
Abstract
Significance Statement: Primary middle ear inverted papilloma is an exceedingly rare finding posing a diagnostic challenge, as symptomatology often mimics common clinical entities like serous otitis media. Clinical and radiological findings are not specific, whilst high recurrence rates, local destruction, and potential malignant transformation constitute an overall demanding surgical challenge, requiring aggressive procedures. We report the case of a primary inverted papilloma of the middle ear, discussing diagnostic and therapeutic issues.
Case Description
A 59-year-old male was referred to our department due to progressive hearing loss and prolonged sensation of right-sided aural fullness. There was no history of other otologic symptoms, apart from occasional episodes of right sided tinnitus, lasting less than a week.
Otomicroscopy revealed a retracted, right tympanic membrane as well as evidence of what appeared to be secretory otitis media. The left ear was normal. Both Weber and Rinne tests indicated conductive hearing loss on the affected side, partially confirmed by pure tone audiometry that revealed mild bilateral symmetrical sensorineural hearing loss, combined with a 40 dB conductive component in the diseased ear. Full head and neck examination, including nasal and nasopharyngeal fibroscopy, did not reveal any pathological findings.
Courses of antibiotics and corticosteroids failed to achieve any improvement; thus, a grommet was inserted, which only temporarily and partially improved the patient’s symptoms. On follow-up otoscopy 1 month after grommet insertion, it was established that grommet was extruded to the ear canal