
Abstract
Introduction
In the last years, there have been several reports published about “another” ethmoidal artery different from the anterior and posterior ethmoidal arteries. The authors refer to it in different terms, such as supernumerary, tertiary, intermediate, accessory, or middle ethmoidal artery.1,2 The European position paper on the anatomical terminology of the internal nose and paranasal sinuses suggests the term of accessory ethmoidal artery (AcEA) and it refers a prevalence of 40% according to the Lang J’s study.3,4
However, neither the international anatomical terminology nor the classical anatomy books make reference to AcEA,5-8 which creates serious doubts about its existence and if so about its true anatomical origin. The different exploratory methods and the various specimens used in order to identify the AcEA can explain this controversy.
In addition, the anterior ethmoidal arteries are usually mentioned as possible cause of refractory epistaxis when the sphenopalatine artery ligature fails. These arteries are responsible for the nose bleeding in approximately 20% of cases.1,2 Exceptional intractable epistaxis can involve other different arteries. These reports mention posterior ethmoidal artery, the palatovaginal artery, or branches from facial artery as possible causes.9-11Most of these studies note the possibility of cauterization of the AcEA in order to control the epistaxis. The aim of our study is to calculate the prevalence of the AcEA in endonasal endoscopic cadaver dissections and to identify its intraorbital origin.
Material and Methods
From October 2018 to October 2020, thirty-four nasal dissections were performed in seventeen adult cadaveric heads with no history of ENT pathology or surgery. The specimens belonged to the voluntary body donation program of the Anatomy Departments from the University of Girona and the Autonomous University of Barcelona, which follows the legal procedures and ethical framework governing body donation in our country.
Eight cadaveric specimens had been fixed with Cambridge solution, whereas in the other 9 specimens, we used the modified Larsen solution. All cases had been previously injected with colored latex into the internal and external carotid system.
