
Abstract
Introduction
Fibrovascular polyps (FVPs) are benign, intraluminal tumours of the upper aerodigestive tract. 1 These tumours produce symptoms after they gradually grow into a large size. Although the incidence of FVPs is rare, caution must be exercised because they may lead to asphyxiation secondary to polyp aspiration; a total of seven such cases of fatalities have been reported in literature. 2 Clinical presentations of FVPs include regurgitation of the polyp to the mouth and progressive dysphagia due to the growing oesophageal tumour. Other symptoms include dyspnoea, vomiting, laryngeal discomfort, weight loss, syncope, anaemia and sore throat. 3
FVPs are potentially lethal, and their surgical excision is essential for improving the symptoms. Transoral, transcervical, transthoracic and transabdominal approaches or a combination of these approaches are generally used for specific oesophageal tumour removal. Malignant transformation and disease recurrence are rare after complete resection. 3
The management of FVPs with hypopharyngeal pedicles (hFVPs) is challenging. Globally, only 16 cases of hFVP have been reported.1,3–12 The accurate diagnosis of hFVP can be problematic if the concerning doctors (gastroenterologists, thoracic surgeons and otolaryngologists) are unaware of the disease and fail to thoroughly examine the patient’s hypopharynx. The lack of accurate diagnosis of hFVP may result in incomplete resection, recurrence of symptoms and repeated surgeries.
Long and thin tumours have been reported in literature that could be removed rapidly from the oesophageal inlet after pedicle severance by using the less invasive transoral endoscopic approach. The presence of an hFVP tumour in the stomach has been reported in only a single case that required gastrotomy (5). However, when oesophageal masses were giant and irregular in shape, the protocol of management could be very different, and minimally invasive transoral approaches (including video assisted endoscopic approach, or robotic approach) might not be adequate to deliver satisfactory haemostasis and mass extraction.
This study analysed the diagnosis and management of 2 cases of giant, irregularly shaped hFVP by using the transcervical approach at a tertiary academic institution.
Patients and Methods
Patients
This retrospective study was conducted in 2 patients with giant, irregularly shaped hFVPs who were treated at the Department of Otolaryngology Head and Neck Surgery, Beijing Friendship Hospital, Capital Medical University in 2018 and 2020. Clinical data of the patients were retrieved. The protocol of the research project was approved by the Bioethics Committee of Beijing Friendship Hospital, and it conformed to the provisions of the Declaration of Helsinki. A written consent form was obtained from the patients.
Case 1 was of a 43-year-old woman, whereas Case 2 was of a 32-year-old man. Both patients received inaccurate diagnoses initially and underwent several surgeries without the proper management of hypopharyngeal pedicles, which eventually failed. Finally, both the patients received the accurate diagnosis of hFVP and were successfully treated at our department. Both patients received a routine follow-up.
Diagnostic Workup
The preoperative diagnostic workup included fibreoptic laryngoscopy for evaluating the hypopharynx and identifying the pedicle of the giant oesophageal tumour; barium swallow test for demonstrating the intraluminal nature of the oesophageal tumour by observing the circumferential flowing down around the oesophageal tumour; gastroscopy also for demonstrating the intraluminal nature of the oesophageal tumour (yet in the case of giant hFVP, its view could be blocked, and might not be able to give definite conclusions); and computed tomography (CT) and magnetic resonance imaging (MRI) with contrast for analysing the extent, feature and shape of the tumour to design a management strategy.
Surgical Procedure
Complete removal of the hypopharyngeal pedicles is crucial for the successful management of hFVPs. The transcervical approach and hypopharyngeal incision were utilised in the 2 cases because of two reasons. First, the size of oesophageal tumours was large. Second, both the hypopharyngeal pedicles were thick and had high vasculature, which was confirmed intraoperatively.
The transcervical approach involved a horizontal incision on the lowest cervical skin crease above the clavicles, followed by elevation of the subplatysmal flaps and lateral retraction of the strap muscles. Superior vascular pedicle of thyroid lobe ipsilateral to the hypopharyngeal pedicle was ligated, and the entire lobe was mobilized and retracted to the contralateral side. The superior and recurrent laryngeal nerves were monitored and preserved. The ipsilateral half of the hyoid bone was removed for additional hypopharyngeal exposure, followed by detachment of the muscles attached with the ipsilateral thyroid cartilage. The lateral hypopharyngotomy was performed to reveal the bulky hypopharyngeal pedicle, followed by removal of the entire pedicle from the hypopharynx. After achieving haemostasis, the whole tumour was gradually pulled out of the oesophagus. Multiple layers of suturing of the hypopharyngeal mucosa were performed, and the recovered muscles were utilised for protecting the hypopharyngeal wall. Negative-pressure suction device was placed, and incision was closed.
