
Abstract
Tracheobronchopathia osteochondroplastica (TO) is a rare disease. Here, we report 5 TO cases treated at our hospital. Bronchoscopy showed typical multiple firm and glossy nodules in all the 5 cases. Conservative treatment effectively alleviated the symptoms. Tracheobronchopathia osteochondroplastica is a manageable disease. Awareness in clinicians is critical to avoid unnecessary treatment in patients with TO.
Introduction
Tracheobronchopathia osteochondroplastica (TO) is a rare, benign, and indolent disease. It is characterized by multiple chondro-osseous submucosal nodules in the distal trachea and the main bronchi. 1 Incidence of TO is believed to be underestimated because most patients are asymptomatic or present with only nonspecific respiratory symptoms. Osteocartilaginous nodules originating from the tracheobronchial cartilaginous rings can cause airway stenosis or obstruction. 2 Patients with TO with this condition may have more severe symptoms such as dyspnea and hemoptysis.
Up to now, almost 500 cases of TO have been reported worldwide, including approximately 140 cases in Japan literatures and 80 cases in Chinese literatures. 3 -5 However, the etiology of TO is still unclear and there is no consensus on the management of this rare disease. Here, we report our experiences with 5 patients with TO admitted in our hospital during the past 20 years.
Case 1
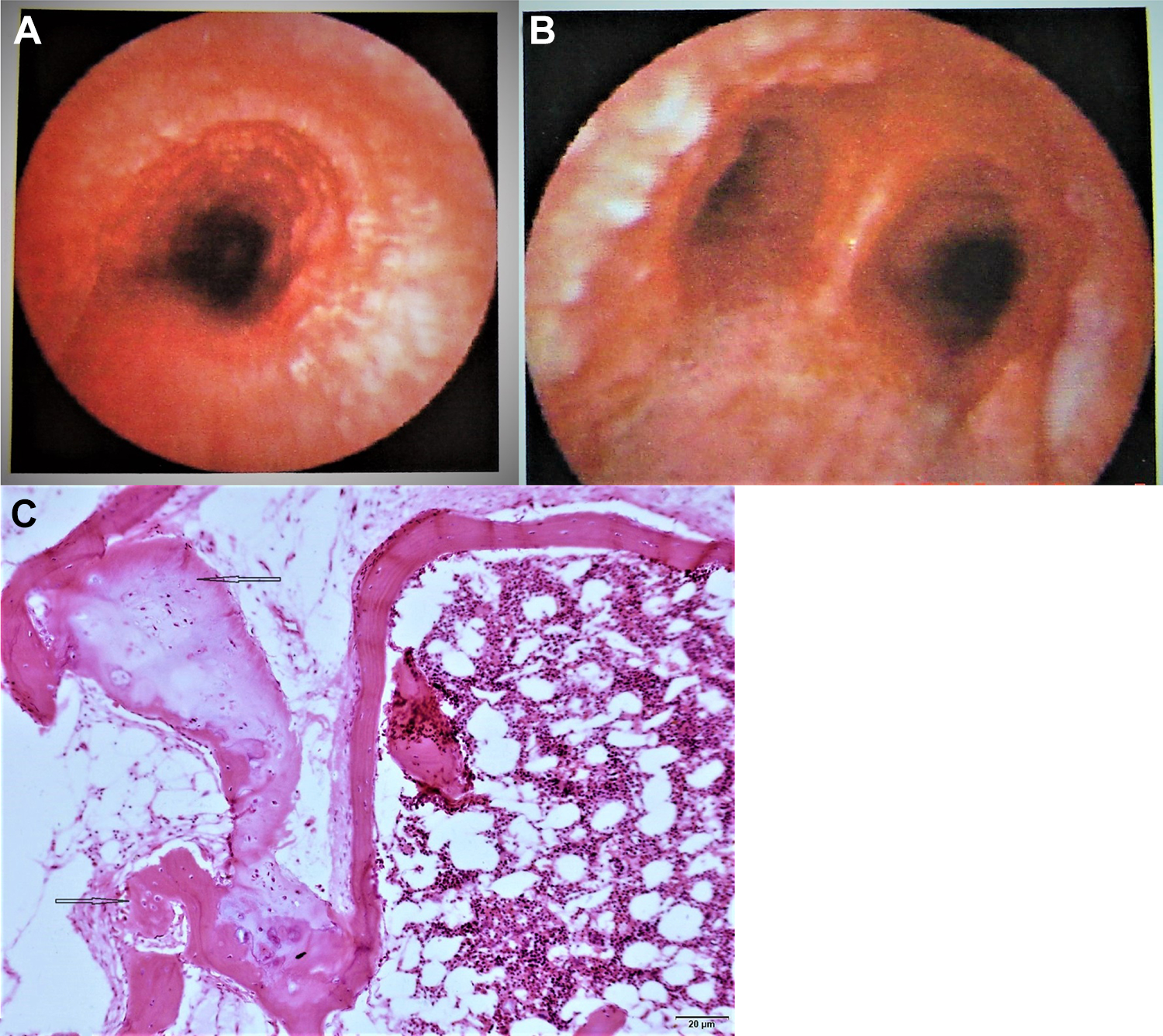
A 45-year-old man was referred to our clinic with recurrent productive cough and fever for 3 years, which had deteriorated in the past 2 months. He had a 6 half-pack-year smoking history and no other remarkable medical backgrounds. Computed tomography (CT) scan showed multiple high-density nodules protruding into the lumen of the trachea and the main bronchi (Figure 1A). Physical examination and pulmonary function test were normal. Fibrobronchoscopy demonstrated diffuse pebble-like nodules throughout the trachea and both main bronchi (Figure 1B). Biopsy and histopathology identified bronchial mucosal epithelial hyperplasia with squamous and submucosal osseous metaplasia, which was consistent with the diagnosis of TO (Figure 1C). The patient responded well to antibiotics and symptomatic treatments, and the symptoms had been well controlled for 6 years.
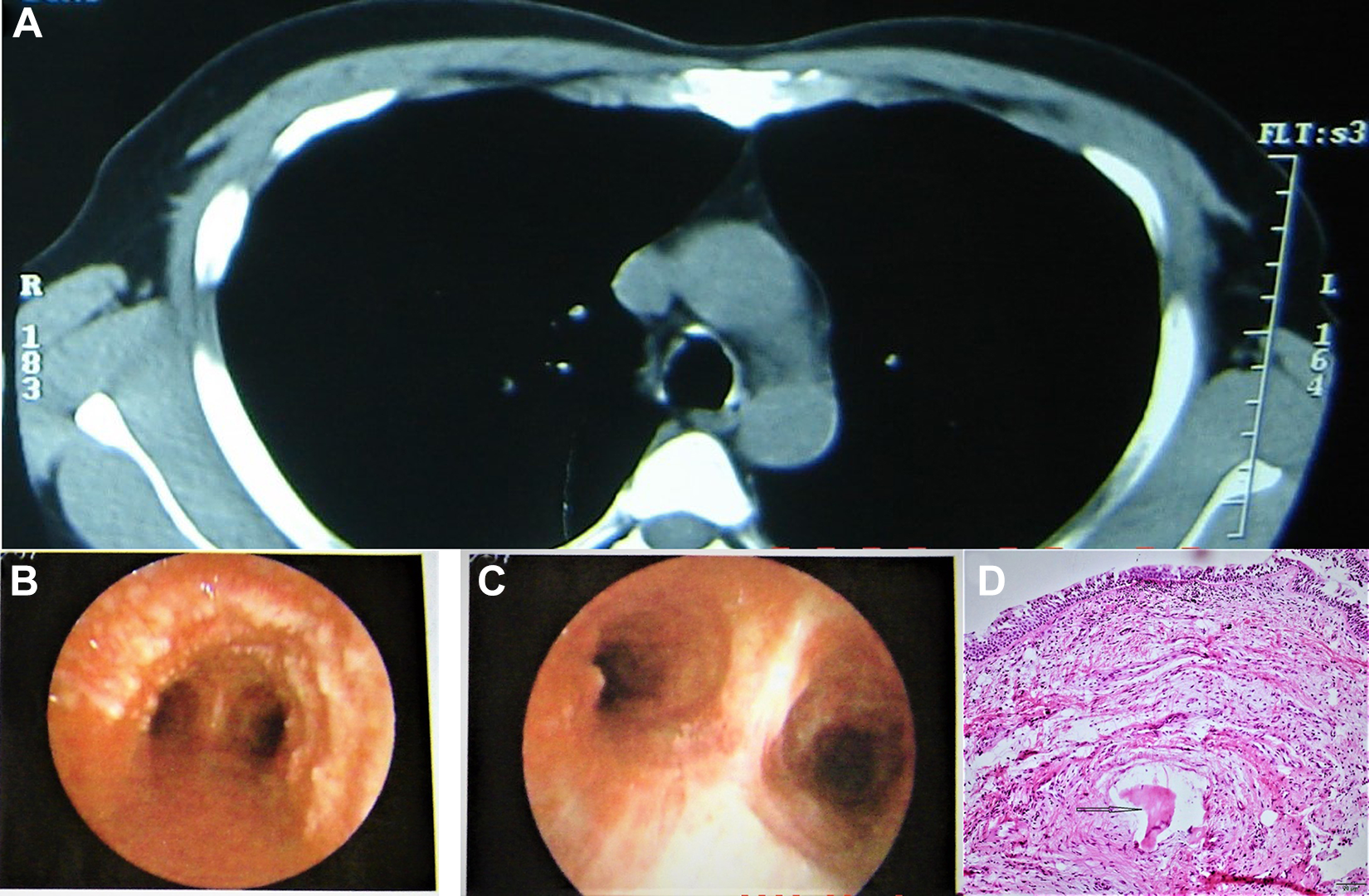
