
Abstract
Objectives
The lesion distribution of juvenile-onset recurrent respiratory papillomatosis (JORRP) during first-time surgery has been rarely reported. The purpose of this study was to describe the anatomical distribution of papilloma across 25 Derkay sites during initial surgery and to assess the impact of the lesion distribution on disease severity.
Methods
Surgical videos and medical records of 106 patients with JORRP (27 aggressive and 79 nonaggressive cases) were retrospectively reviewed. Lesion locations were recorded using Derkay anatomical sites. Logistic regression was used to analyze the effect of the lesion distribution on disease severity.
Results
Among the 106 patients, the true vocal cords (90.6% left, 84.0% right) were the most frequently involved site, followed by the false vocal cords (39.6% left, 35.8% right) and the anterior commissure (26.4%). Two patients (1.9%) had tracheal involvement. Patients with false vocal cord involvement (odds ratio [OR] = 3.425, 95% confidence interval [CI] [1.285, 9.132], P = .014) and a younger age at diagnosis (OR = .698, 95% CI [.539, .905], P = .007) were more likely to require more than 4 procedures in the year following first-time surgery.
Conclusions
Lesions were most common on the true vocal cords. False vocal cord involvement and a younger age at diagnosis were risk factors for disease severity.
Keywords
Introduction
Recurrent respiratory papillomatosis (RRP) is the most common benign neoplasm of the larynx and is predominantly caused by human papillomavirus (HPV) types 6 and 11. 1 It has been separated into juvenile-onset RRP (JORRP) and adult-onset RRP (AORRP) by an age of diagnosis of 18 years. 2 -4 Juvenile-onset RRP treatment has been a medical challenge because of its unpredictable clinical course, with a high frequency of recurrence, and dissemination throughout the entire aerodigestive tract. 5,6 These features may correlate with the initial lesion distribution. 7,8 To date, however, few published reports have focused on this topic.
Kashima et al. summarized the lesion distributions of more than 400 RRP patients in 9 published studies and concluded that the lesions were mainly distributed at the squamo-ciliary junction. 6 This study is of great significance for understanding the distribution of lesions in patients with RRP. However, some debatable concerns remain. First, the subjects included patients of any age despite differences in the mode of HPV infection, risk factors, and disease severity between adults and children, 9 which may result in differences in lesion distributions. Second, the study includes patients who had undergone surgical interventions, which affected the distribution of lesions; thus, the results cannot reflect the actual natural lesion distribution.
Benedict et al. described the lesion distributions of 83 previously untreated patients with AORRP and reported that membranous vocal folds were most frequently involved. 10 Moreddu et al. analyzed the effect of the lesion distribution in the 3 regions of the larynx on disease severity at first endoscopy; however, the lesion distribution was not discussed in detail. 7 Yao et al. described the anatomical distribution of JORRP in different periods, but only described the distribution in the larynx, but did not describe the extra-laryngeal sites. 11 Thus far, the lesion distribution in patients with JORRP at first-time surgery is still unknown. The Derkay staging system is widely used to stage the disease. 12
Therefore, this study aimed to describe the lesion distribution across 25 Derkay anatomical sites in patients with JORRP at initial surgery. This study also aimed to analyze the effect of the lesion distribution on disease severity.
Patients and Methods
Subjects
One hundred six patients with JORRP who underwent initial surgery from January 1, 2010, to August 30, 2019, by senior ear, nose, and throat (ENT) surgeons at our institution, were retrospectively reviewed. The inclusion criteria were as follows: (1) age at diagnosis < 18 years old; (2) initial operation at Beijing TongRen Hospital; (3) a histopathologically confirmed diagnosis of respiratory papillomatosis lesion; and (4) a follow-up period exceeding 1 year after initial surgery. The exclusion criteria were as follows: (1) patients with papillomas affecting only the oral cavity or pharynx and (2) patients diagnosed with squamous epithelial papillary hyperplasia. The study protocol was approved by the ethics committee of Beijing Tongren Hospital, Capital Medical University in China (TRECKY2021-015).
Data Collection
We collected information from medical records and surgical videos. Variables included sex, age at diagnosis, symptom duration before diagnosis, the locations of papillomas involved in 25 anatomical sites of the aerodigestive tract according to the Derkay staging system, 13 and the total number of procedures performed 1 year after the first surgery. The locations of papillomas were evaluated by 2 ENT surgeons (Yang Xiao and Lijing Ma).
