
Abstract
Primary ectopic meningioma of the middle ear is relatively rare in clinical practice. It is often difficult to distinguish it from chronic otitis media or otitis media with effusion due to its similar and atypical clinical symptoms. We report a case of epithelial tympanic ectopic meningioma with the main complaints of otalgia, aural fullness, and hearing loss. It was accidentally discovered during tympanotomy due to the symptoms of recurring refractory secretory otitis media. This article briefly reviews the relevant literature in recent years, summarizes the characteristics of primary ectopic tympanic meningioma with intact tympanic membrane, and emphasizes the diagnosis and treatment strategy of the middle ear mass.
Introduction
Meningioma is a common benign intracranial tumor originating from arachnoid cap cells, accounting for 13–26% of all primary intracranial tumors. 1 Meningioma that occurs outside the central nervous system is defined as primary ectopic meningioma. 2 Ectopic meningiomas often occur near the sensory organs of the head and neck, such as the orbit, skull, paranasal sinuses, nasopharynx, or along the nerve distribution and next to the spine, and are rarely seen in the lungs and elbow joints. 3 Ectopic meningiomas originating in the temporal bone are rare, accounting for only 1% of all meningiomas. In the 1970s, scholars 4 reviewed the preoperative ectopic meningioma that was considered limited to the tympanic cavity. Postoperative imaging examination found that all patients had adjacent large intracranial meningiomas. With the application and progress of computed tomography (CT) and magnetic resonance imaging (MRI), intracranial and extracranial communicating temporal meningiomas are easy to diagnose before the operation. However, primary meningiomas confined to the temporal bone and even the tympanum are often difficult to identify due to the lack of specific imaging findings, and most of them are found in postoperative pathology. Due to the complex anatomical structure of the mastoid process of the middle ear, tumors generally grow slowly. Early symptoms can vary from hearing loss, aural fullness to headache, otalgia, tinnitus, vertigo, facial nerve paralysis, and bleeding. 