A 45-year-old man presented with recurrent productive cough and fever for 3 years, which had deteriorated in the past 2 months. A, Computed tomography scan showed anterolateral tracheal calcified nodules sparing the posterior wall. B and C, Bronchoscopy found diffuse smooth nodules distributed along the anterolateral tracheobronchial wall. D, Biopsy and histopathology identified bronchial mucosal epithelial hyperplasia with squamous and submucosal osseous metaplasia, which was consistent with the diagnosis of Tracheobronchopathia osteochondroplastica (TO).
Case 2
A 31-year-old man was admitted to our hospital for cough and fever for 1 month. The patient had been pathologically diagnosed with TO 7 years ago and was well managed with antibiotics. He had been smoking for 6 years with 5 cigarettes per day. Physical examination was unremarkable. Computed tomography scan showed unsmooth tracheal and bronchial walls and calcification in the cartilage (Figure 2A and B). Fibrobronchoscopy found airway mucosal congestion, edema, thickening, and gray-white nodules at the upper parts of the left and right bronchi (Figure 2C and D). The nodules had a hard texture and were difficult to biopsy, which was like the findings 7 years ago in 1999 (Figure 2E). The patient was well managed with aerosol inhalation of budesonide and amikacin for 14 days. The symptoms had been well controlled for several years.
