
Abstract

Keywords
A 10-year-old male with a history of X-linked chronic granulomatous disease (CGD) presented with 12 months of non-productive cough, dysphonia, and weight loss. Diagnosis of CGD was confirmed 5 years earlier based on cervical lymphadenopathy demonstrating granulomas with low neutrophil oxidative burst. Genetic analysis identified a missense mutation in CYBB located on the X chromosome. Symptoms developed after endotracheal intubation for a cervical lymph node biopsy and flexible bronchoscopy. Despite 6 weeks of oral prednisone, he exhibited unlabored inspiratory stridor and flexible laryngoscopy revealed a bulbous, obstructive epiglottis. These findings prompted urgent surgical evaluation to secure his airway and obtain tissue samples.
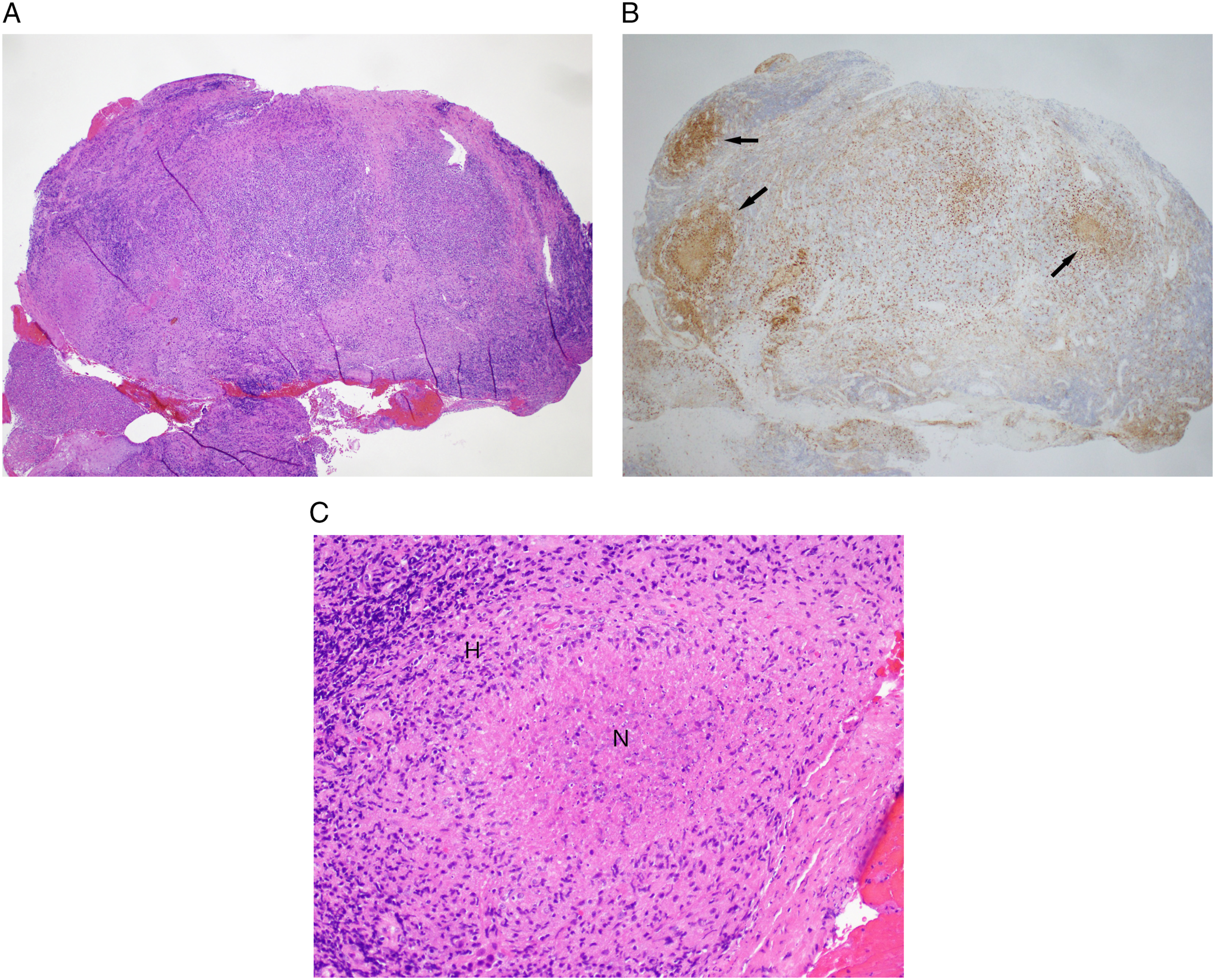
Airway endoscopy confirmed friable, edematous mucosa of the supraglottic larynx (Figure 1A) with less severe changes to the glottic structures (Figure 1B). Epiglottis biopsy revealed necrotizing granulomas, acute and chronic inflammation, and negative cultures consistent with CGD (Figures 2A-C). He was successfully extubated after 10 days of systemic dexamethasone and underwent several additional interventions to improve the airway caliber. This included inhaled corticosteroids, intralesional triamcinolone injections and two CO2 laser resurfacing techniques. Although he was discharged home on 2 mg of daily dexamethasone, his throat discomfort progressed within 4 weeks reflecting extensive upper airway granulomatous changes. Given advanced airway obstruction, he was electively intubated and a tracheostomy was performed. Three weeks after tracheostomy, he was discharged on trimethoprim-sulfamethoxazole, interferon gamma-1b, azathioprine, and a weaning dose of daily prednisone. He continues to tolerate daily capping and nightly humidification while awaiting clinical trial enrollment. (A) Direct laryngoscopy of laryngeal chronic granulomatous disease (CGD) manifestations identifying a narrowed glottic inlet (thin arrow) and granulomatous blunting of supraglottic landmarks (thick arrow). (B) Direct laryngoscopy revealing granulomatous changes of the false vocal folds (thick arrow) and true vocal folds (thin arrow) with patent glottic caliber (asterisk). (A) Hematoxylin & eosin (H & E) (4X). The biopsy tissue is occupied by an intense lymphoplasmacytic and histiocytic infiltrate in a vaguely nodular