5 However, because of the low incidence rate and lack of clinical attention and nonspecific symptoms, it is easy to misdiagnose as inflammatory diseases and other tympanal tumors such as tympanic body tumor. Despite the presence of symptoms, most patients remain undiagnosed for a long period of time, with an average duration ranging from 2 to 10 years. Therefore, this article aims to review the previous primary meningioma of the middle ear with an intact tympanic membrane and to try to clarify the clinical and radiological characteristics that distinguish it from other diseases of the middle ear.
Case Report
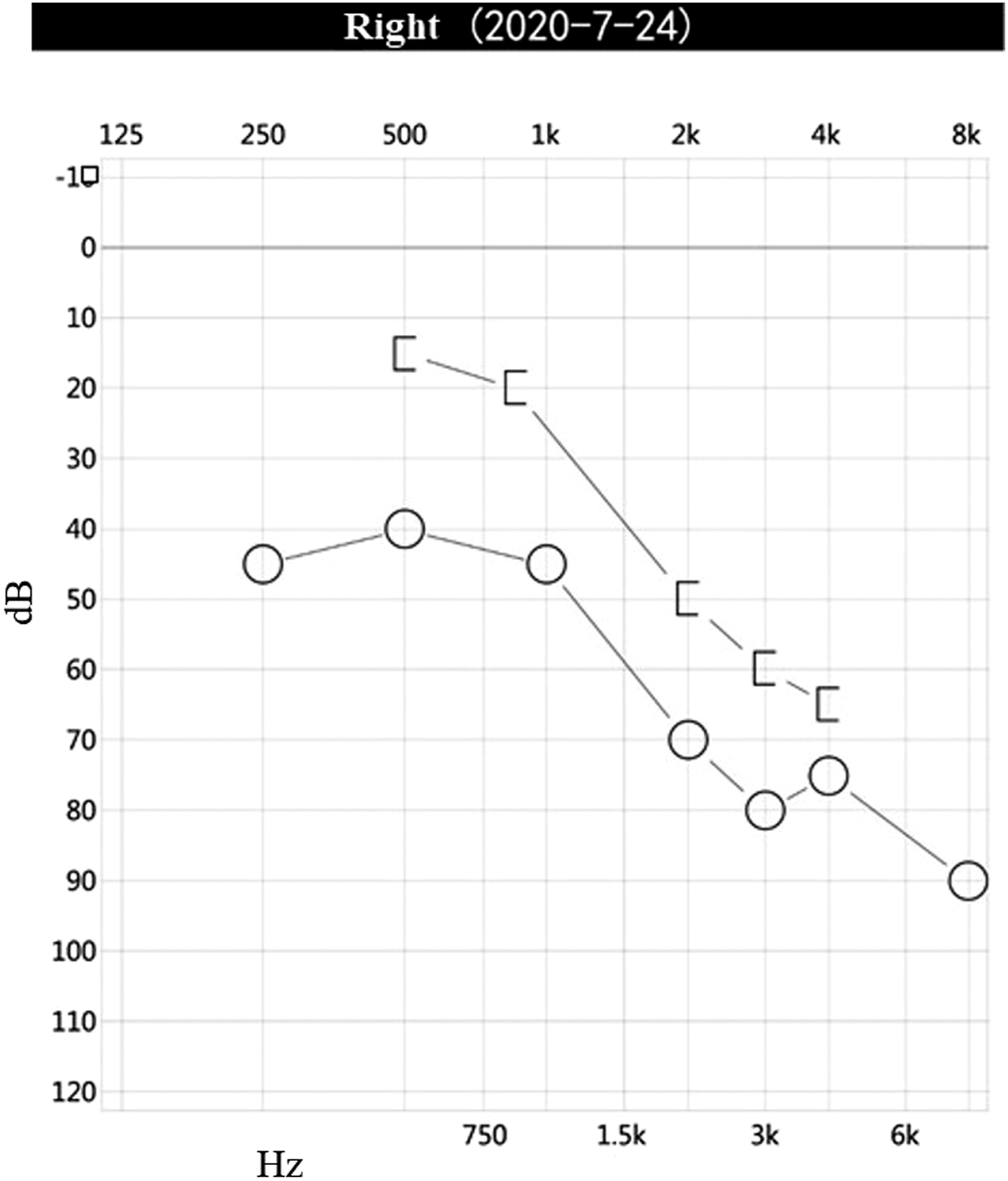
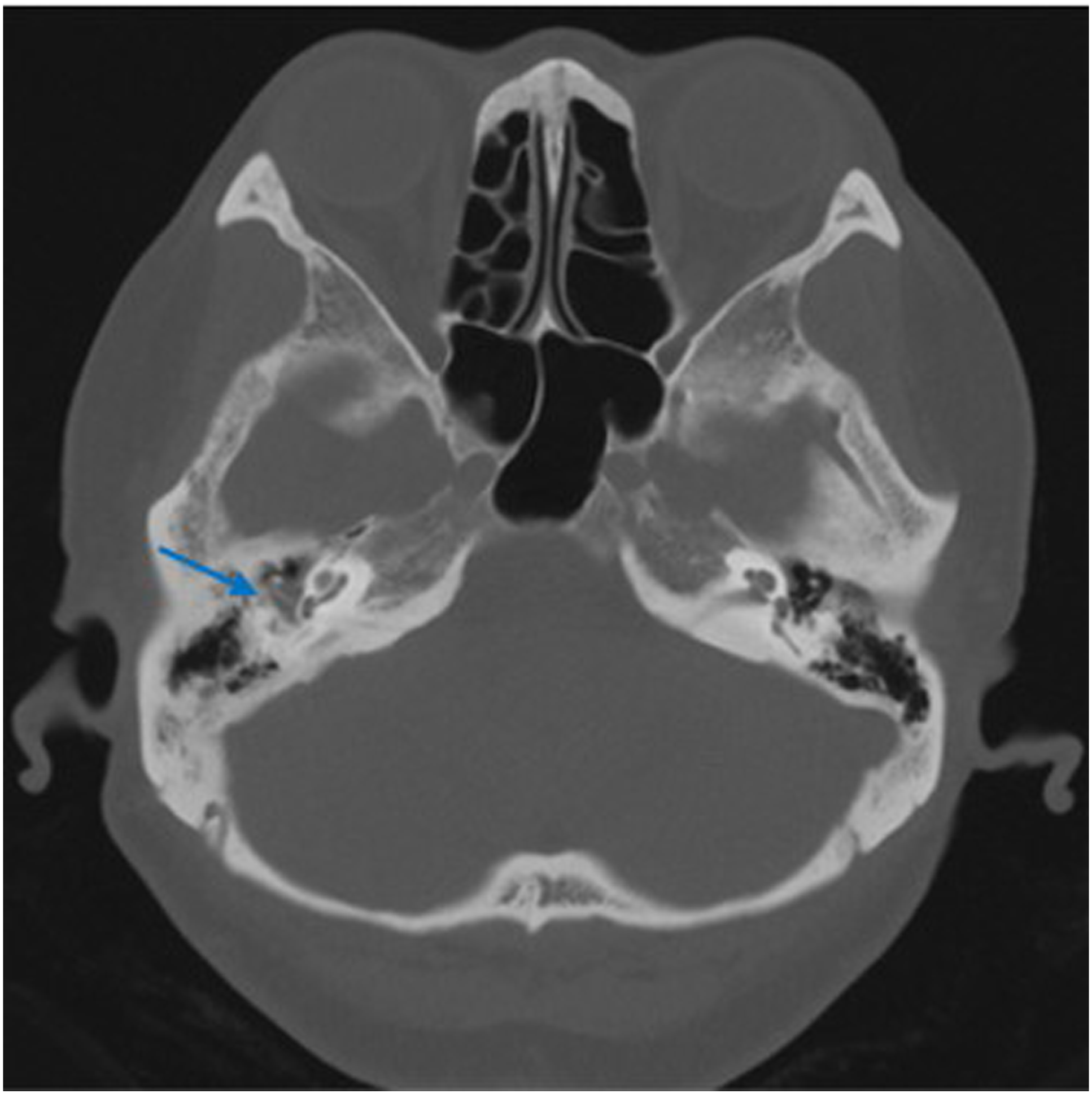
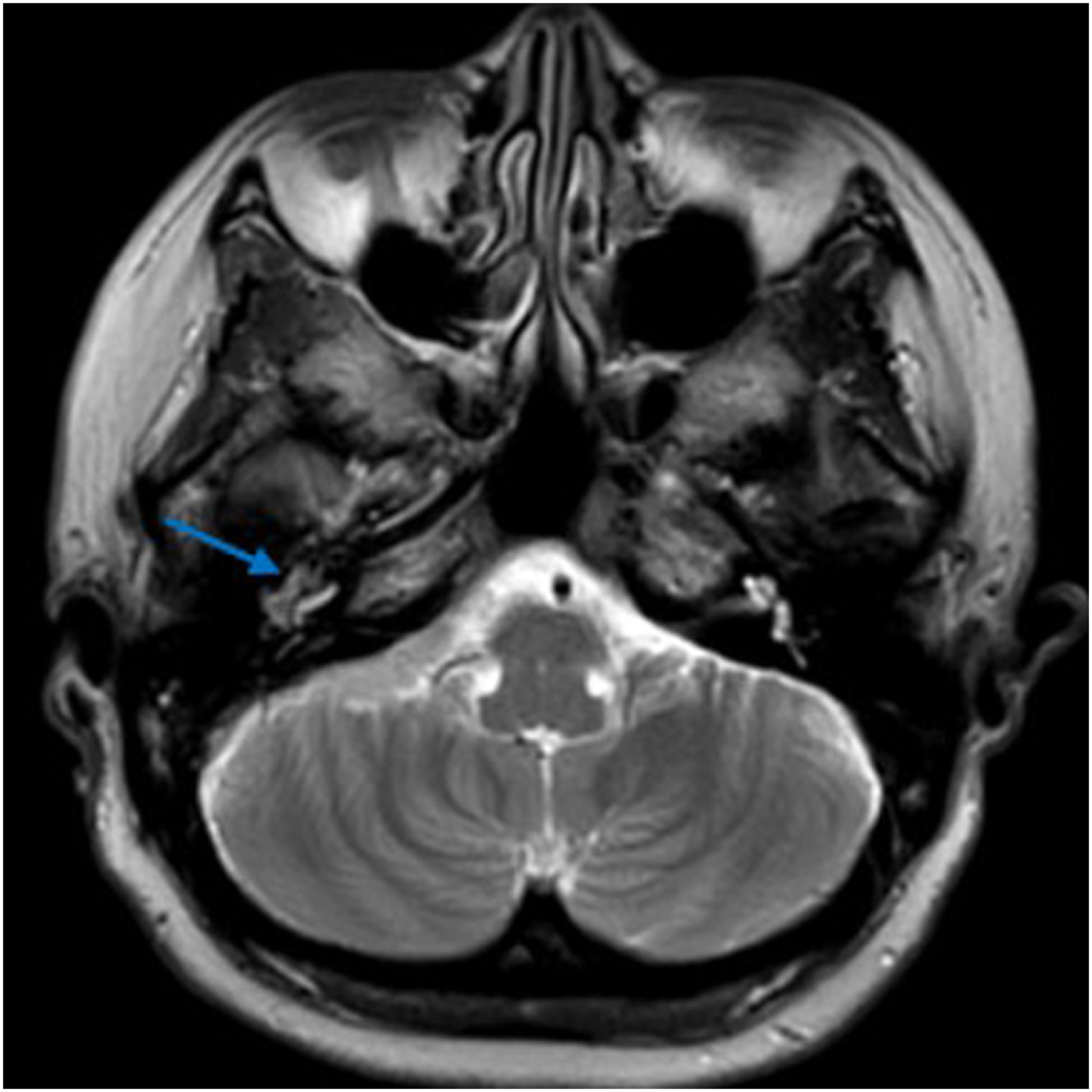
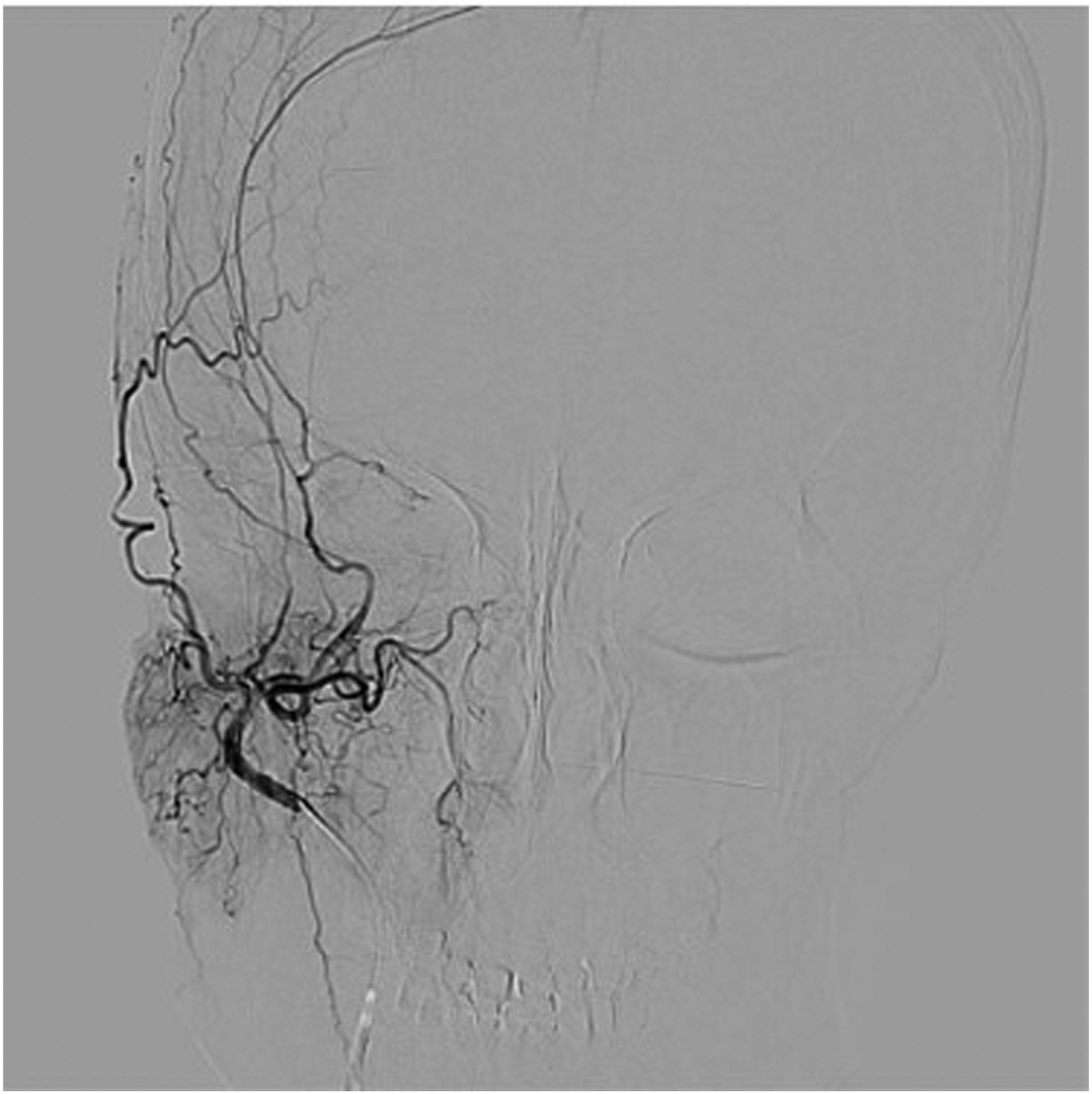
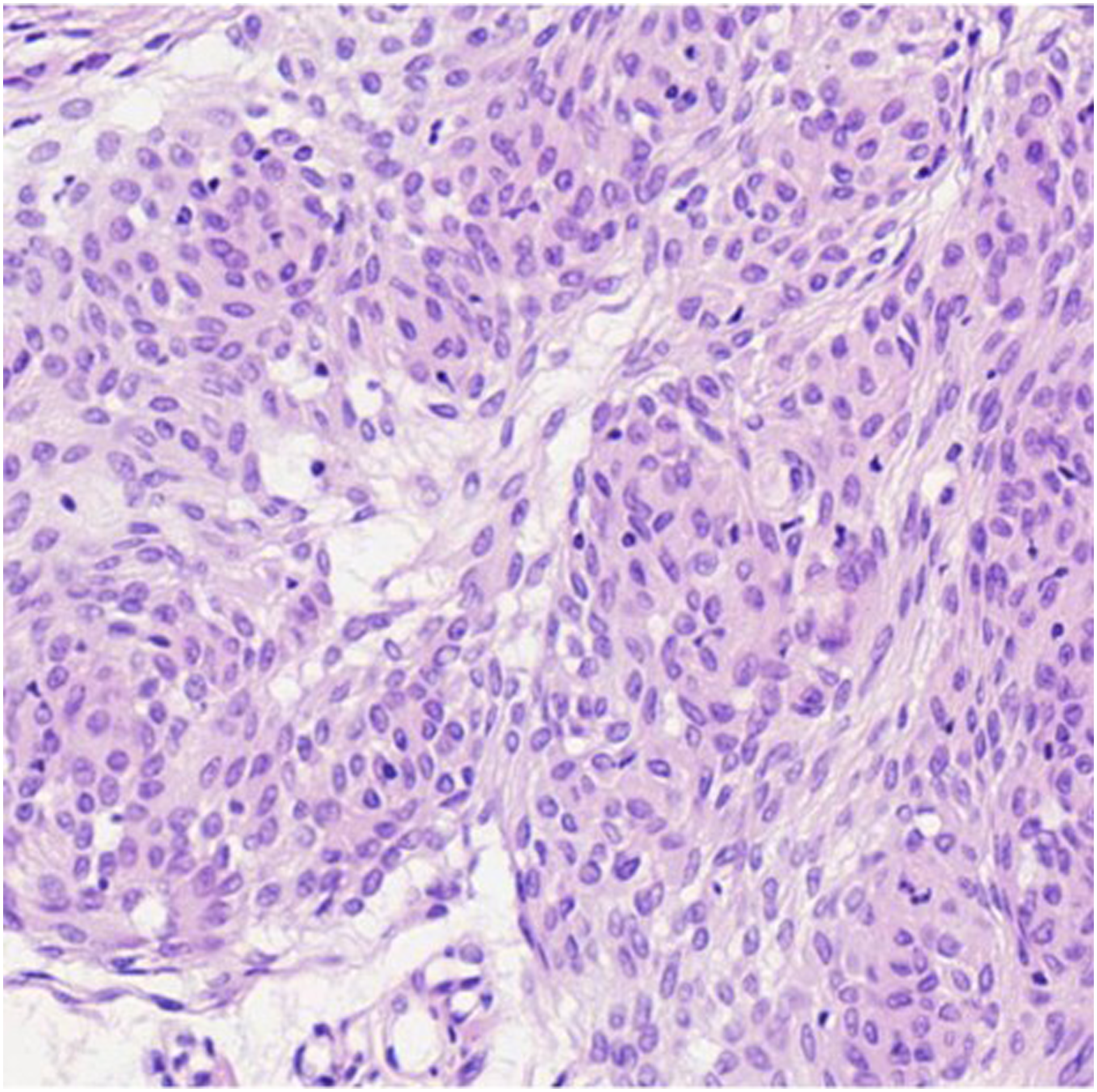
The patient was a 53-year-old woman who suffered for 3 years from otalgia, aural fullness, and progressive hearing loss in the right ear. She was found to have a tympanic effusion during an otoscope examination and diagnosed as “secretory otitis media” in the