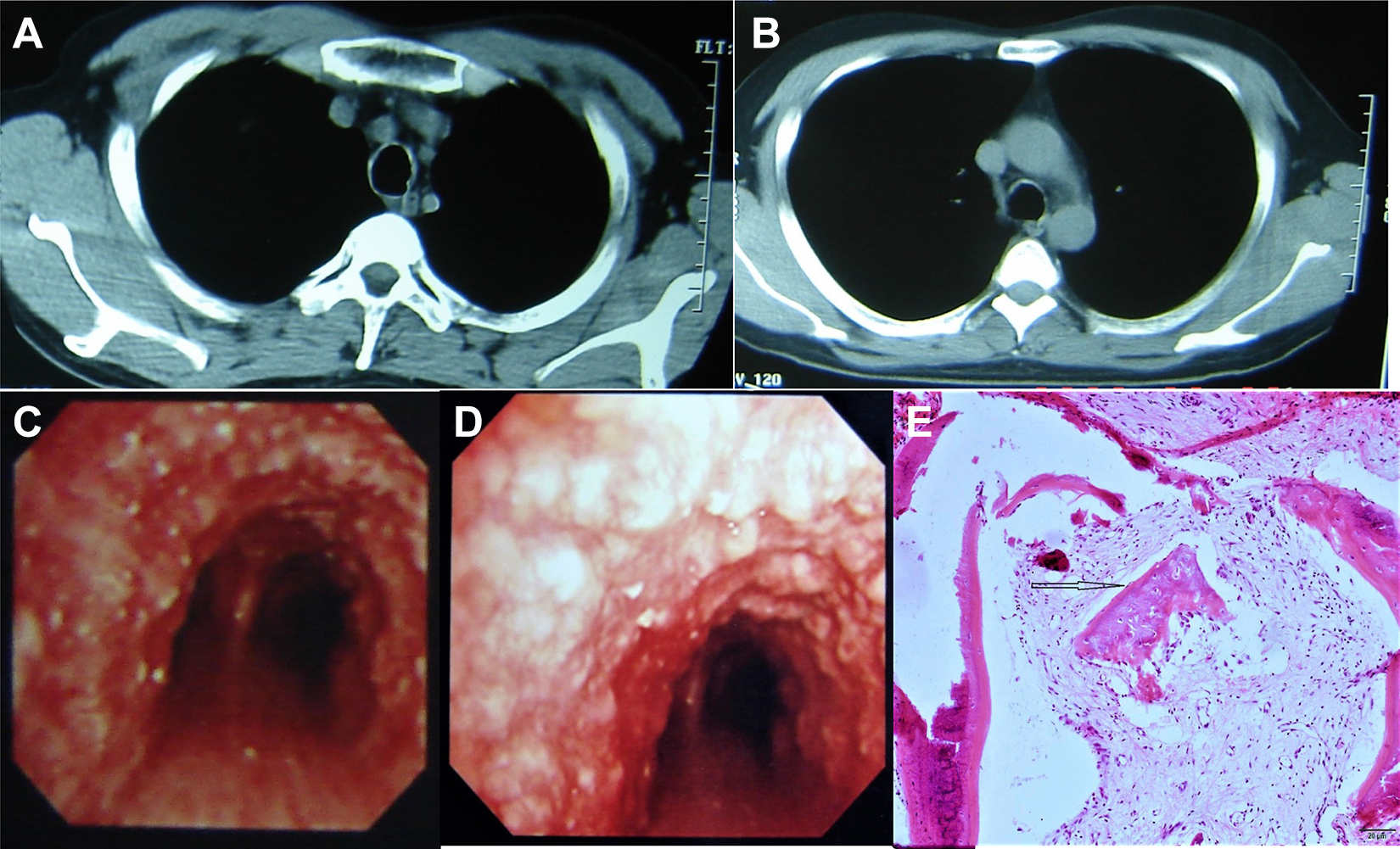
A 31-year-old man was admitted for cough and fever for 1 month. A and B, Computed tomography scan showed unsmooth tracheal and bronchial wall and calcification in the cartilage. C and D, Fibrobronchoscopy found airway mucosal congestion, edema, thickening, and gray-white nodules at the upper parts of the left and right bronchi. E, Pathology in 1999 showed bronchial epithelial proliferation and squamatization and submucosal osseous metaplasia.
