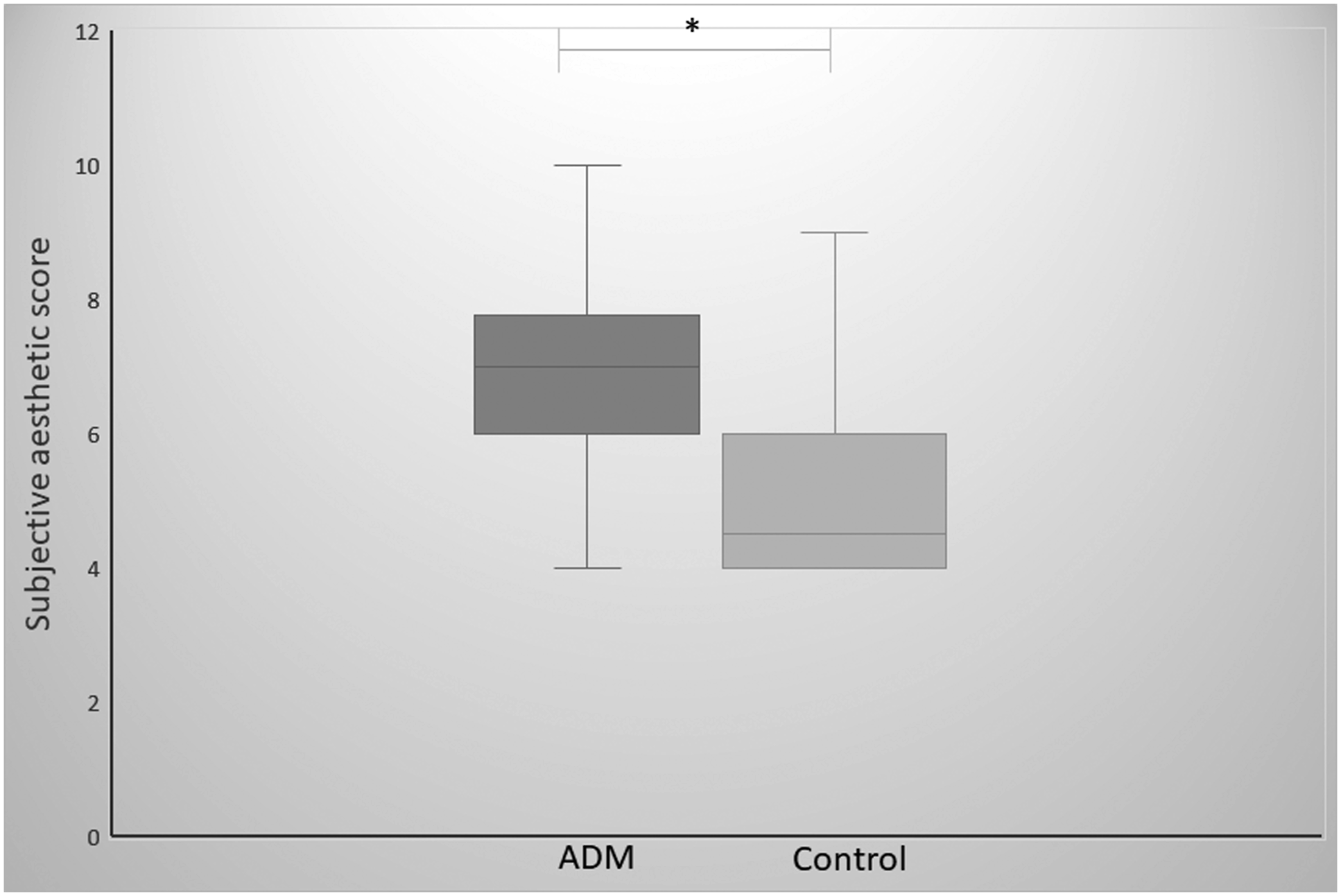
Discussion
Facial nerve preservation is the most important problem in parotidectomy for benign tumors. However, quality of life after parotidectomy should not also be ignored. FS and facial esthetics have the potential to profoundly impact quality of life after parotidectomy. Therefore, the purpose of this study was to evaluate complications, including FS, and the esthetic effects of ADM insertion after parotidectomy with propensity score matching analysis.