local hospital. Treatment, such as with decongestants and myringotomy with insertion of the grommet, was performed, but the effect was limited. Symptoms were relieved after insertion of the grommet, but few secretions were drained from the tube. These symptoms recur over a 3-year period. The patient had sudden deafness in the right ear 10 years ago. After conservative treatment, hearing was restored, but a sequela of persistent auditory hypersensitivity was left. She had no headache, facial paralysis, or other related symptoms and no history of chronic disease. Physical examination showed that the tympanic membrane of the right ear was intact, slightly bulging, and the posterior inferior quadrant of the tympanic membrane was reddish. The facial motion was symmetrical, and no tongue deflection was found. No obvious positive signs were found on the physical examination of the nasal cavity, pharynx, larynx, and neck. Pure-tone audiometry showed conduction deafness of the right ear with a gap of 20dBnHL. The average hearing threshold had dropped by about 20dBnHL during 6 months, and hearing loss fluctuated (Figures 1 and 2). The acoustic immittance measurement showed type B in the right ear. High-resolution CT (CT) showed the density of soft tissue in the right mastoid and tympanum (Figure 3), and the right tympanic membrane had thickened. Due to the patient’s history of metal allergy, she did not complete MRI with gadolinium enhancement. Magnetic resonance imaging of the internal auditory canal showed a long T1 and long T2 signal in the cells of the tympanum and the mastoid process of the right middle ear (Figure 4). To exclude vascular lesions in the tympanum and jugular foramen and to determine the presence of major blood supply vessels in case of necessary vascular embolization, digital subtraction angiography (DSA) was performed before surgery. Angiography showed that the inferior branch of the tympanum of the right ascending pharyngeal artery increased, and the blood supply area in the parenchymal stage was slightly enhanced, considering inflammatory lesions (Figure 5). An exploratory tympanotomy was performed and a red mulberry-shaped mass was found on the surface of the