Case 3
A 54-year-old nonsmoker man presented with productive cough and white sputum for 6 years. The symptoms had been well managed with antibiotics and symptomatic treatments. He used to have pulmonary tuberculosis (TB) and had been cured. Computed tomography scan showed nodulous elevation on the anterior airway wall (Figure 3A). Fibrobronchoscopy found multiple nodules on the anterolateral wall of the trachea, which had a hard text and were difficult to biopsy (Figure 3B). Pathological examination showed inflammatory infiltration and cartilage metaplasia in the bronchial mucosa (Figure 3C). The patient responded well to antibiotics and symptomatic treatments and the symptoms had been well controlled for several years.
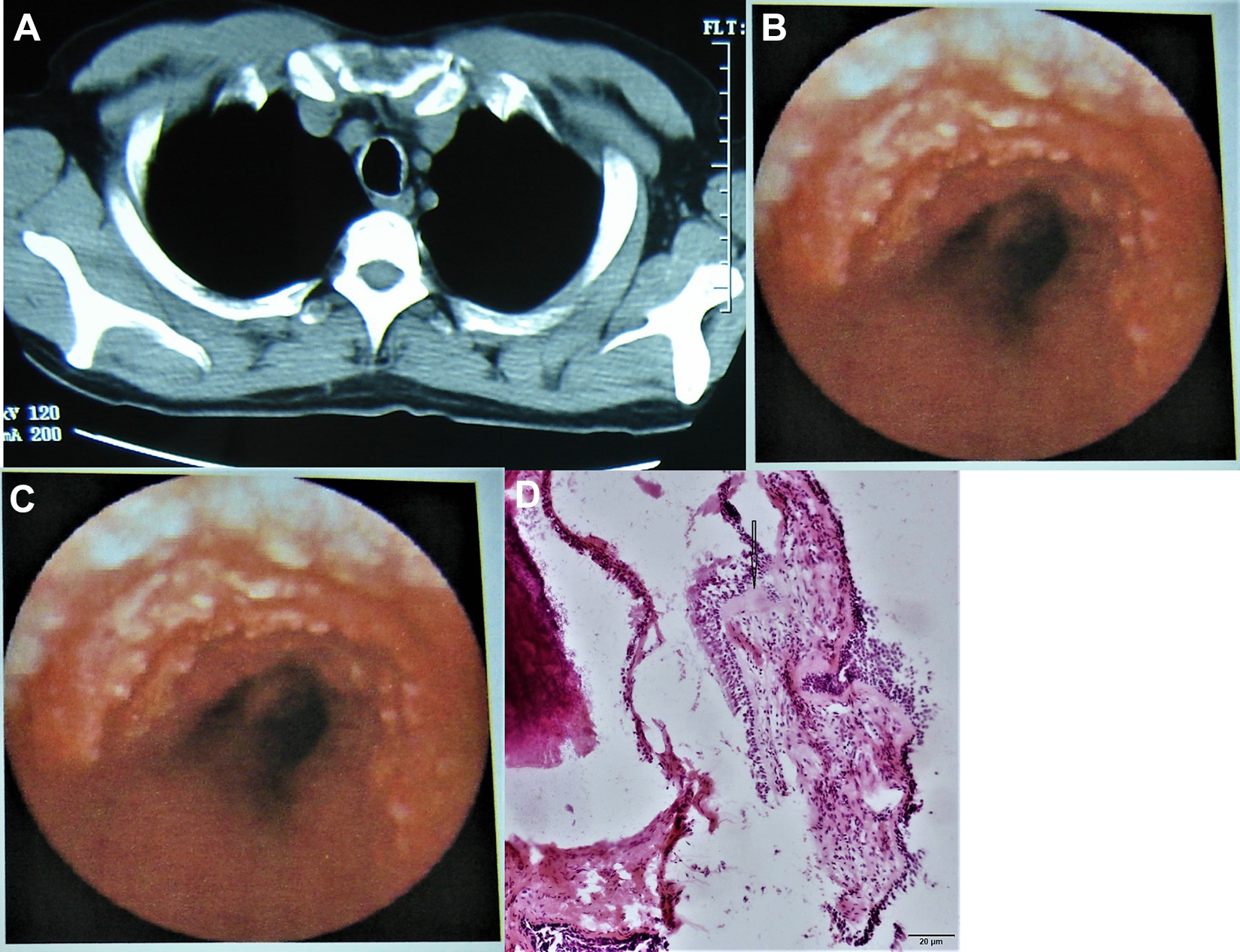
A 54-year-old nonsmoker man presented with productive cough with white sputum for 6 years. A, Computed tomography scan showed nodulous elevation on the anterior airway wall. B and C, Bronchoscopy found multiple nodules on the anterolateral wall of the trachea, which were hard and difficult to biopsy. D, Pathological examination showed inflammatory infiltration and cartilage metaplasia in the bronchial mucosa.