One of the mechanisms of FS is caused by aberrant regeneration between the postganglionic parasympathetic nerve fibers that innervate secretion of the parotid glands and the sympathetic nerve fibers that control the subcutaneous sweat glands and vessels after parotidectomy. 21 The overall incidence of FS following parotidectomy has been reported to be greatly different. Most previously reported subjective incidences of FS were between 10% and 40%, and the objective incidences were as high as 90%. 22 One reason for this difference could be the inability to estimate the clinical symptoms of gustatory sweating and gustatory flushing. The other reason could be the different research methods. A study reported that the incidence of FS in a prospective group was higher than that in a retrospective group. The differences could clarify that the prospective group was more aware of the possible incidence of FS and that symptoms of FS might disappear with time in the retrospective group.
A variety of treatments have been reported over time with advantages and disadvantages. Botulinum toxin type A has become the first-line therapy. However, the duration of effect can be short, from 12.1 months to 17.3 months 23 Scholars have also reported that building a barrier in the surgical site after parotidectomy can help to prevent FS, including the sternocleidomastoid muscle flap, the temporoparietal fascia flap, the superficial musculoaponeurotic system flap (SMAS), the free or vascularized dermal fat graft, and ADM.
The SMAS layer is the superficial cervicofacial fascia. The SMAS flap is placed between the skin and the surgical site of the parotid region. The SMAS flap can effectively prevent the occurrence of FS following parotidectomy for benign tumors. 24 The use of SMAS flaps is limited in malignant tumors or obese patients, and its resection is sometimes insufficient to cover the surgical site. Another limitation of the SMAS flap could be more injury to the marginal mandibular branch or cervical branch of the facial nerve.
The free fat graft is also a common barrier after parotidectomy. A study reported that ADM and free fat grafts were equally effective in preventing FS and other complications, including facial palsy, sialocele or salivary fistulas, and sensory deficit. 25 Nosan et al. 26 used free abdominal dermal-fat grafts to preserve the periauricular depression of 9 patients undergoing parotidectomy, and the results showed that the esthetic scores improved without significant complications. However, the shortcoming of grafts might include the need for a second surgical site with potential wound infection. Another shortcoming is the potentially unpredictable reabsorption rate without continuous efficiency. Some previously reported reabsorption rates were high, varying from 20% to 90%. 11
In recent years, ADM has been used in plastic surgery and parotidectomy. Hartzell et al. 27 reported that ADM had a satisfactory effect and was a safe material for breast augmentation. In 2007, Chen et al. 28 reported that ADM provided a satisfactory esthetic result with a low incidence of FS in parotid hemangiomas. Govindaraj et al. 7 reported the use of ADM in the prevention of FS compared with a control group for superficial parotidectomy. Sixty-four patients were randomly and equally assigned to two groups. The results demonstrated that the subjective incidences of FS were 9.3% in the control group and 3.1% in the ADM group. The objective incidence of FS was 40% in the control group and 0% in the ADM group. However, the complication rate of 25% in the ADM group was higher than 9% in the control group. In 2008, Wei et al. 29 reported a similar conclusion regarding the incidence of FS after superficial and partial superficial parotidectomy. The subjective and objective incidences of FS were recorded as 61% and 23% of the control group and 2% and 2% of the ADM group, respectively. Furthermore, the complication rate of sialocele or salivary fistula of 17% in the control group was higher than 2% in the ADM group. Luo et al. 19 reported that the subjective incidence of FS in the ADM group was 1 patient (3.4%), which was lower than the 14 patients (34.1%) in the control group for total parotidectomy. No complications were observed in either group.