Cadaver dissection following endoscopic endonasal approach was performed using 0° and 45° rigid endoscope. We performed an uncinectomy with antero-posterior ethmoidectomy and sphenoidectomy in both nasal cavities, in order to have a complete view of the ethmoidal roof. We defined anterior ethmoidal canal (AEC) as the most anterior canal in the anterior ethmoidal roof located posterior to the anterior wall of the bulla. The posterior ethmoidal canal (PEC) was defined as the most posterior canal in the posterior ethmoidal roof in front of the most superior aspect of the anterior wall of the sphenoid sinus. The accessory ethmoidal canal (AcEC) was defined when we found a canal between the anterior and posterior canals. Then, we removed the bony canal and the lamina papiracea to verify the injected vessel and to confirm the vascular structure inside the canal. Finally, we removed the periorbita and we dissected the intraorbital space until to identify the ophthalmic artery and the origin of the ethmoidal arteries.
Ethics Statement
The Institutional Review Board of Santa Creu i Sant Pau Hospital approved all protocols and procedures used.
Results
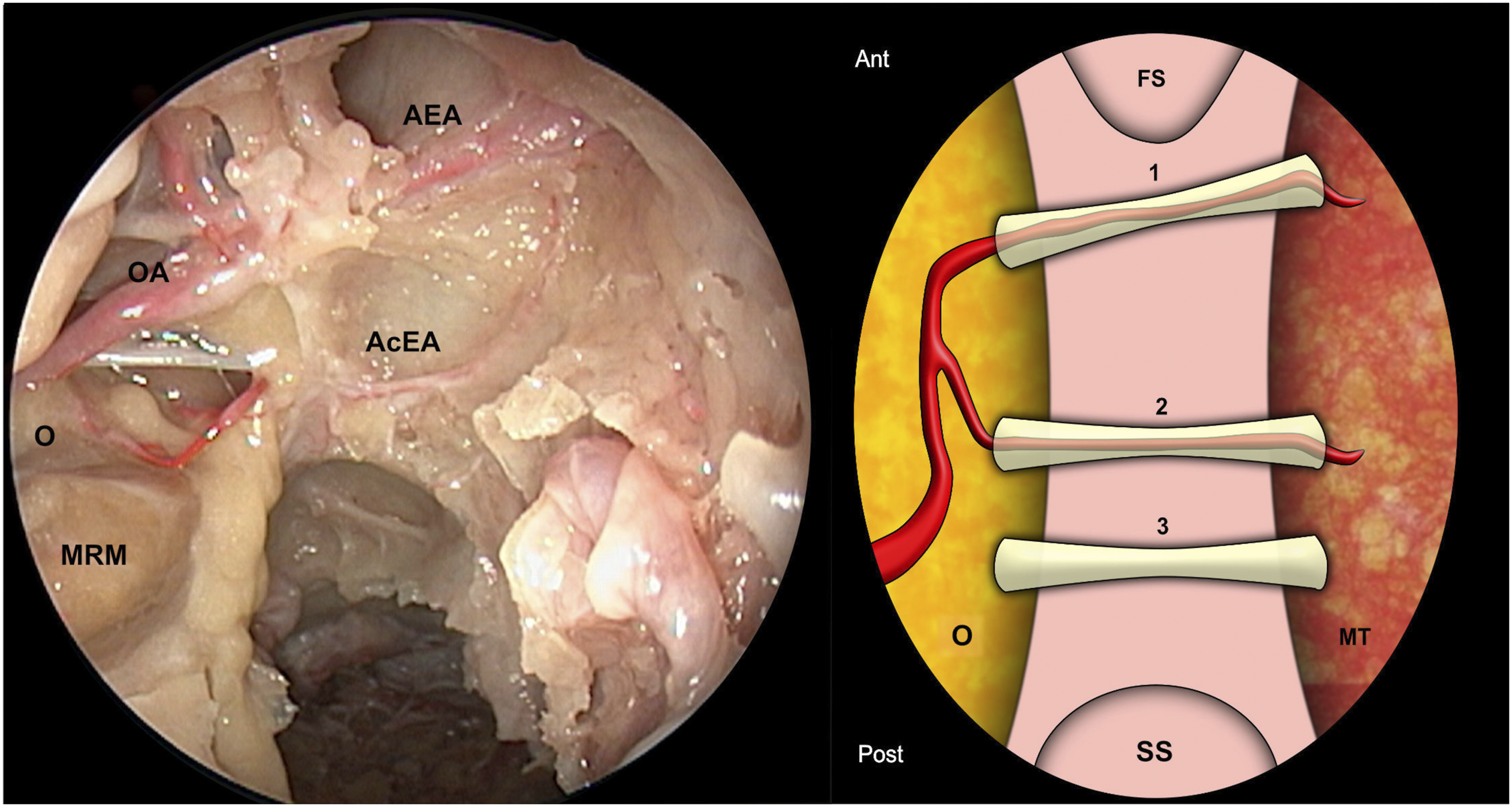
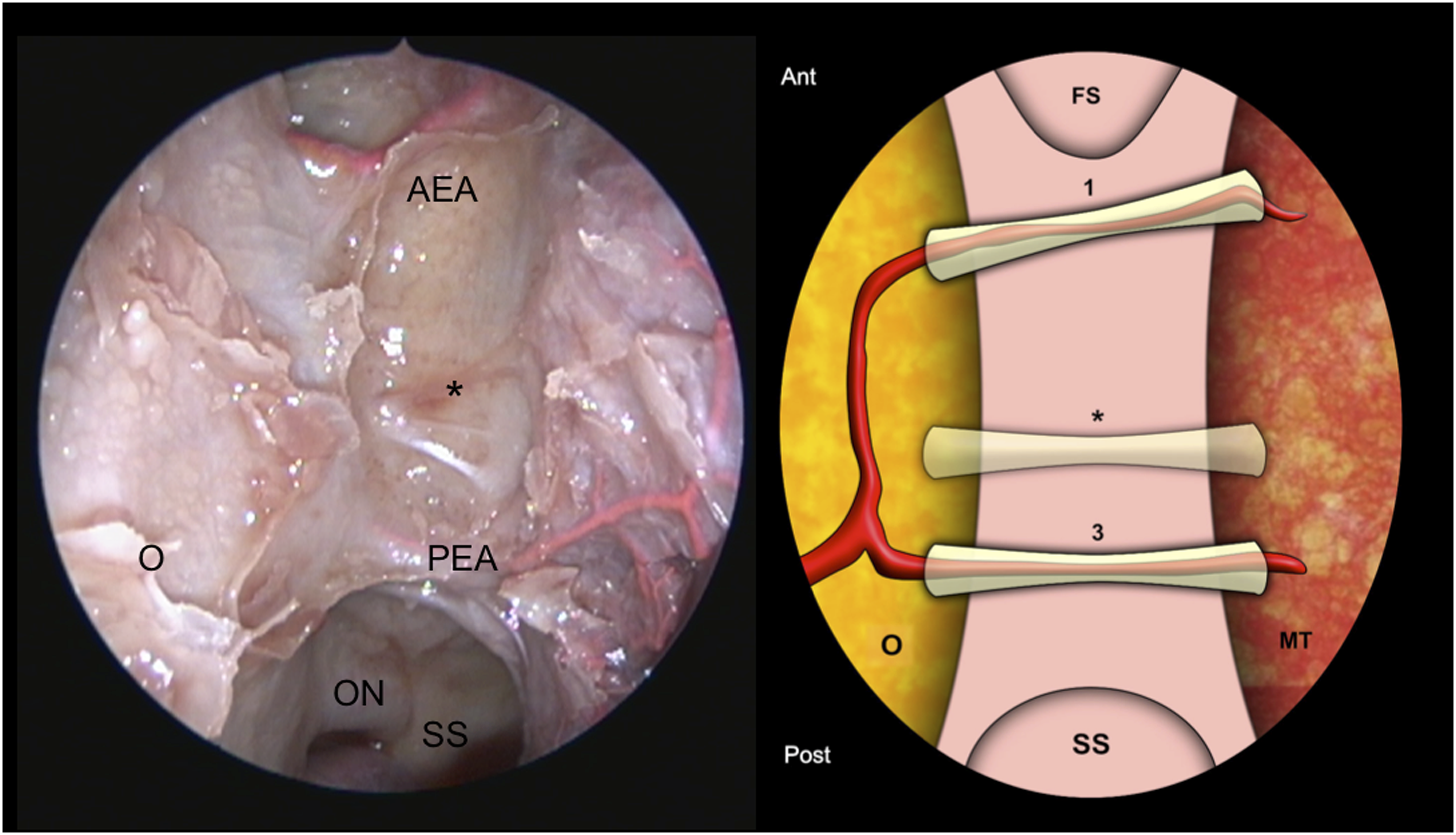
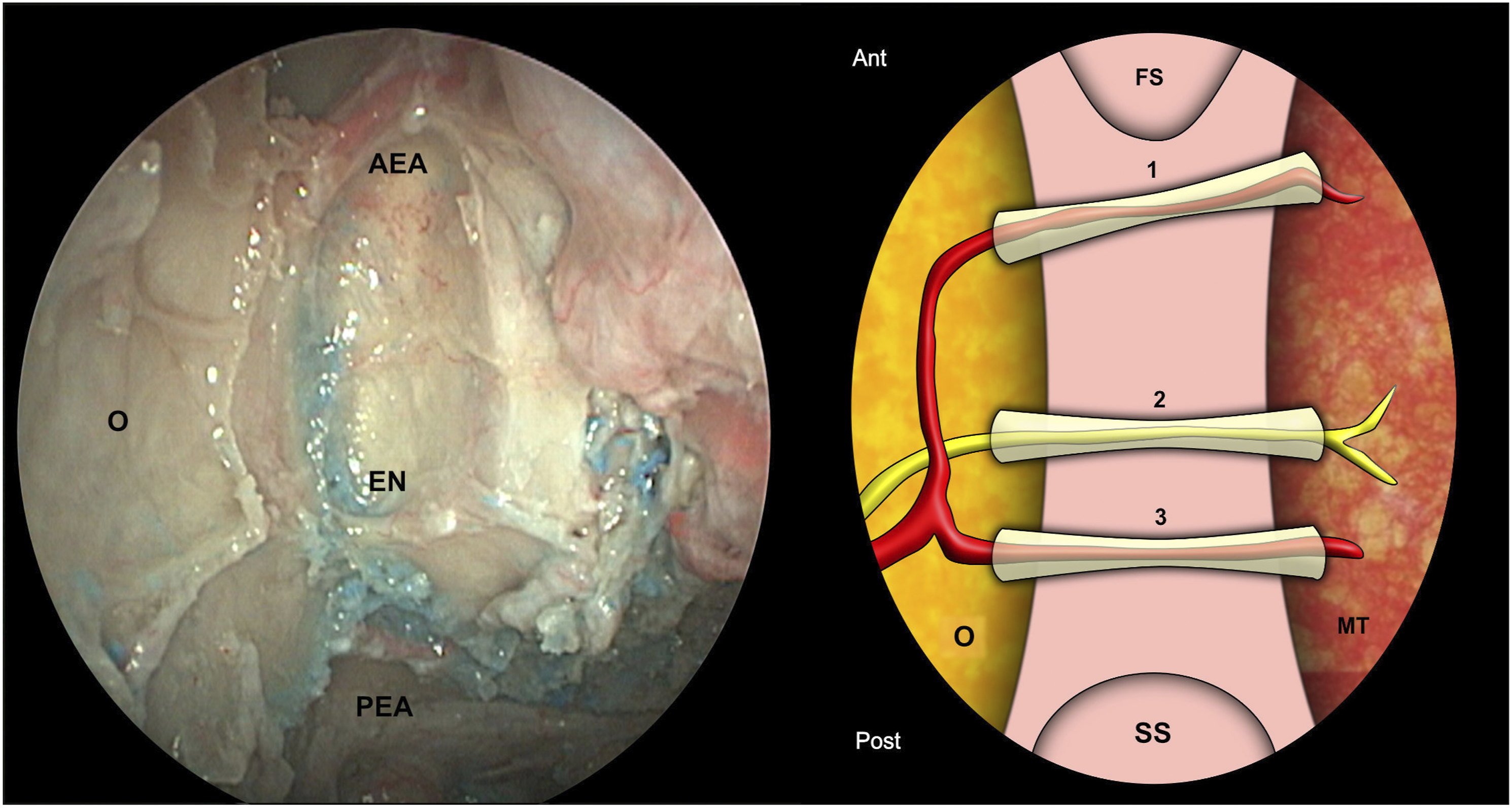