Case 4
A 48-year-old man presented with productive cough for 5 years. His symptoms had worsened with fever in the past 3 months. The patient had been smoking for 10 years with 20 cigarettes per day. Computed tomography showed unsmooth tracheal and bronchial walls with high-density nodulous elevation (Figure 4A). Fibrobronchoscopy found extensive pebble-like nodules in the cartilage of trachea and bronchi (Figure 4B). Pathological examination showed bronchial epithelial proliferation and squamatization and submucosal osseous metaplasia, which supported the diagnosis of TO (Figure 4C). His symptoms had been well controlled for several years with antibiotics and symptomatic treatments.
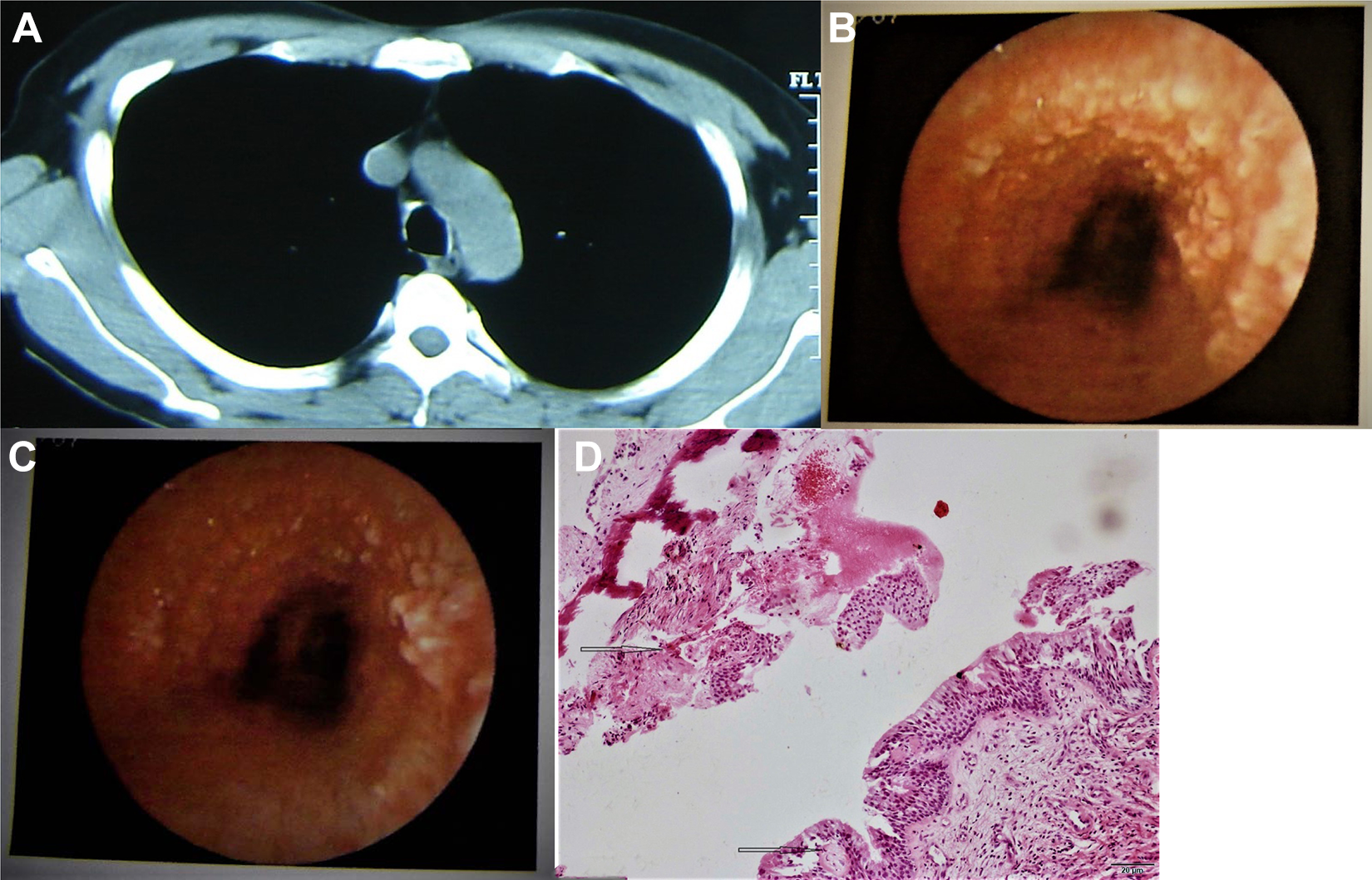
A 48-year-old man was admitted for productive cough for 5 years. A, Computed tomography showed unsmooth tracheal and bronchial walls with nodulous elevation, which was high in density. B and C, Bronchoscopy found extensive pebble-like nodules in the cartilage of trachea and bronchi. D, Pathological examination showed bronchial epithelial proliferation and squamatization and submucosal osseous metaplasia, which supported the diagnosis of Tracheobronchopathia osteochondroplastica (TO).
Case 5
A 62-year-old man was admitted for nonproductive cough and fever up to 39.5°C for 9 months. The symptoms were previously well managed with antibiotics and symptomatic treatments but had worsened in the past 2 weeks. The patient had been smoking for 25 years. Chest X-ray showed obliterative inflammation in the left upper lung and atelectasis. Fibrobronchoscopy found a nodulous mass blocking the opening