In our study, the subjective incidence of FS in the ADM group was 1 patient (3%), which was lower than the 9 patients (30%) in the control group (P=0.015). The overall complication rate of 5 (17%) in the ADM group was lower than that of 13 (43%) in the control group (P=0.024). The incidence of FS for both groups in our study resembled that in the previous literature.7,19,28,29 The complication results were analogous to the conclusion of Wei et al. 29 but different from the conclusions of Govindaraj et al. 7 The reason for the difference might be partly because the research methods were different. Although our study used a retrospective design, similar to the previous literature, we matched the baseline data according to a propensity score matched analysis. We matched some important data, including age, sex, type of tumor, size of tumor, volume of specimen, type of parotidectomy, hypertension and diabetes mellitus, which might have reduced the bias of the data and increased the persuasiveness of the conclusions.
In our study, the complications of facial palsy and sensory deficit were not statistically significant. The incidence is related to the surgical technique, tumor size and location, individual feeling, etc. The incidence rate of sialocele or salivation [1 (3%)] in the ADM group was lower than that [6 (20%)] in the control group (P=0.108). However, postoperative drainage and time were significantly decreased or lower in the ADM group than in the control group (Fig. 2A and 2B). In the present study, although the incidence rate of sialocele or salivary drainage was not statistically significant, ADM patients experienced a lower rate of postoperative drainage and less time than the control group. This difference in sialocele or salivary drainage and postoperative drainage is thought to be related to the use of the ADM barrier. Some previous studies have shown similar conclusions. Ye et al. 29 reported that one salivary fistula was noted in the ADM group, while 18 cases developed in the control group (P = 0.002). We consider that the ADM should completely cover the exposed parotid and facial nerve surface. ADM grafts could replace fascia to reduce secretion and promptly eliminate the dead space. When the postoperative drainage tube was less than 10 mL, it was removed, and a proper pressure dressing was used for approximately 3–5 days. Therefore, the ADM graft could promote quality of life after parotidectomy.
The esthetic score after parotidectomy should also be an important consideration. In our study, the subjective esthetic score for patients in the ADM group was higher than that for patients in the control group (P =0.040). In 2012, a study reported that the use of ADM could reduce postoperative facial contour deformities following total parotidectomy. 19 Ciuman et al. 30 also reported that the extent of parotidectomy was related to the esthetic score. In 2019, Kim et al. 9 showed that insertion of ADM after parotidectomy, including partial, superficial, and total parotidectomy, could improve the esthetic score. The results also demonstrated that the esthetic score was related to sex and complications. Interestingly, the results showed that women were more satisfied than men. We consider that the subjective esthetic score might not have been different in either group before the study. Our research results indicated that the subjective esthetic score was manifold. We hypothesize that this factor is related to age, sex, incision, tumor size, sample volume, complications, individual feelings, etc. Further study is needed.
Our study was limited by the small sample size and relatively short follow-up time. The FS and esthetic score were evaluated by subjective methods without objective assessments because the FS and esthetic score are higher related to the subjective evaluation than the objective evaluation. Therefore, even if the starch iodine test is positive or the esthetic score is low, if a patient suffers no symptoms or is satisfied, then no intervention is required.
In conclusion, the present clinical study suggests that ADM grafts are effective in preventing FS and improving esthetic scores after parotidectomy. More RCTs are needed to confirm.
Footnotes
Acknowledgments
Thank Dr Xu Jian-Hui (The Department of Otolaryngology in the Zhongshan City People’s Hospital, Zhongshan Affiliated Hospital of Sun Yat–sen University) for reviewing the paper.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
Our study was approved by the Ethics Committee of the Zhongshan City People’s Hospital, Zhongshan Affiliated Hospital of Sun Yat-sen University (approval No. 2020075). Our ethics committee (the Ethics Committee of the Zhongshan City People’s Hospital, Zhongshan Affiliated Hospital of Sun Yat-sen University) approved the waiver of informed consent for this study.