promontory, with the ossicular chain not eroded. The tympanic membrane was reconstructed with temporal fascia muscle. The mass was sent for fast frozen pathology, which showed disordered epithelial nests and mild atypia. The tumor was considered to have epithelial origin, but whether benign or malignant was uncertain. After the operation, she received anti-infection treatment and a routine dressing change and was discharged 7 days later. Paraffin pathology is consistent with epithelial meningioma (Figure 6), and the immunohistochemical results showed STAT6 (cytoplasm +), CD34 (vascular +), desmin (−), caldesmon (weak +), CK (nest surrounding +), EMA (+), ERG (vascular +), and S100 (−), Ki-67 (1% +). 2 months after the operation, the operating cavity had been epithelialized and the tympanic membrane was intact. There were no signs of recurrence during a 12-month follow-up. Audiogram demonstrating a fluctuating conductive hearing loss in the right ear. Audiogram demonstrating a fluctuating conductive hearing loss in the right ear. High resolution computed tomography (CT) in the axial plane shows in the right middle ear and mastoid cells a soft tissue mass (arrow), and the tympanic membrane thickens. The ossicular chain was intact and was not displaced. There was no evidence of destruction of the petrous bone or mastoid. MRI of the temporal bones (without gadolinium enhancement due to patient allergies) showed that the flaky long T1 long T2 signal shadow in the tympanum and mastoid cells of the right middle ear (arrow), and the shape of the right cochlea and semicircular canal was normal. Digital subtraction angiography (DSA) showed that the inferior tympanic terminal branch of the right arteriae pharyngea ascendens increased slightly and light staining was observed in the area of blood supply in the parenchymal phase. The tumor cells are round and oval, with mild cells, no obvious atypia, local vortex arrangement, and a small number of psammoma bodies can be seen (HE, original magnification×200).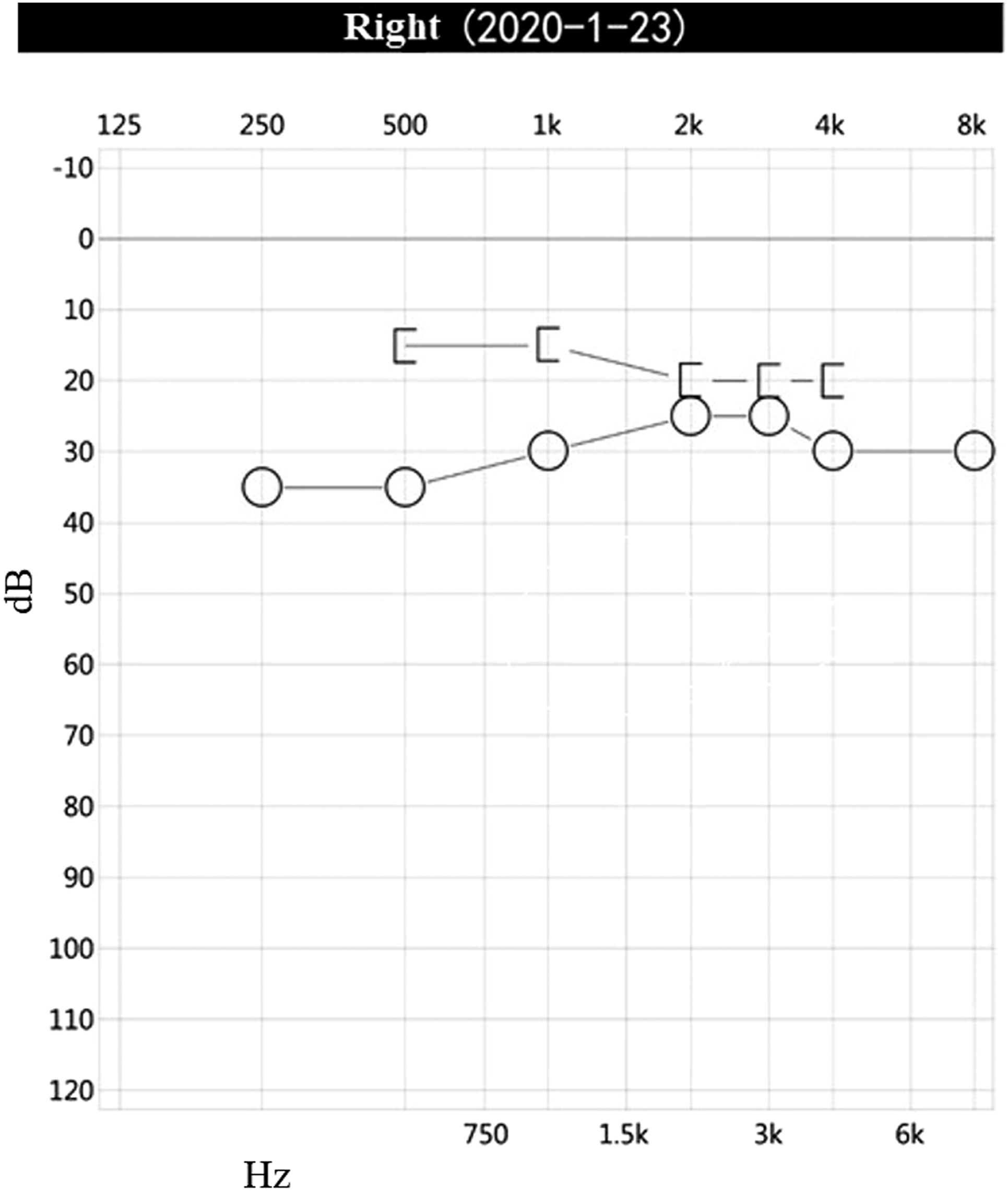
Discussion
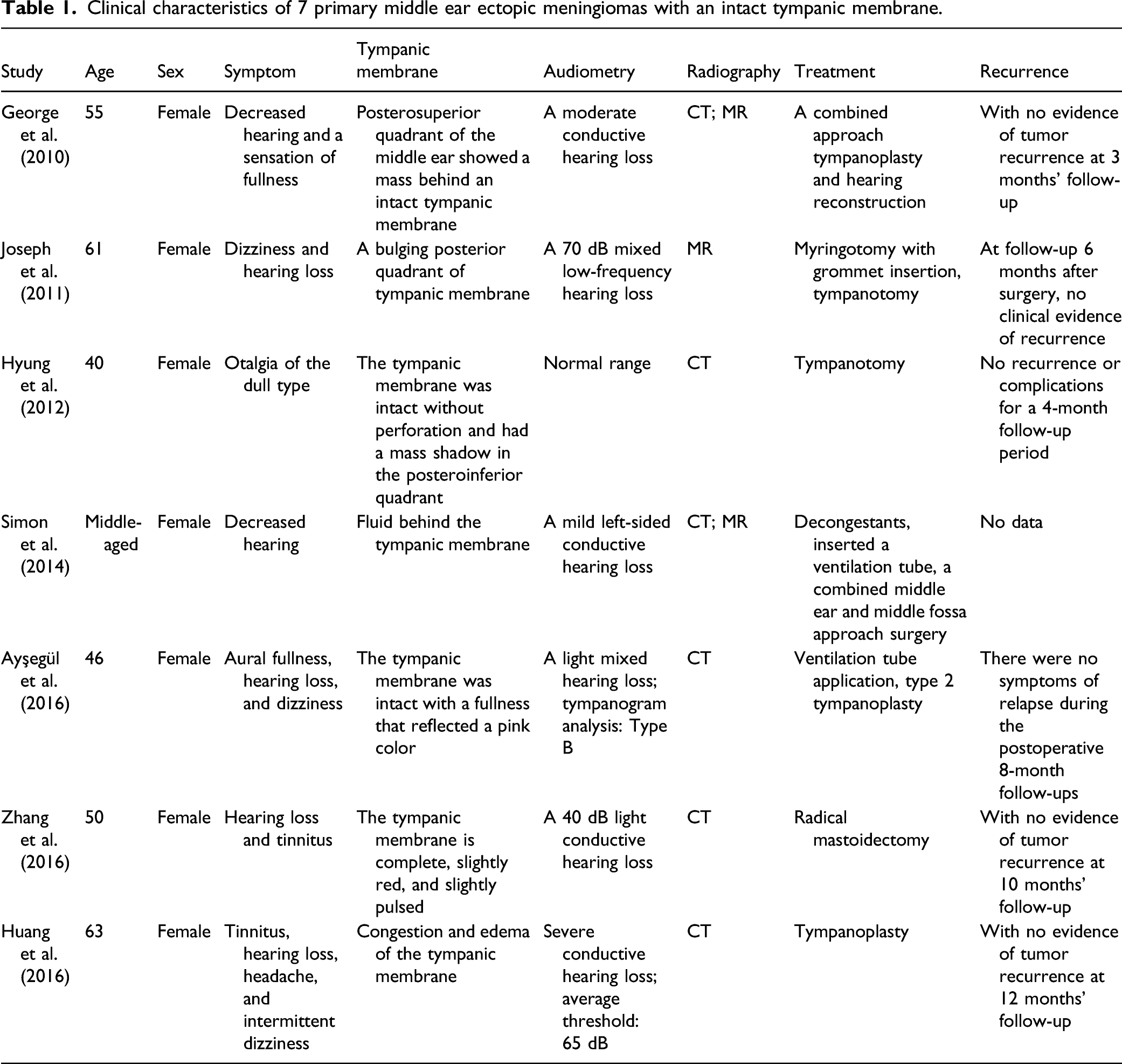
Clinical characteristics of 7 primary middle ear ectopic meningiomas with an intact tympanic membrane.
