
Abstract
We report two subjects with tracheobronchopathia osteochondroplastica (TO), including the clinical manifestations, histological findings, and clinical treatments, which were analyzed retrospectively. One patient with TO was a 60-year-old woman, and the other was a 47-year-old man. The main clinical manifestations were cough, chest pain, and dyspnea. Computed tomography (CT) images showed that TO mainly occurred in the trachea and main bronchus. Histological analysis showed inflammatory exudation, squamous metaplasia, submucosal cartilaginous, and ossification. We present the two cases to increase physician and patient awareness of this benign disease and to improve their understanding of the disease manifestations and potential complications.
Introduction
Tracheobronchopathia osteochondroplastica (TO) is an indolent benign tracheal bronchus entity characterized by the development of multiple cartilaginous or osseous submucosal nodules that protrude into the walls of the trachea and bronchus, causing persistent cough, dyspnea, hoarseness, and other symptoms. 1 It is easy to misdiagnose due to its nonspecific clinical presentation, and most patients are asymptomatic in the early stage. With the development of CT as an alternative to bronchoscopy, the diagnosis rate has increased in recent years, although the accurate incidence of TO remains unclear. 2,3 There are still a number of misdiagnosed cases, revealing the need for a better understanding of the disease and its symptoms. Here, we present two cases that may provide a better description of TO and its indicators to assist in the identification and understanding of this disease.
Case report
Case 1
A 60-year-old woman was admitted to our hospital with dyspnea on exertion that had started 1 year previously and edema in her lower extremities that had begun 1 week prior. She had visited a local clinic and underwent chest radiography, which showed inflammation. At that time, a chest CT revealed tracheobronchial wall calcification from the trachea to the opening of the main bronchi. A pulmonary function test showed a moderate obstructive pattern. At the same time, the patient underwent ultrasound, and the results indicated Hashimoto’s thyroiditis of the bilobulated thyroid.
Under bronchoscopy, the entire trachea and the left and right main bronchi were observed to be covered with whitish, irregular nodules (Figure 1). Some areas were nearly obstructed by the nodules. Finally, the tissues were resected for pathological examination. Whitish nodules protrude into the lumen; mucosa was normal (A). Multiple nodular tuberositas of the lower trachea (B). Bronchus wall was thickened with irregular, dense tuberositas, especially thickened with irregular, dense tuberositas, especially in the anterior and lateral walls (C). Hematoxylin and eosin staining showed inflammatory bronchial mucosa (D). Focal ossification of tracheal cartilage underneath the mucosa and squamous metaplasia of the bronchial mucosa (E). Bone marrow was detected and replaced by mature fats (F) (H&E, 20X).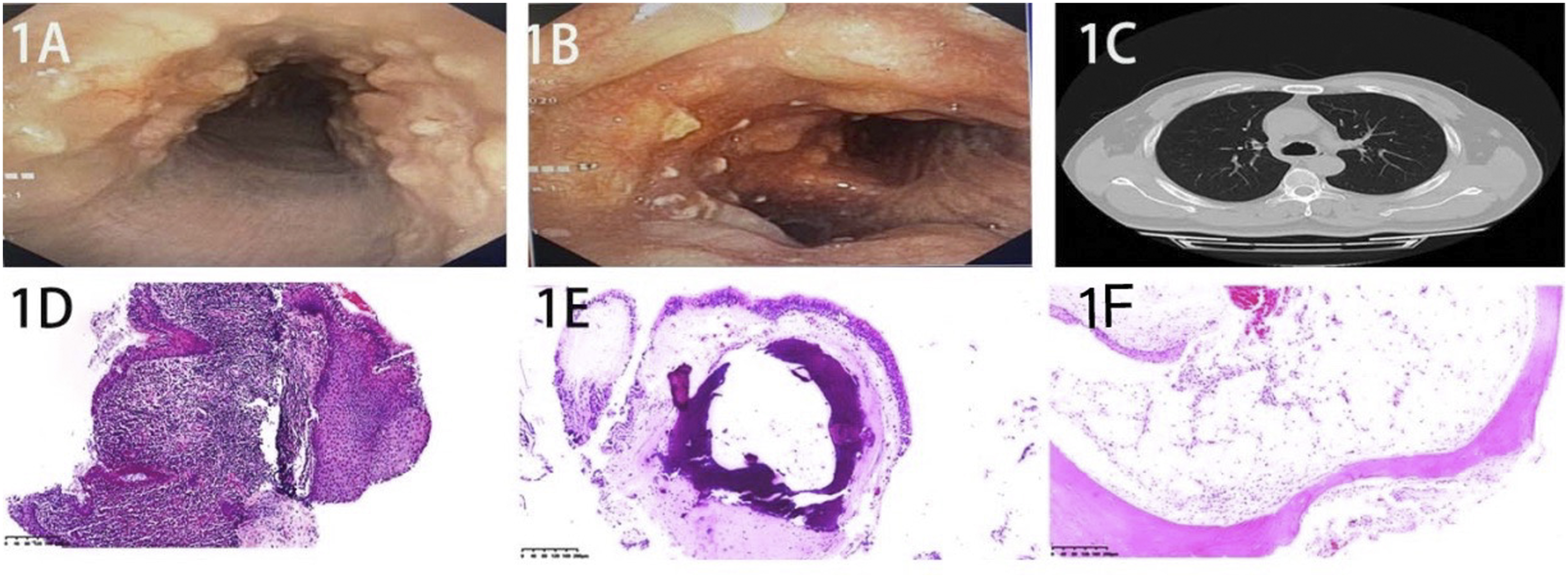
The patient was admitted to the pneumology department, and the decision was made to remove the large nodules and improve the symptoms of dyspnea by argon interventional therapy. She was also given anti-infective therapy at the same time.
Case 2