and a fleshy, bleeding, irregular papillomatous lesion erupted, protruding out of the remaining eardrum perforation (Figure 1A). (A) Grommet is extruded to the ear canal and a fleshy, bleeding, irregular papillomatous lesion is protruding out of the remaining eardrum perforation (white arrow). On MRI, (B) the tympanic cavity and mastoid air cells are largely opacified by soft tissue density mass occupying them.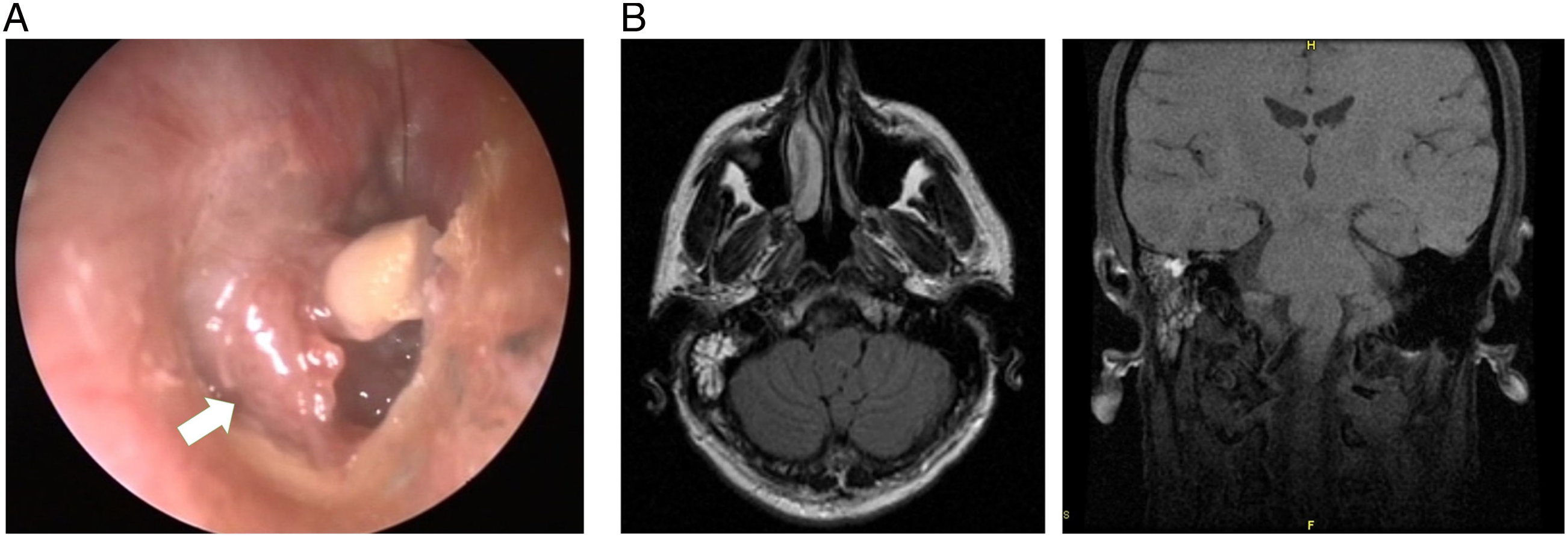
On MRI, the tympanic cavity appeared largely opacified by a soft tissue density mass occupying the middle ear, antrum, and a large portion of mastoid air cells (Figure 1B). The tissue did not significantly involve or erode the ossicles. The Eustachian tube, fallopian canal, and labyrinth were intact. Imaging largely excluded encephalocele and meningocele from the differential diagnosis; thus, the lesion underwent biopsy under local anesthesia and histology confirmed that biopsy material consisted of fragments of middle ear Schneiderian type papilloma (Figure 2). There were no signs of dysplasia or malignant transformation. Papillary structures composed of fibrovascular cores with moderate chronic inflammatory infiltrates, lined by ciliated pseudostratified columnar epithelium. “Inverted” growth of the epithelium into the connective tissue. (A) H&E, × 20; and (B) H&E, × 100.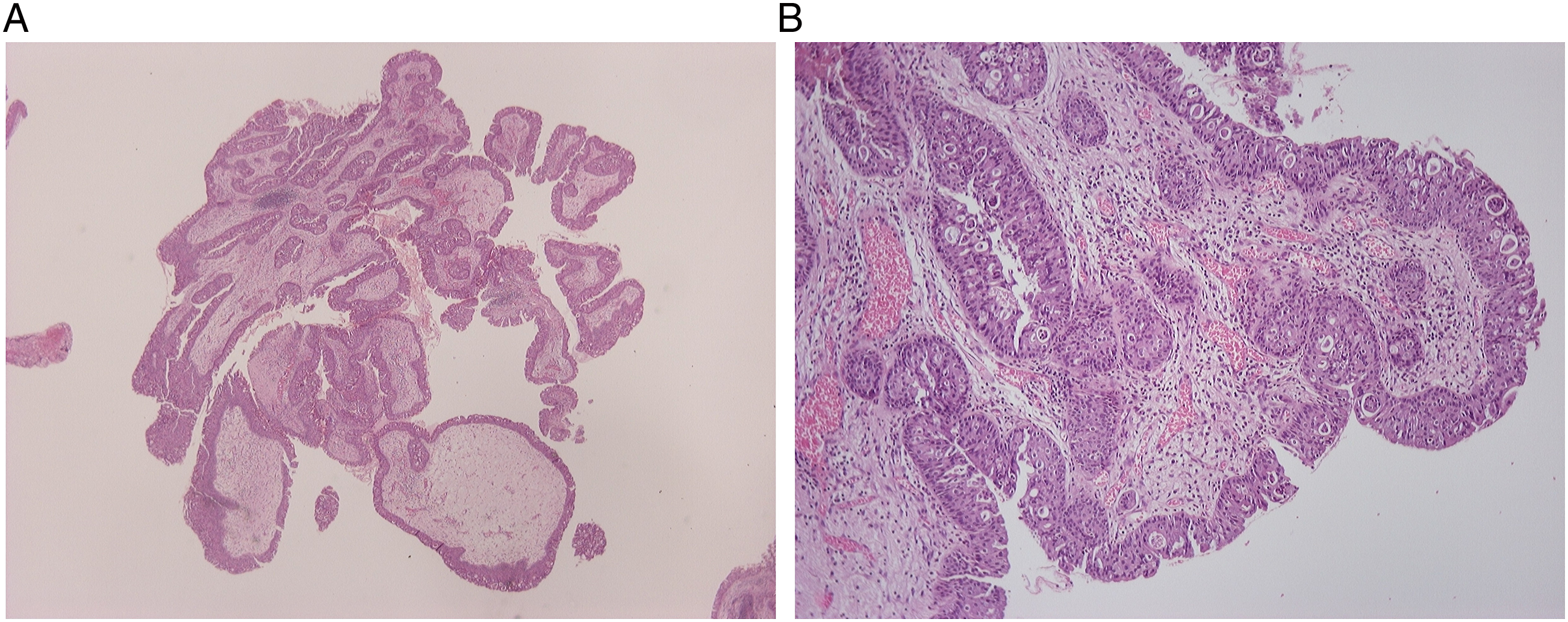
The patient underwent a canal wall up mastoidectomy to address the middle ear and mastoid mass. The middle ear cavity was exposed and found filled by a scarcely bleeding, multilobulated, polypoid tissue. The lesion originated from the promontory and depicted extension toward the epitympanum. All