
Abstract
Background: We aim to report a rare case of a herniated mastoid segment of the facial nerve that was accidently discovered during cochlear implantation surgery and how altering the surgery plan could achieve the implantation while preserving the nerve. Case presentation: A four-year-old girl presented with profound bilateral sensorineural hearing loss that did not completely resolve after 2 years of using hearing aids was scheduled for cochlear implantation surgery in the right ear. During surgery, a herniated mastoid segment of the facial nerve took an anterior course and obstructed the access to the round window. Conclusion: When a traditional posterior tympanotomy approach in cochlear implantation surgery is limited in cases of a herniated facial nerve, a tunnel created near the inferior part of the posterior wall of the auditory canal provided safe insertion of the electrode. It also permitted placement of a piece of fascia between the electrode and the facial nerve, therefore, protecting the facial nerve from electrical stimuli.
Background
Facial nerve herniation is an important anomaly that can be accidently discovered in middle ear surgery in general, and in cochlear implantation surgeries specifically. Injury and paralysis of the facial nerve are more likely to happen in an aberrant than in a normal nerve. 1 Another complication is stimulating the facial nerve, which happens in approximately 5.8% of cochlear implantation surgeries. 2 About 60% of congenital fallopian canal dehiscence are reported to affect the tympanic portion above the oval window but rarely found at the mastoid portion. 3 Hereby, we aim to report a case of a herniated mastoid segment of the facial nerve that was accidently discovered during cochlear implantation surgery and how altering the surgery plan could achieve the implantation while preserving the nerve.
Case Presentation
A four-year-old girl was admitted to our clinic because of congenital sensorineural hearing loss that was first discovered at the age of 2 years and did not completely resolve after 2 years of using hearing aids. She was a full-term baby, without any significant medical history. Her family history was also clear of any related conditions. Her auditory brainstem response test (ABR) did not detect the fifth wave till 90 dB in both ears. HRCT showed normal middle ear, cochlea, internal meatus, and mastoid, but the facial nerve findings were unremarkable. Based on these results, cochlear implantation surgery for the right ear was scheduled.