of lingula of the left lung (Figure 5A). Suspecting that he had lung carcinoma, resection of the upper lobe of the left lung was performed. However, pathological examination showed nodulous proliferation of osseous and cartilage tissues, covered by mucosal epithelium, which was partially metaplastic (Figure 5B). The patient was finally diagnosed with TO and had been followed up for several years without disease progression.
A 62-year-old man was admitted for nonproductive cough and fever up to 39.5°C for 9 months. A and B, Bronchoscopy found a nodulous mass blocking the opening of lingula of the left lung. Suspecting that he had lung carcinoma, resection of the upper lobe of the left lung was performed. C, Pathological examination showed nodulous proliferation of osseous and cartilage tissues, covered by mucosal epithelium, which was partially metaplastic.
Discussion
Tracheobronchopathia osteochondroplastica is a rare disease of the large airways and is characterized by the development of submucosal cartilaginous and bony nodules. Tracheobronchopathia osteochondroplastica is more commonly seen in the elderly rather than children. The mean age of patients with TO is 51 years. 6,7 Using autopsy data and bronchoscopic findings, the estimated TO incidence is 2‰ to 7‰ 8,9 with a male to female ratio of 3:2. We searched the databases of PubMed, CNKI, VPCS, CSPD, and CBM and identified 64 papers in English or Chinese published during January 01, 1991, to December 31, 2018, reporting 130 Chinese TO cases. 4,5,8,10 -70 The reviewed 130 Chinese TO cases included 76 males and 54 females with a sex ratio of 2.81:2.