polypoid tissue was resected by a “combined approach” via both the tympanic cavity and mastoid (Figure 3). Ossicular chain appeared intact and mobile. Fallopian canal, tegmen, and, more importantly, Eustachian tube orifice were carefully inspected intraoperatively for any tumor involvement, and no extension was identified. As middle ear inverted papillomas depict high recurrence rates, extensive exenteration of the mastoid cells was considered necessary. Cartilage–perichondrium composite graft was harvested and placed over the intact ossicles. Postoperative period was uneventful, and the patient has been under close follow-up for more than 3 years with no signs of recurrence. Canal wall up mastoidectomy and resection of polypoid tissue through a combined approach. Resecting the lesion (white arrows) from mastoid cells and antrum (A), middle ear cavity (B), ossicular chain and epitympanum (C). Reconstructing with cartilage tympanoplasty (D).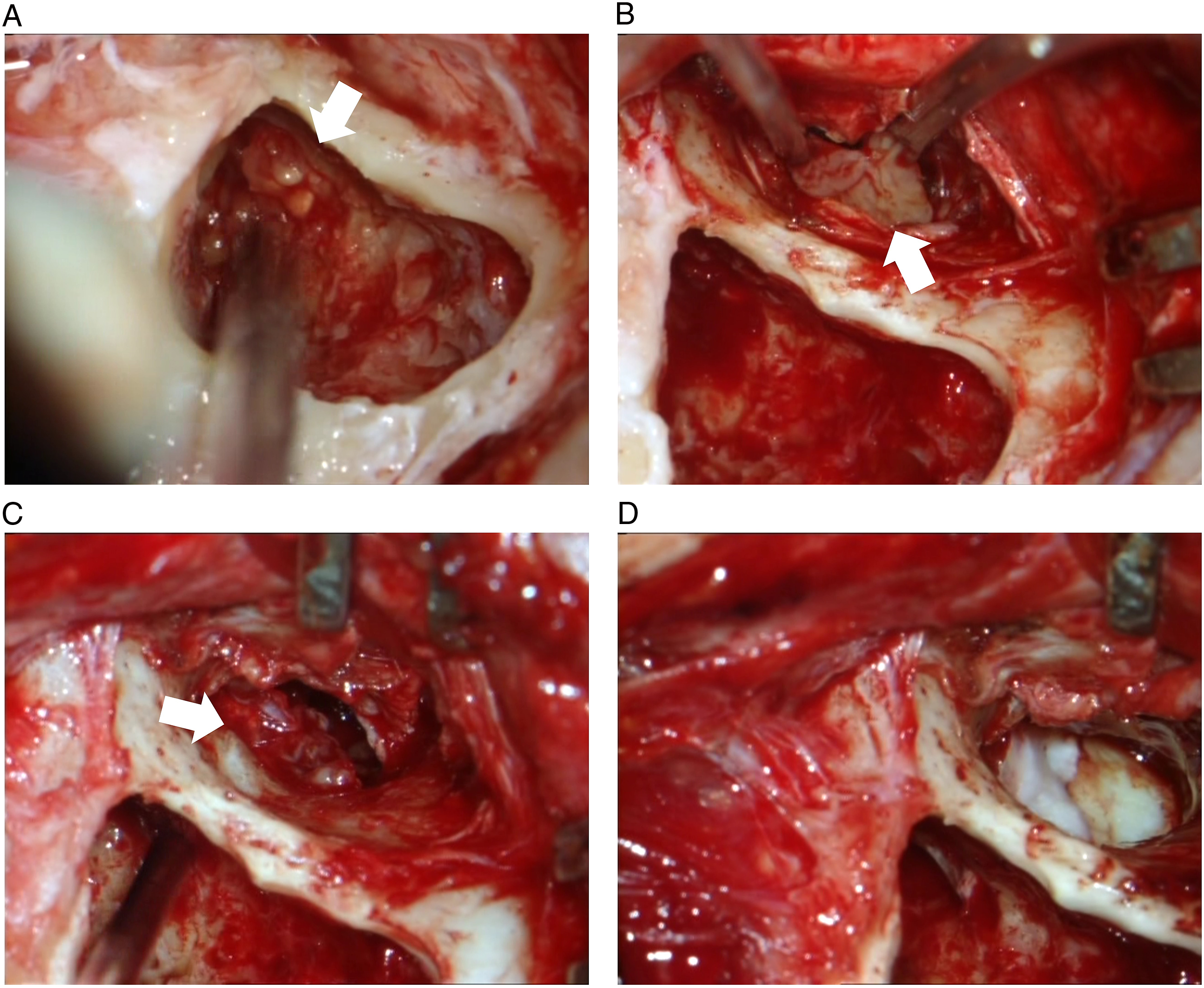
Discussion
Inverted papilloma involving the middle ear is extremely rare, posing a challenge for physicians to define clinical behavior and standardize therapy. Including the current case, 34 cases1,2 of inverted papilloma involving the middle ear have been reported in the English literature, out of which only 20 (counting our case) had no sinus involvement. 1
The origin of middle ear inverted papillomas remains controversial. When there is co-existent ipsilateral paranasal sinus disease, direct extension of tumor through the Eustachian tube is the most likely mechanism (secondary papillomas). 