arrangement. (B) CD68 (4X). Immunohistochemical staining for CD68, which marks histiocytes and macrophages, highlights the histiocytic granulomas within the inflammatory infiltrate (arrows). (C) H & E (20X). Some of the granulomas show central necrosis (N) in the center of the histiocytic infiltrate (H). Gram stain, Fite stain, and Gomori methenamine silver stain on the granulomas were negative for bacteria, acid-fast mycobacteria, and fungi, respectively.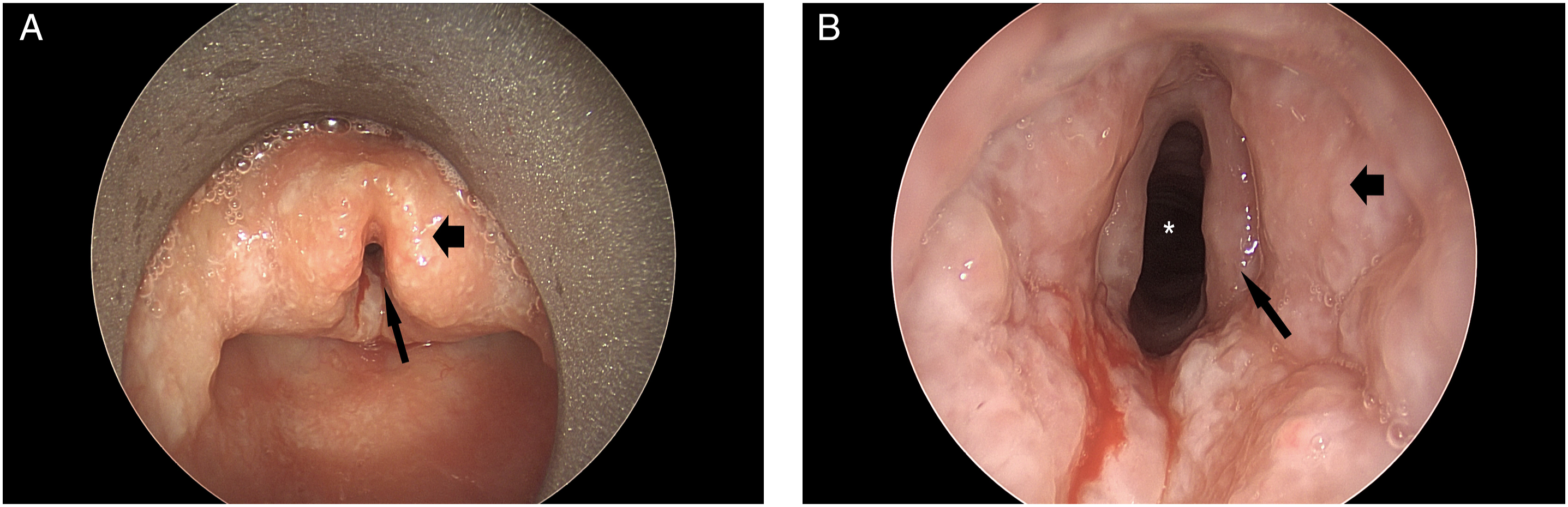
Chronic granulomatous disease is a primary immunodeficiency 1 affecting 1 in 200 000 births often through an X-linked recessive inheritance. 2 Defects in nicotinamide adenine dinucleotide phosphate (NAPH) oxidase subunits impair generation of reactive oxygen intermediates (ROIs) necessary for microbial phagocytosis. 3,4 Ineffective production of superoxide anion and other ROIs leads to recurrent infections, granulomatous complications, and early mortality. 5 Inflammatory aspects of CGD are challenging to manage and present in the gastrointestinal system, lungs, genitourinary tract, and eyes. 6
Inflammatory sequalae of CGD occur through unclear and likely multifactorial mechanisms. 7 Etiologies include dysregulated cytokine production along with increased scar formation, wound dehiscence, and strictures. 5 Endotracheal intubation may have incited the cascade of inflammation seen in this case resulting in mucosal friability and edema. These complications are twice as likely in children with X-linked CGD as those with autosomal recessive inheritance. 6 Inflammatory manifestations are found in the gastrointestinal system, urogenital tract, lungs, and eyes, characterized by noncaseating granulomas unrelated to infection. 6 To date, only three case reports, all published over 30 years ago, discuss laryngeal manifestations of CGD in children and young adults. 8 -10 In two of those three patients, there was no improvement with antibiotics or systemic steroids and a tracheostomy was required. 8,10 Obstructive symptoms similar to the index case were described.
Endoscopic airway management has advanced since laryngeal CGD was initially described. Notably, mucosal findings are consistent with other inflammatory processes such as sarcoidosis 11 -13 and Crohn’s supraglottitis. 14,15 Management included submucosal steroid injections described for sarcoidosis 16 and CO2 laser photoreduction described as a “pepper pot” technique. 