During surgery, after a standard transmastoid posterior tympanotomy approach, a pale pearl-white soft cord appeared. It corresponded with the mastoid segment of the facial nerve without its bonny canal. The nerve took an anterior course and obstructed the access to the round window where electrode insertion was planned. To maximize vision, the facial recess was widened using a diamond burr with a long-tapered stem. Adequate irrigation was employed, the operating table and the microscope were adjusted, and a slight posterior retraction of the facial nerve was done until the surgeon had enough exposure to perform cochleostomy, anterior and inferior to the round window. Then, the surgeon created a tunnel through the mastoid cavity that ended in the tympanic cavity. The tunnel was near the inferior part of the posterior wall of the auditory canal (Figure 1). A Med-El straight electrode was later dropped directly into the cochleostomy. A pre–insertion photograph showing that after widening the facialrecess, the anteriorly misplaced dehiscent mastoid segment of the facial nerve was obstructing the access to the round window;The normal place of electrode insertion (blue arrow).The alternative place for insertion (green line) with the artificial tunnel near the inferior border of the posterior wall of the auditory canal (blue cross).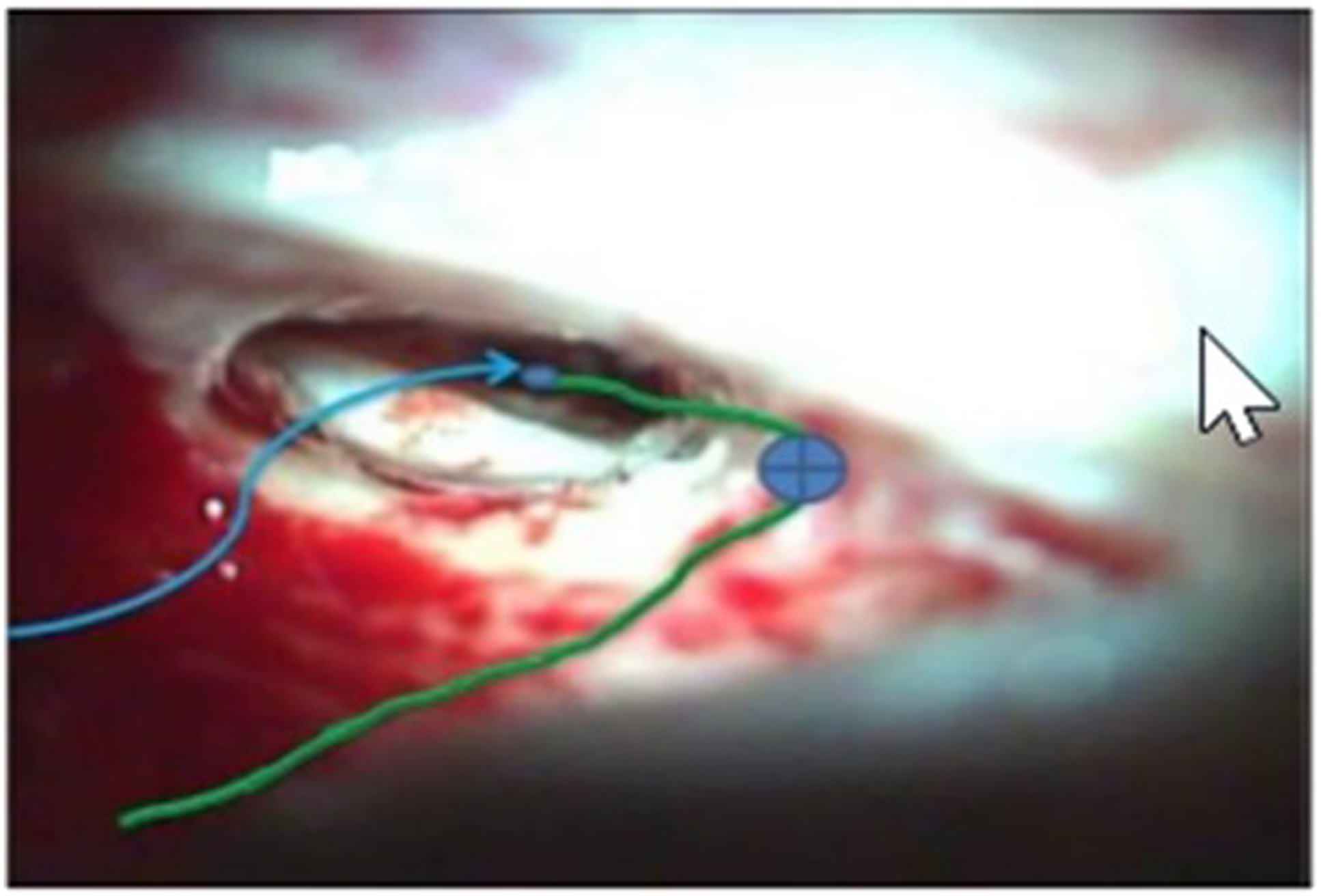
Before closure, an inspection of the middle ear mucosa and the ossicular chain revealed a normal appearance, and a piece of temporal fascia was placed between the electrode and the facial nerve (Figure 2). During the operation, no injury to the facial nerve occurred, and the tympanic nerve remained intact. Auditory response telemetry (ART) confirmed total activation of all channels. The patient’s postoperative course was uneventful, and the follow-up assessment of facial nerve function was normal. No stimulation was reported from the time of activation of the external process 6 weeks after the implantation till the 1-year follow-up examination. The free field audiometry with cochlear implant showed a threshold of 40-50 dB after 6 months of surgery. A post-insertion photograph showing the beginning of the tunnel (blue arrowhead). The end of the tunnel (blue arrow). The fascia used to fill the space between the electrode and the facial nerve (star).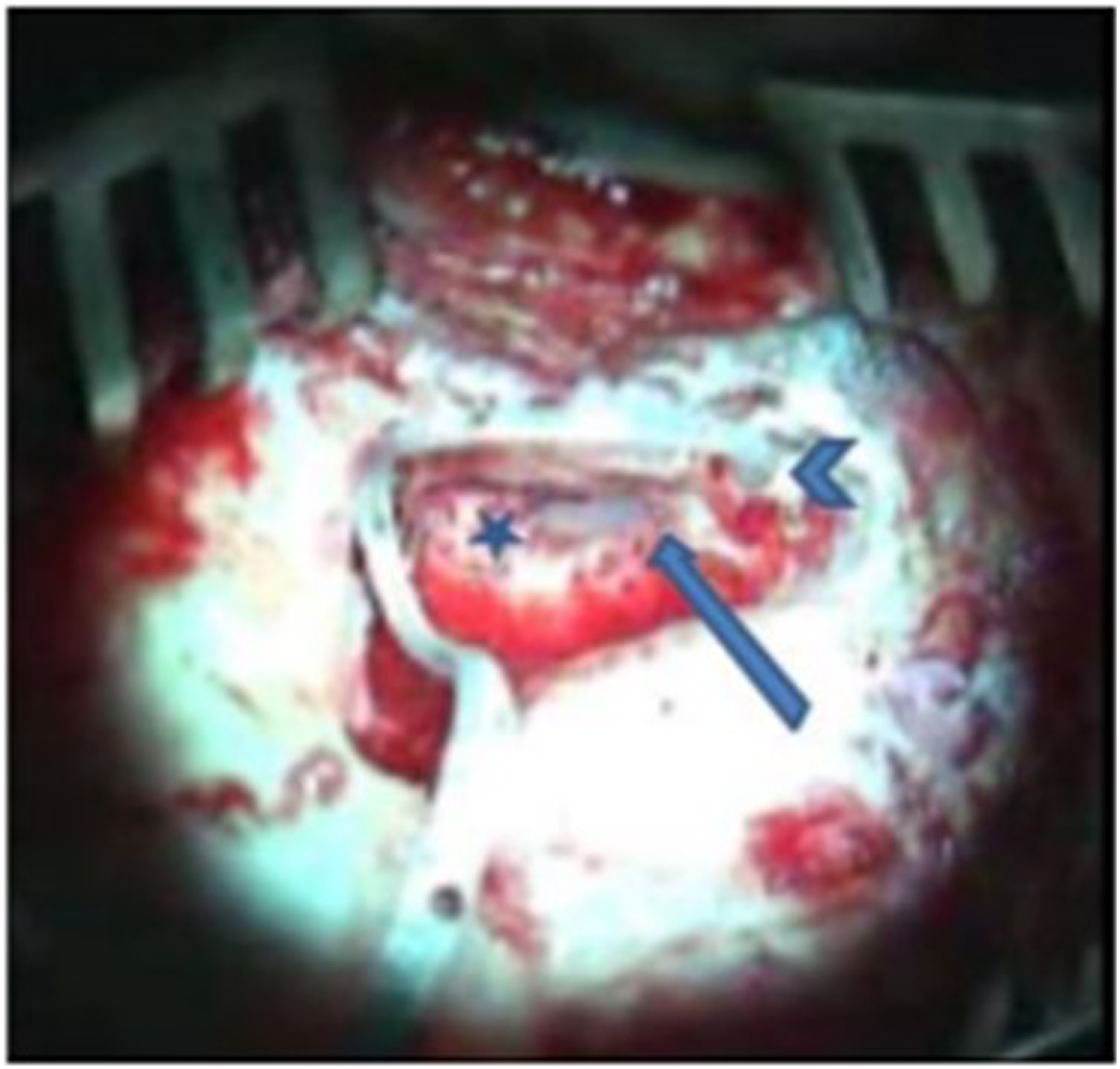
Discussion