We found the AEC and PEC in 100% of nasal cavities (34/34). We identified 4 AcEC in the 34 nasal fossae dissected (12%) (Figure 1). All AEC contained an arterial vessel. The AcEC contained an arterial vascular structure in 2 cases, a neural structure in other specimen, and in the fourth case no structure could be verified (Figures 2–5). No case was bilateral. In 32 of 34 nasal cavities, the PEC contained an artery and only in 2 cases the PEC did not contain any vascular structure. In these specimens, we observed that the AcEC with an arterial vessel inside (6%) was closer to the posterior canal than the anterior canal. Three ethmoidal canals (1-2-3) can be observed at the right ethmoidal roof. P = periorbita; FS = frontal sinus; MT = middle turbinate. Right endoscopic view of the ethmoidal roof, showing an ethmoidal artery inside the AcEC. We can observe how the ophthalmic artery is the origin of this accessory artery.The posterior ethmoidal canal does not contain neither vascular nor neural structure. O = orbit; AEA = anterior ethmoidal artery; AcEA = accessory ethmoidal artery; MRM = medial rectus muscle; SOM = superior oblique muscle;OA = ophthalmic artery; FS = frontal sinus; SS = sphenoidal sinus; MT = middle turbinate. Absence of the right posterior ethmoidal artery with presence of the middle ethmoidal artery