In the early stage of the disease, primary ectopic meningioma of the middle ear with intact tympanic membrane and secretory otitis media is difficult to differentiate and therefore is often misdiagnosed and mistreated. In cases where conventional conservative treatment is ineffective, benign or malignant tumors, including meningioma, should be considered in diagnosis. When there is no obvious drainage of serous fluid after the myringotomy or an unclear neoplasm is found in the middle ear cavity, an exploratory tympanotomy should be performed. Biopsy should be performed with caution for special pathological types of lesions such as paraganglioma of the middle ear or schwannoma of the facial nerve due to the risk of massive hemorrhage and facial paralysis. 13 In the limited published cases of primary ectopic meningioma confined to the tympanic cavity, we have not found any reports with symptoms of previous sudden deafness and hyperacusis. Tumors, including meningioma, in the cerebellopontine area are a common cause of sudden deafness. Toro et al. 14 reported a case of sphenoid wing meningioma with sudden deafness as the primary symptom. Due to the long duration of sudden deafness and the failure to perform related imaging tests at the time of onset, we cannot establish a correlation between the occurrence of initial sudden deafness and the existence of meningioma of the middle ear. Among the common causes of diseases of the peripheral and central auditory system, endocrine system, infectious diseases, and other causes of auditory hypersensitivity, 15 middle ear meningioma may not be associated with long-term persistent auditory hypersensitivity in this patient. It remains to be studied whether sudden deafness and long-term auditory hypersensitivity after treatment can be used as the primary indication for the diagnosis of middle ear meningioma in more related cases.
Nager et al. 16 divided temporal meningioma into 2 types: type 1 is more common, manifesting as an extension of intracranial meningioma and type 2 has no intracranial extension, and they pointed out that type 2 should be clearly diagnosed by MRI. Computed tomography features of temporal meningioma are diffuse “hairy” trabecular hyperplasia without destroying the trabecular structure, thickened bone and irregular edges, meningioma invading the middle ear cavity manifests as a mass with a density of soft tissue surrounding the auditory ossicles, without erosion or destruction. 17 After injection of gadolinium, the temporal meningioma shows uniform enhancement of soft tissue in the T1-weighted image on MRI. Another unique feature of the MRI is the “dural tail sign.” The dural tail sign is an en plaque linear dural enhancement along the floor of the middle or posterior cranial fossa. 18 Glomus jugulare paraganglioma 19 can be distinguished from it according to the characteristics of the “salt-pepper sign” or “serpentine effusion” on MRI, and enhanced MRI has higher sensitivity. 20 Gadolinium-enhanced MRI is superior to CT scan in distinguishing peripheral extension of intracranial meningioma and primary extracranial meningioma. 5 Currently, most scholars recommend that patients with unexplained or refractory secretory otitis media be examined by temporal bone CT. When CT cannot exclude other spaces occupying the space, such as temporal bone meningioma, enhanced MRI will help confirm the diagnosis and give the exact scope of the disease. 9 Previous studies have compared multislice spiral CT angiography (MSCTA) and DSA in patients with meningioma, and the results revealed that DSA showed obvious advantages over MSCTA in displaying blood vessels near the skull. 21 There is still a lack of relevant research comparing the advantages and disadvantages of DSA and enhanced MRI for the diagnosis of temporal bone ectopic meningioma. The DSA of this patient showed light staining in the tympanic area on the right side and diffuse distribution of fine blood vessels, except for paraganglioma and other highly vascularized tumors that occur in the tympanic cavity, greatly improving operation safety. The types of meningothelial, psammomatous, and fibroblastic are the most common pathological types of temporal bone meningiomas. 22 Histologically, cells are arranged in nests and whorls, and most of the cells have relatively uniform, oval nuclei and clear to faintly eosinophilic cytoplasm, with indistinct cytoplasmic borders. Immunoreactivity for EMA is a characteristic finding, while the expression of the S100 protein varies. 23
Surgical resection is the main treatment for middle ear meningioma. Lester et al. 5 followed up 36 cases of temporal bone meningioma during an average of 15.5 years. A total of 10 cases had local recurrence between 5 months and 4.8 years after the initial visit. The recurrence site is basically the same as the original tumor site. The specific origin site, the patient’s sex, bone invasion, histological type, or the percentage of Ki-67 immune response cells did not change the long-term prognosis of the patient. In most cases, complete eradication through surgery is often difficult due to the lack of clear boundaries, so long-term follow-up and periodic examination are important in preventing recurrence.
Conclusion
Primary tympanic meningioma with an intact tympanic membrane is prone to be misdiagnosed and mistreated during the initial visit. For cases with recurrent symptoms similar to secretory otitis media, the image of the tympanic membrane can provide valuable information. Computed tomography and even MRI should be performed in time to exclude lesions that occupy the middle ear space and obtain intervention at an early stage. Patients should also be reviewed regularly after surgery to prevent disease recurrence.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.