17 Laryngeal resurfacing has been used for sarcoidosis, 13,17 idiopathic non-granulomatous supraglottitis, 18 and Crohn’s disease. 15 This approach creates small mucosal marks separated by islands of mucosa. This allows for edema extrusion, causes mucosal scarring to cartilage, and eliminates potential space for recollection. 18 While results were initially promising in this case, advancements were quickly lost with disease progression. We recommend this technique, but surgeons should recognize the uncertainty of disease progression in CGD.
Medical management of CGD utilizes prophylactic antibiotics and antifungals. 14 Inflammatory manifestations of CGD usually respond to steroids; however, immunosuppressants and biologics may play a role in refractory cases. 3,6 Definitive treatment has been demonstrated with hematopoietic stem cell transplantation with much current interest in gene therapy. 19,20 These treatment frontiers may ultimately produce a cure for this disease process.
Several management points are worth emphasizing. First, symptoms can be insidious with severe impairment occurring over a few months. Therefore, otolaryngology referral should be considered early if aerodigestive involvement is suspected. Second, safely securing the airway included dialogue with an anesthesiologist to prevent catastrophic complications. Experienced airway physicians should be involved as mucosal friability and loss of landmarks makes multiple intubation attempts risky. Third, although adjunct strategies may be helpful, if the underlying pathology progresses, children may need a tracheostomy. Long term outcomes of tracheostomy placement, particularly as it pertains to systematic inflammation, are unknown. Finally, children with CGD require a multidisciplinary approach. Pediatric immunology, infectious disease, and critical care should work closely with pediatric otolaryngology, anesthesiology, surgery along with nursing, respiratory therapists, and speech therapists to ensure appropriate adjustments and interventions when necessary.
Footnotes
Acknowledgments
The authors would like to thank Charles Timmons, MD, PhD, for providing the representative images and pathology impressions of biopsy specimens from this case.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Statement of Informed Consent
Written informed consent was obtained from the patient’s legal guardian for the publication of this case report.