This specimen presents the same finding as the Figure 2. O = orbit; AEA = anterior ethmoidal artery; AcEA = accessory ethmoidal artery; MRM = medial rectus muscle; OA = ophthalmic artery; FS = frontal sinus; SS = sphenoidal sinus; MT = middle turbinate. No vascular or neural structure can be showed in the right middle ethmoidal canal (*). O = orbit; AEA = anterior ethmoidal artery; PEA = posterior ethmoidal artery; ON = optic nerve; FS = frontal sinus; SS = sphenoidal sinus; MT = middle turbinate. A neural structure can be exposure in the middle ethmoidal canal with both right anterior and posterior ethmoidal arteries present. O = orbit; AEA = anterior ethmoidal artery; PEA = posterior ethmoidal artery; EN: ethmoidal nerve; FS = frontal sinus; SS = sphenoidal sinus; MT = middle turbinate.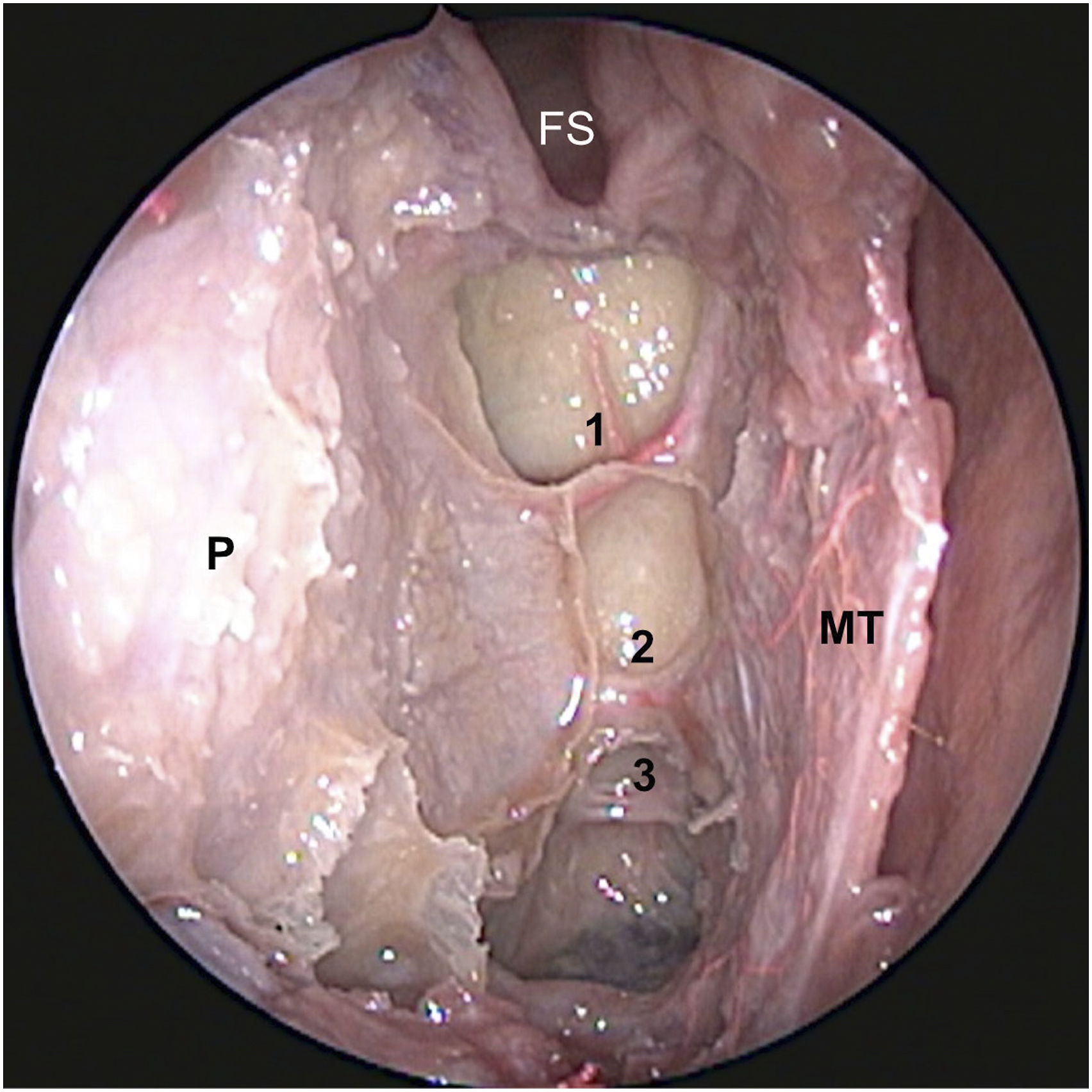
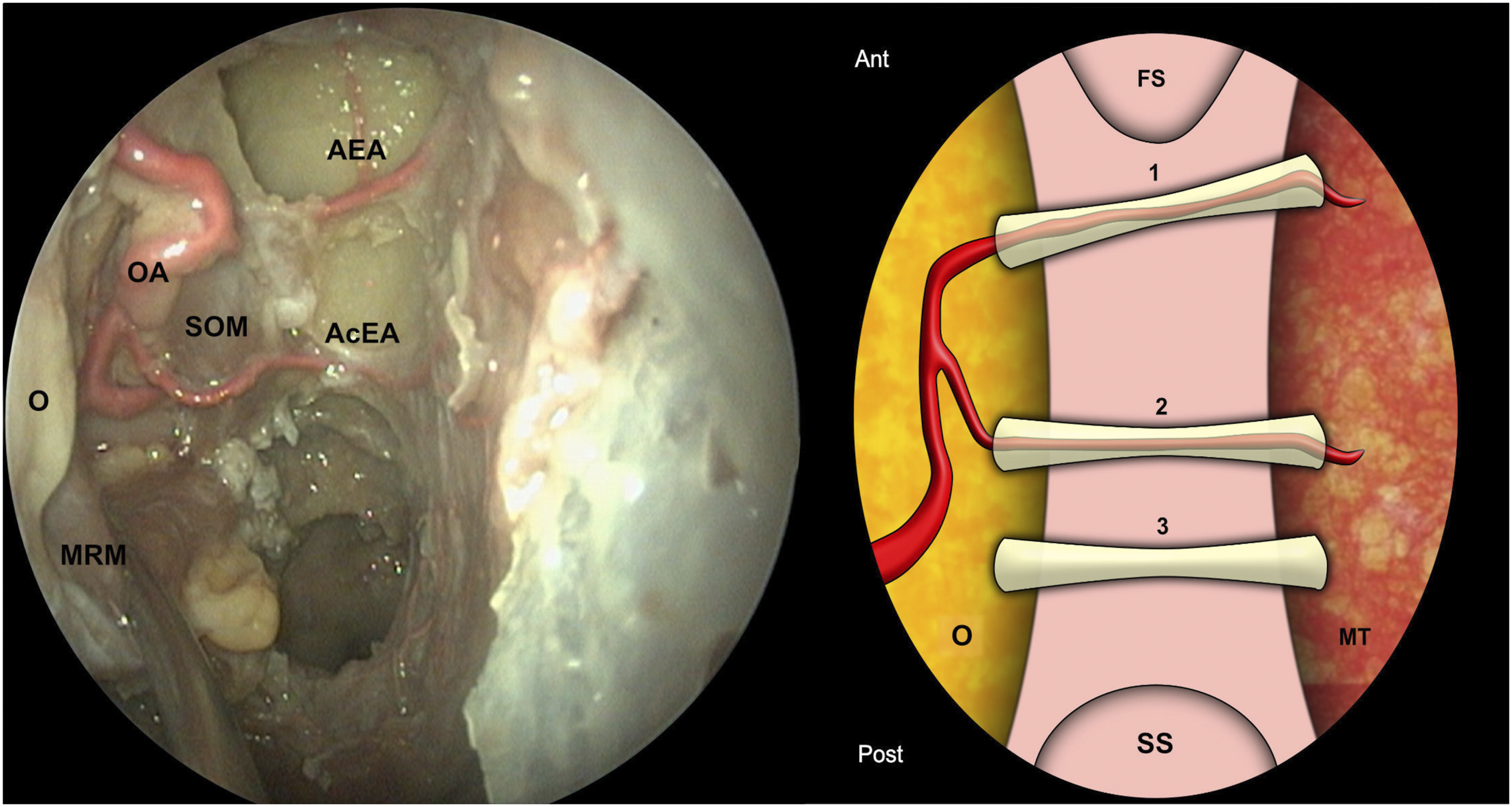
The ophthalmic artery (OA) and the optic nerve (ON) were identified through the anatomical window below and above the medial rectus muscle. In their intraorbital route, the anterior ethmoidal artery (AEA) and the AcEA were situated inferior to the superior oblique muscle (SOM) in all cases. The posterior ethmoidal artery (PEA) was found superior to the SOM. In all cases, the origin of the ethmoidal arteries (AEA, PEA, and AcEA) was the ophthalmic artery.
Discussion
In recent years, several reports, especially endonasal endoscopic studies in cadavers, have described the existence of a middle or accessory ethmoidal artery. It has been described a prevalence between 25 and 42% and in 14% of cases this artery can be bilateral. It seems to be smaller and thinner than the AEA and is located between both ethmoidal arteries, usually closer to the PEA. 12
However, practically, only contemporary anatomical studies mentioned this third ethmoidal artery and it is not present in the classical anatomical descriptions. The pioneer workers in ophthalmic branch arteries are Hayreh SS and Meyer F. 13 They described in detail the origin of all branches arising from the ophthalmic artery and showed a topographical classification of the branches. They described the medial branches of the OA as the ethmoidal arteries, the supraorbital artery, and muscular arteries. None of these arteries cross the ethmoidal complex except the anterior and posterior ethmoidal arteries that were found in the ethmoidal roof. They did not identify any artery between them.