Derkay Anatomical Sites
The Derkay staging system includes the following 25 subsites: the lingual surface of the epiglottis; laryngeal surface of the epiglottis; left aryepiglottic fold; right aryepiglottic fold; left false vocal cords; right false vocal cords; left true vocal cords; right true vocal cords; left arytenoids; right arytenoids; anterior commissure; posterior commissure; subglottic region; trachea, including the upper 1/3, middle 1/3, and lower 1/3; left bronchi; right bronchi; tracheotomy stoma; nose; palate; pharynx; esophagus; and lungs. 13 The score for each site was 1 or 0, indicating the presence of absence of a lesion at this site, respectively.
Inter-Rater Reliability
Two ENT surgeons analyzed the surgical videos, and each surgeon examined half of the total surgical videos. To ensure consistency between the 2 surgeons, 5 randomly selected surgical videos were analyzed by both surgeons, and Cohen’s kappa coefficient was calculated.
Disease Severity
According to the total number of surgical procedures performed during the first postoperative year, JORRP was classified as aggressive or nonaggressive.3 The disease was considered aggressive if the total number of surgeries was ≥4; otherwise, it was considered nonaggressive.
Statistical Analysis
The chi-square or Fisher’s exact test was used to compare differences in proportions. The Mann–Whitney U test was used to compare nonnormally distributed continuous variables. Univariate and multivariate logistic regression analyses were used to analyze risk factors for disease severity. All statistical analyses were performed using SPSS 26.0 (IBM Corp, Armonk, NY), and P < .05 was considered statistically significant.
Results
Among the 106 patients, 64 (60.4%) were male, and 42 (39.6%) were female. The sex distribution showed a slight tendency in favor of male children. The median age at diagnosis was 2.8 years (range, .4 to 17.6 years). The symptom duration before diagnosis ranged from .6 to 146.3 months, with a median time of 6.2 months. The median number of surgeries followed up 1 year after surgery was 2 (range, 1–11). Among the 106 patients, 27 (25.5%) had aggressive disease, and 79 (74.5%) had nonaggressive disease. The age at diagnosis was significantly different (P = .001), whereas no significant difference in sex (P = .553) or symptom duration before diagnosis (P = .189) was found between the two groups.
Inter-Rater Reliability
Cohen’s kappa coefficient of inter-rater reliability between the two surgeons was .97 (P < .001), which indicated strong agreement.