3 Nevertheless, such extension cannot be speculated in absence of sinonasal disease or in lack of evidence establishing temporal or spatial continuity between nasal and aural lesions. As such, these papillomas may arise from abnormality of embryonic migration of ectopic Schneiderian membrane into the mucosa of the tympanic cavity and the Eustachian tube (primary papillomas).4,5 Literature suggests that primary and secondary inverted papillomas of the middle ear should be viewed separately. Primary disease follows a relatively similar course as sinus inverted papillomas, whereas secondary ones frequently exhibit a much more aggressive course, with higher rates of intracranial spread and carcinogenesis. 6
Sinonasal inverted papilloma depicts a tendency to recur following excision. When nasal inverted papilloma involves the middle ear, the literature 7 has reported recurrence as high as 82%, occurring 6 months to 2 years after surgery. In general, the recurrence rate of primary and secondary inverted papilloma of the middle ear is similar. 8
Propensity for malignant degeneration is well recognized in sinonasal inverted papilloma, and inverted papilloma of the middle ear reflects a greater association with malignancy. The risk of malignant transformation is significantly higher for secondary inverted papilloma of the middle ear than for the primary type.7-9
Management of the middle ear inverted papilloma is surgical excision, yet it is extremely hard to define a detailed standard surgical algorithm, due to the rarity of available literature data. Since recurrences are frequent, especially when the excision is not adequate, an aggressive surgical approach is advocated.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.