The angiography studies show very interesting findings. De Bonnecaze G. and cols 11 evaluated the origin of nasal bleeding proving the active extravasation after angiography with embolization. Active extravasation arose from sphenopalatine artery followed by anterior ethmoidal artery and facial artery. In no case was observed active extravasation from any accessory ethmoidal artery. Mostafa BE and cols 14 performed a selective angiography of the ICA and ECA for 100 patients undergoing routine angiography. The ethmoidal arteries were found in 95% of cases, while in 5% they were absent, but none of them were listed as a third ethmoidal artery.
Some studies have tried to explain the presence of the AcEA demonstrating the presence of multiple skull orbital foramina. Regoli M and cols,15,16 according to dry skulls, observed 2 ethmoidal canals between 63% to 80% of cases, 3 canals between 17% to 31% of cases, and in less than 2% we observed 4 canals.
Muller SK and cols 17 found more than 2 ethmoidal foramina in the 35% of 273 bone orbits examined of several ethnic groups. Abed SF 18 reported similar data with approximately 42% more than 2 ethmoidal foramina.
All these authors based their studies in the discovering of foramina on the medial orbital wall in dry skull or cadavers heads. But the presence of multiple foramina does not necessarily imply the presence of an arterial vessel inside.
Other authors have adopted the use of computed tomography (CT) to research the anatomy of the ethmoidal canals and have indeed identified the presence of middle ethmoidal artery. Yamamoto 19 analyzed the CT images of 100 patients, identifying a third canal in 21% cases and similar results (28%) were obtained by Ferrari M 20 using cone beam CT. The limitation of these studies was that the arteries were not injected.
Mason E and cols 21 studied computed tomographic angiographies in fifty patients and had evidence of middle ethmoidal vessels in 38% of cases. Instead, in those patients where they could not identify contrast, they decided to interpret bony foramina as evidence for a middle ethmoidal vessel. So, they considered the presence of foramina as an indication of an artery.
Conversely, Monjas I and cols 22 described forty CT-injected cadaver nasal fossae and they did not find any middle ethmoidal artery. They interestedly found 1 case of common ethmoidal trunk for the anterior and posterior ethmoidal artery arising for the ophthalmic artery.
Finally, other studies based their finding in cadaver dissection demonstrating more than 2 canals in the ethmoid roof. Probably the first dissection study about the AcEA in injected specimens was published by Lang and cols in 1990. 23 They examined 71 arterial-injected orbits after the frontal bone was removed and in 33% of cases showed a third ethmoidal foramina that contains an artery.
Berens AM 1 dissected thirty-eight orbits using a transorbital endoscopic approach identifying more than 2 ethmoidal arteries in 58% of the orbits. However, these results have been analyzed with caution because of only 2 orbits were latex injected. Wang L and cols 12 released a more exhaustive paper about the presence of the AcEA. They dissected forty-four nasal cavities after intravascular injection and they verified the presence of the AcEA in 32% of cases. The main contribution is that after locating the third canal they removed the lamina papyracea in order to verify the injected ethmoidal artery. Our study is similar to the Wang and cols but additionally we dissected the intraorbital space in order to verify the origin of the ethmoidal arteries.
We only found a 12% of middle ethmoidal canal and only a 6% of middle or accessory ethmoidal artery. We identified 2 AcEA and they were associated with an absence of posterior ethmoidal artery inside its canal. In these cases, both AEA and AcEA were arising from the ophthalmic artery
Conclusion
Anatomical knowledge of the ethmoidal arteries (including middle ethmoidal artery) is essential for the treatment of epistaxis, for extended endonasal endoscopic surgery of the skull base and for endonasal orbital surgeries. According to our findings, we can suggest that the presence of a canal does not necessarily imply the presence of an arterial vessel, and that presence of the middle ethmoidal artery could be associated with the absence of posterior ethmoidal artery. The AcEA could be supplying the lack of vascularization from the posterior ethmoidal artery.
Footnotes
Acknowledgments
The authors sincerely thank those who donated their bodies to science so that anatomical research could be performed. Results from such research can potentially increase mankind’s overall knowledge that can then improve patient care. Therefore, these donors and their families deserve our highest gratitude.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.