Distribution of Lesions
The Lesion Distribution of JORRP and the Difference Between Aggressive and Nonaggressive Groups.
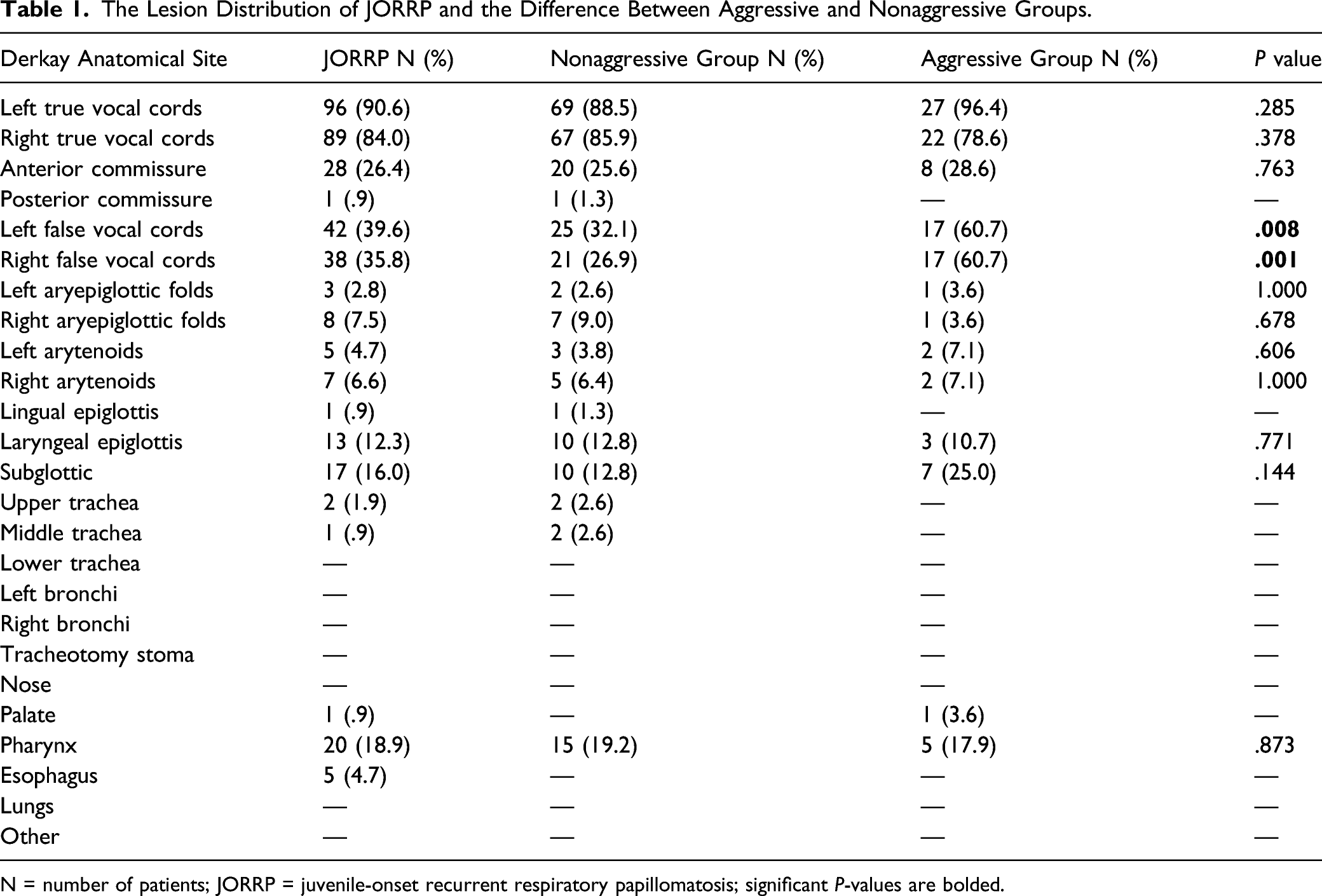
N = number of patients; JORRP = juvenile-onset recurrent respiratory papillomatosis; significant P-values are bolded.
Twenty patients (18.9%) presented with pharyngeal lesions, including 6 patients with piriform fossa involvement (5.7%), 4 with posterior hypopharyngeal wall involvement (4.2%), 3 with uvula involvement (3.2%), 3 with soft palate involvement (3.2%), 3 with tonsil involvement (3.2%), 3 with posterior ring area involvement (3.2%), 3 with base of the tongue involvement (3.2%), 2 with posterior oropharyngeal wall involvement (2.1%), and 1 with palatoglossal arch involvement (1.0%).
The trachea was involved in 2 patients (1.9%) at the first surgery. One patient presented with hoarseness when he was 4.6 years of age, and he was diagnosed with RRP 5 months later. Multiple papilloma sites were found in the larynx, bilateral tonsils, base of the tongue, and posterior wall of the pharynx. Another patient was diagnosed with JORRP at the age of 11 years, and papilloma was observed on the right vocal cords, right arytenoids, subglottic region, and trachea at the first surgery. In the following 8 years, she underwent 4 surgeries.
Lesion Distribution Between the Aggressive and Nonaggressive Groups
No significant differences in the distribution of lesions on the true vocal cords, anterior commissure, subglottic, aryepiglottic fold, arytenoids, or pharynx were found between the two groups. However, false vocal cord involvement was higher in patients with aggressive disease than in those with nonaggressive disease (P < .05) (Table 1).
Influence of the Lesion Distribution on Disease Severity
Logistic Regression Model for Disease Severity.
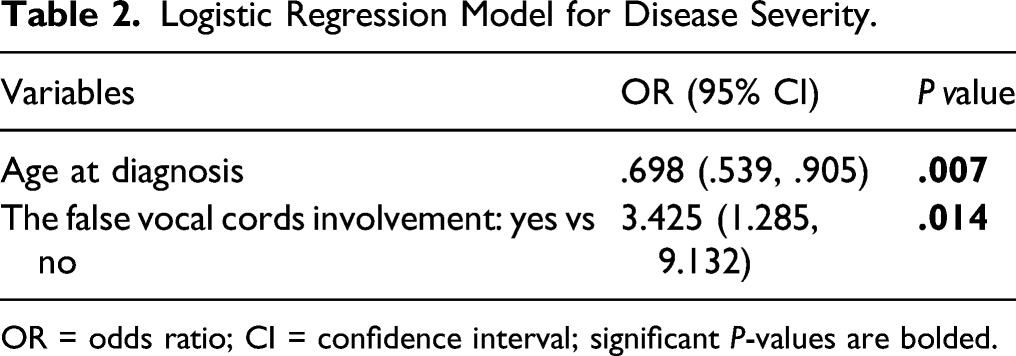
OR = odds ratio; CI = confidence interval; significant P-values are bolded.
Discussion
Recurrence and poor disease control are major obstacles to successful JORRP treatment, particularly because these patients require multiple procedures, which adversely affect patients’ and their families’ quality of life. 14 Lesion distribution characteristics are closely related to recurrence and may affect the clinical course of the disease. 7,15 However, many previous studies on lesion descriptions were performed decades ago, only tangentially address this topic, and fail to capture the natural lesion distribution. 8 Therefore, investigating the distribution of initial JORRP lesions and its clinical relevance are imperative.