A 47-year-old man was admitted to our hospital with chest pain and cough. He underwent a chest CT. The image showed irregular changes in the wall of the trachea or bronchus and multiple high-density shadows protruding into the airway (Figure 1). The patient agreed to bronchoscopy and biopsy for pathology. Bronchoscopy showed tracheal stenosis and scattered cartilaginous nodules projecting into the lumen without obstruction.
The patient was not given symptomatic treatment; instead, long-term clinical observation was advised.
Histopathologically, the two cases showed respiratory epithelium with foci of squamous metaplasia and a small amount of lymphocyte and plasma cell infiltration under the mucosa. In the underlying submucosa, we found well-developed cartilaginous and osseous nodules, few fat cells in the osseous tissues, nearby mature bone, and bone marrow replaced by fat (Figure 1).
During follow-up, both subjects had chronic or recurrent cough and expectoration.
Discussion
Tracheobronchopathia osteochondroplastica is a rare benign airway disease that was originally described in 1857 by Wilks. 4 The current incidence rate ranges from 1:400 (.25%) to 3:1000 (.30%) in autopsies and 1:125 (.80%) to 1:10000 (.01%) via bronchoscopy, and the detection rate of this disease is .06% by bronchoscopy in China. 3,5 TO is diagnosed with the widespread use of bronchoscopy, although the lesions are easily misdiagnosed.
The etiology and pathophysiology of TO are not fully understood. Chronic inflammation, genetic factors, congenital anomalies, chemical or mechanical irritation, amyloidosis, tuberculosis, and malignancy have all been considered. 6 -8 The clinical manifestations of TO are variable and nonspecific. Some reports have found that the most frequent presentation is chronic cough and dyspnea, 9 which were complaints voiced by our subjects. Some patients also have restrictive or pulmonary ventilation dysfunction 10 ; our patients had slightly anormal pulmonary function.
In this patient population, chest X-ray is generally normal, and there are no sensitive signs. CT scans can show multiple small nodules with calcification in the trachea and bronchus; some radiologists ignore this evidence due to a lack of awareness of TO. Bronchoscopy is a noninvasive technique that can identify the manifestations of TO; however, multiple nodules of the tracheobronchus under bronchoscopy can be caused by several diseases and are commonly diagnosed as malignancies followed by inflammatory lesions. 11 Reports of the presentation of TO as a single dominant mass in the literature are rare. 12 In summary, pathological biopsy is helpful for further differential diagnosis.
There is no special treatment for TO. The administration of anti-infective treatment, drainage of airway secretions, inhalation of bronchodilators, and administration of corticosteroids may alleviate the symptoms. 13 For some patients, long-term clinical observation may be a good choice. 14 Endoscopic interventional excision can be used to relieve clinical symptoms, but studies with larger sample sizes are warranted to validate these measures.
Conclusion
In conclusion, chest CT and bronchoscopy are helpful for the diagnosis of benign lesions of unknown origin. Although the definitive diagnosis is a pathological diagnosis, multidisciplinary cooperation is key. A large multicenter study needs to be performed to provide new insights into TO.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.