The specific mechanisms of TO are still not fully understood but are considered to be associated with bone morphogenetic protein 2, 71 chronic infection with mycobacteria or other bacteria, squamous metaplasia, metabolic disorder, and chemical or mechanic stimulations. 72,73 There is no conclusive evidence that smoking or genetics play a role in the development of TO. 2 The 5 patients treated at our hospital included 4 smokers and 1 nonsmoker. The reviewed 130 Chinese TO cases included 10 smokers and 17 nonsmokers and the rest patients were unclear in smoking history.
Tracheobronchopathia osteochondroplastica develops slowly and has no specific symptoms. The symptoms of TO are associated with disease involvement and tracheal obstruction. Among the 5 patients treated at our hospital, 1 patient had obstructive pneumonia. Among the reviewed 130 TO cases, 33 patients had obstructive inflammation and 3 patients had TB, which is speculated to be associated with airway stenosis.
Tracheobronchopathia osteochondroplastica can be easily misdiagnosed due to its nonspecific symptoms and the low awareness of this disease among clinicians. 6,7 Among the 130 reviewed Chinese TO cases,13 patients were misdiagnosed with TB, 5 patients with bronchitis or pneumonia, and 5 patients with lung carcinoma. Chest X-ray findings of TO are either unremarkable or nontypical chronic inflammation. On the contrary, CT scan is a useful imaging modality in diagnosing TO. Computed tomography may demonstrate characteristic 1 to 3 mm calcified nodules from the anterolateral wall of the trachea and main bronchi, which protrude into the airway lumen and cause tracheal wall thickening and airway stenosis. 6,7,72 In the 130 reviewed cases, 88.7% (86/97) of the patients with available CT data showed these characteristic multiple calcified projecting nodules, with or without tracheal wall thickening and lumen stenosis. The unique geographic distribution of TO nodules, typically sparing the posterior tracheal wall, is useful in distinguish TO from other nodular conditions affecting the large airways, such as TB, neoplastic diseases, endobronchial sarcoid, and amyloidosis. 74
Bronchoscopy and pathological examination are still the gold standard for diagnosing TO. The typical bronchoscopic findings of TO are multiple firm and glossy nodules protruding into the lumen of the distal two-thirds of trachea and proximal main bronchi, which may or may not cause airway stenosis and irregularity depending on the development of the disease. 72 Among the 5 patients treated at our hospital, only one patient had obstructive pneumonia. All the 130 reviewed cases showed consistent bronchoscopic findings of multiple firm and glossy nodules projecting into the airway lumen with intact mucosa. Biopsy and pathological examination usually find fragments of cartilaginous/osseous tissue in submucosa with normal mucosa tissue. Among the 130 reviewed cases, chronic inflammation and squamous intraepithelial metaplasia were described in 40 patients who had recurrent respiratory infections or other tracheobronchial complications. The hardness of the TO nodules resulted in biopsy failure in 3 patients of the reviewed 130 cases. Computed tomography and bronchoscopy should be sufficient for diagnostic imaging of TO. 75,76
Patients with TO are usually managed symptomatically using antibiotics, airway drainage, bronchodilators, and glucocorticoids. It has been reported that long-term inhalation of corticosteroids is effective in patients with early or mid-phase TO. 63 Bronchoscopic or surgical procedures are reserved for patients with severe airway stenosis and obstruction, 69 such as laser ablation, radio frequency ablation, bronchoscopic resection, stenting, and surgical removal. However, the safety and long-term efficacy of these procedures are still uncertain except laser ablation, which has shown good efficacy in patients with TO with airway stenosis. 7
Conclusions
Tracheobronchopathia osteochondroplastica is a rare benign disease with nonspecific symptoms and is difficult to diagnose. Computed tomography scan and bronchoscopy are useful in differentiating TO from other nodular respiratory illnesses. Patients with TO are usually managed symptomatically. Bronchoscopic or surgical procedures are reserved for patients with severe airway stenosis and obstruction. Awareness of this disease in clinicians is critical to make the correct diagnosis and avoid unnecessary treatments.
Footnotes
Authors’ Note
Written informed consent has been obtained from our treated patient for publication of this manuscript and any accompanying image.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.