In the present study, we found that the true vocal cords were the most often involved site, which is consistent with the results of previous studies. 10,11,16 Although the exact mechanism is still unknown, two possible explanations can be considered. First, papilloma tends to occur at the squamo-ciliary junction, and the upper and lower surfaces of the true vocal cords have this histological feature. 6 Second, the glottis is the narrowest part of the upper airway and is impacted by high airflow pressure, which can easily compromise the epithelial barrier function of the true vocal cords when coupled with microtrauma from vocalization. 17,18
The second most common site was the false vocal cords, which is also consistent with previous studies. 6,18 Anatomically, the false vocal cords are adjacent to the true vocal cords, and lesions easily spread from the true vocal cords to the false vocal cords. In addition, false vocal cord involvement may be related to ventricular dysphonia, 19 which is a compensatory mechanism for glottic dysfunction. Lesions of the true vocal cords cause glottic incompetence, and the false vocal cords compensate for pronunciation, easily resulting in microtrauma of the false vocal cords and inducing papilloma growth. Aaltonen et al reported a case of RRP in which lesion progression confirmed this view; the lesions were originally located on the true vocal cords. Due to scarring on the vocal cords after multiple surgeries, the patient used the false vocal cords for pronunciation. Later, papilloma was found on the false vocal cords. 20
Our further study demonstrated that patients with false vocal cord involvement at initial surgery were 3.4 times more likely to have aggressive disease than those without false vocal cord involvement, indicating that false vocal cord involvement might be a useful biomarker for aggressive disease. This is the first report of a relationship between false vocal cord involvement and aggressive disease in JORRP. The exact cause is still unknown and requires further study. However, this study provides some guidance for clinicians to assess disease severity. Moreover, the present study also confirmed that age at diagnosis is a known risk factor for disease severity, 21 which may be related to the smaller airway and poor immune function in younger patients. Therefore, patients with JORRP who are younger at diagnosis and whose lesions involve the false vocal cords at initial surgery are more likely to have more severe disease.
Quiney et al. reported that pharyngeal involvement was less than 1% and was associated with disease severity. 8 However, in this study, the pharyngeal involvement rate was 18.9%, the lesions were mainly located in the oropharynx and hypopharynx, and pharyngeal involvement was not related to disease severity. Considering the relatively high incidence of pharyngeal involvement, we recommend that the pharynx warrants greater attention during the first operation to avoid missing papilloma lesions. Earlier studies suggested that the epiglottis was also a more frequently involved anatomical site. 6 In this study, the involvement rates of the laryngeal surface and lingual surface of the epiglottis were 12.3% and .9%, respectively. The lesions were mainly located on the laryngeal surface of the epiglottis, which was related to the anatomical characteristics of the squamo-ciliary junction in the middle of the epiglottic laryngeal surface. 6
Previously reported tracheal involvement rates range from 5% to 31% 22,23 ; however, in this study, the tracheal involvement rate was 1.9%, which was significantly lower than those in previous reports. Since tracheotomy is the primary cause of tracheal involvement, we and others have previously reported that the tracheal involvement rate in patients with tracheotomy ranges from 73.5% to 80%. 24,25 The tracheal involvement rate was low in this study because all patients had primary disease and did not undergo tracheotomy. Distal airway involvement has been used as a marker of aggressive disease because lesions in the distal airway often indicate more severe disease. 26 However, since the purpose of this study was to identify the effect of the lesion distribution on disease severity, tracheal involvement was not directly classified as aggressive. The present study showed that the total number of operations performed on the two patients with tracheal involvement was fewer than 4 in the first year after initial surgery. Due to the small number of patients, whether tracheal involvement corresponded to aggressive disease was impossible to evaluate from a statistical perspective; large-sample data are needed for further confirmation.
The authors recognized that this study had significant limitations. First, this was a retrospective study with inherent difficulties in quality data collection. Second, although no effective adjuvant therapy is available, some patients were given adjuvant medication, which may influence the total number of surgeries. Therefore, additional multicentre prospective studies are needed to validate our findings.
Conclusion
Lesions in patients with JORRP were most frequently observed on the true vocal cords, followed by the false vocal cords, anterior commissure, and pharynx. False vocal cord involvement and a younger age at diagnosis were risk factors for disease severity.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Pediatric Special Project of the Pediatric Subject Collaborative Development Center of Beijing Municipal Hospital Administration under Grant Number XTCX201823 and the Beijing Administration of Traditional Chinese Medicine under Grant Number JJ-2020-17.