Failure of the facial canal closure in the developmental period results in congenital canal dehiscence with only mucoperiosteum covering the facial nerve, and the absent bony cover can further lead to protrusion of the facial nerve from its canal and normal course. 4 Some reports showed that an aberrant facial nerve is found in 16-17% of ears with malformation,5,6 whereas the incidence of an aberrated facial nerve in normal ears is approximately 0.3%. 7 This deformity rarely affects the mastoid segment, 3 making our case presentation even rarer. Continuation with the standard posterior tympanotomy approach carried an increased risk of damage to the facial nerve. Therefore, the creation of a tunnel near the inferior part of the posterior wall of the auditory canal helped to preserve important structures including the aberrant facial nerve and the posterior meatal wall.
A few approaches have been reported in similar settings. Miyamoto et al. inserted the electrode through the ear canal and drilled a groove through the posterior wall of the bony canal to avoid injury to a laterally positioned facial nerve, 8 while Rizk et al. utilized a retrofacial approach in a malformed ear. 9 The tunnel in our approach did not only assure safe electrode insertion but also helped to preserve a space between the facial nerve and the active channels of the electrode, which was filled with fascia. Therefore, this approach also evaded the undesirable results of nerve stimulation.
On the other hand, Mankekar et al. attempted a middle fossa approach in a case with only one functional facial nerve, which was anteriorly displaced on the promontory over the round window, 10 and others followed a suprameatal approach. 11 While both approaches would be valid alternatives to the technique followed in our case, they provide only limited direct visualization, keep the surgeon in close proximity to vital structures, and need highly trained and experienced hands.
Computed tomography (CT) scans provide an important diagnostic tool in demonstrating temporal bone disorders. However, it still has limitations regarding the detection of the dehiscence of the facial canal which can occasionally be unclear or dismissed. In such surgeries, the use of facial nerve monitor throughout the operation can help minimize the risk of injuring it. 12
Conclusion
When a traditional posterior tympanotomy approach in cochlear implantation surgery is limited in cases of a herniated facial nerve, a tunnel created near the inferior part of the posterior wall of the auditory canal can be a feasible alternative.
Footnotes
Authors contributions
All authors read and approved the final manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics Approval
Consent for publication: A signed informed consent was obtained from the parents of the patient to publish this report.