Results
Case 1
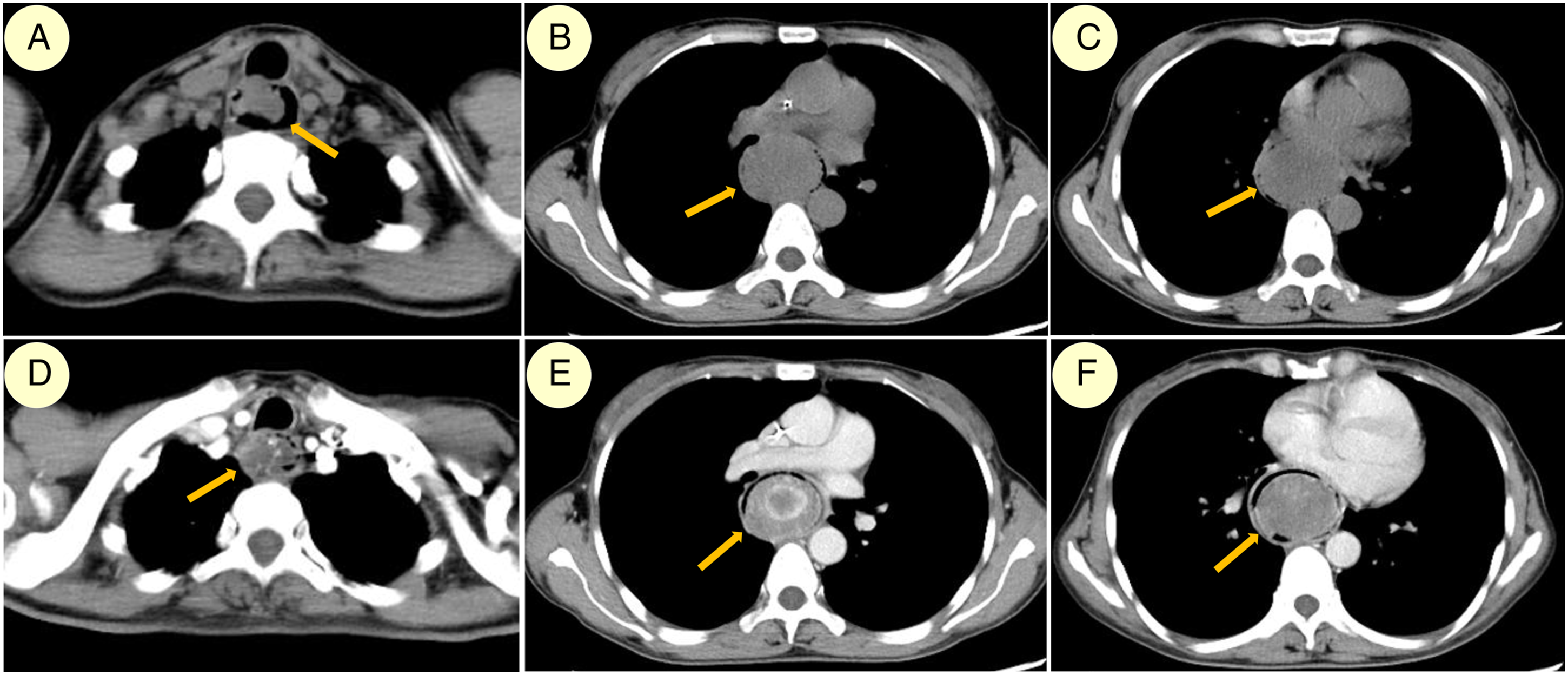
The female patient with progressive dysphagia for 2 months received a diagnosis of FVP through gastroscopy, CT, MRI and barium swallow test, which confirmed a giant tumour in her oesophagus. The oesophageal tumour was 20 cm in length, with a maximum width of approximately 6 cm in the middle section (Figure 1 and 2). Preoperative evaluations of the first patient. A, Endoscopic image illustrating hypopharyngeal pedicle (yellow arrow) on the right side, without apparent involvement of the laryngeal inlet; B, three-dimensional reconstruction CT image of a long rod-shaped oesophageal mass (yellow arrow) that was widest in the middle. Horizontal CT scans of the first patient. A–C, CT scan demonstrating the proximal, middle, and distal oesophageal masses, exhibiting the broadest mass at the middle section (yellow arrows); D–F, contrast CT scan image corresponding to A–C, exhibiting a slightly enhanced oesophageal mass (yellow arrows). Note: CT: computed tomography.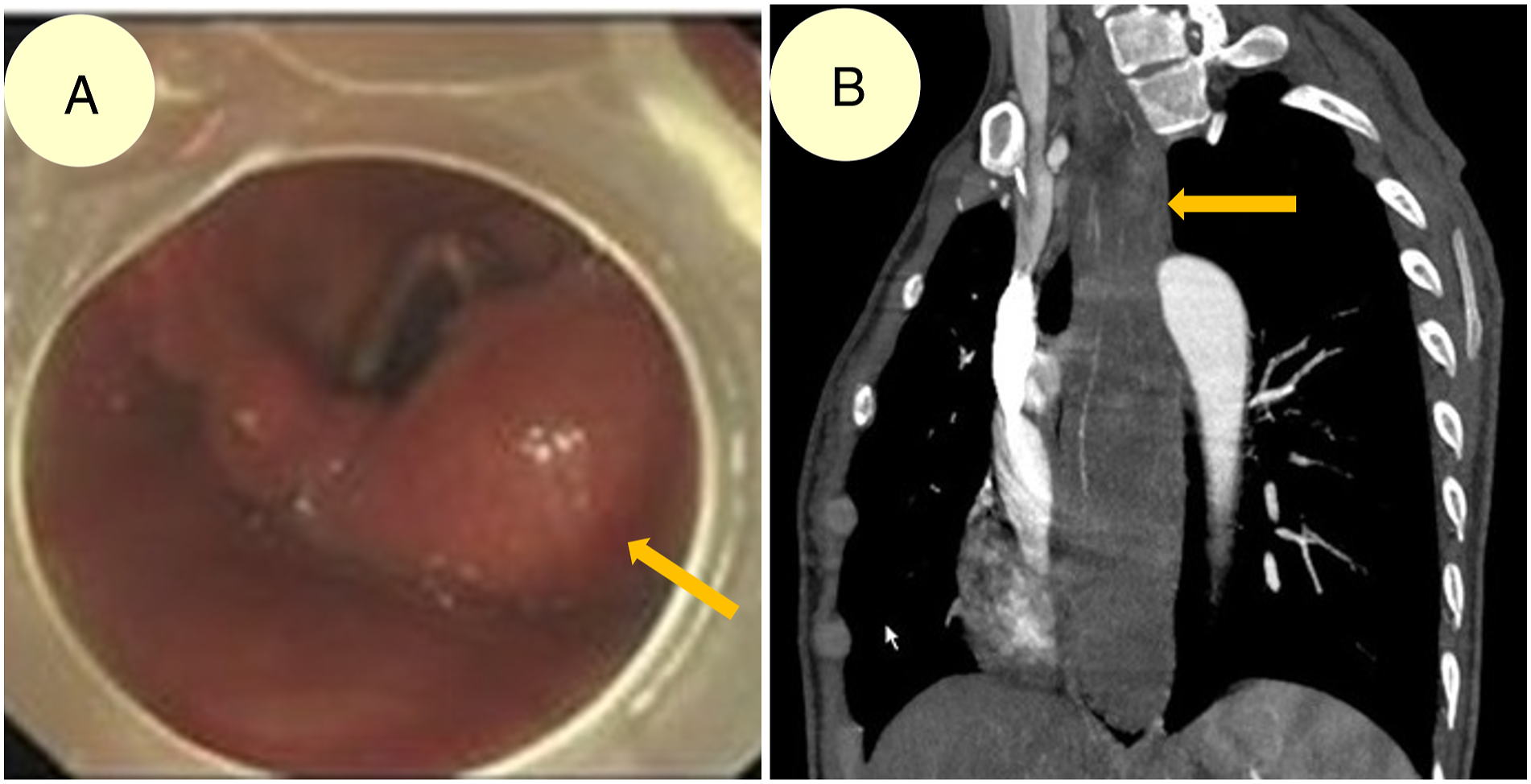
Initially, gastroenterologists overlooked the origin of this FVP, and decided to sever its narrowest point in the oesophagus under endoscope. However, the oesophageal tumour could not be moved. The patient was transferred to the intensive care unit (ICU), expecting a downward tumour movement into the stomach due to necrosis. However, the peristaltic movement failed to move down the tumour even after 7 days in the ICU. Eventually, a transabdominal gastrotomy procedure was performed to remove the oesophageal tumours and avoid toxic effects of the necrotising tumour.
Symptoms recurred after 3 months, and the patient was referred to our department. Fibreoptic laryngoscopy revealed the presence of a hypopharyngeal pedicle, and the diagnosis of hFVP was made. The transcervical approach was used to sever the hypopharyngeal pedicle that occupied an area of approximately 7 cm2 of the medial wall of the right pyriform sinus and to achieve haemostasis of the heavily diffused haemorrhage. The tumour was removed successfully. Recovery was smooth. The final pathology report confirmed the presence of hFVP. No recurrence was detected during the 2-year follow-up period.
Case 2
The male patient with a history of progressive dysphagia was diagnosed as having a giant intraluminal oesophageal mass 4 years ago. Despite this, the concerning thoracic surgeons did not attempt to determine the origin of the mass. First, the patient underwent a transthoracic oesophagotomy procedure, which revealed that the pedicle of the mass too high to be completely resected. Three months later, a transcervical oesophagotomy procedure was performed to remove the residual oesophageal mass. However, the origin of the tumour was not determined.
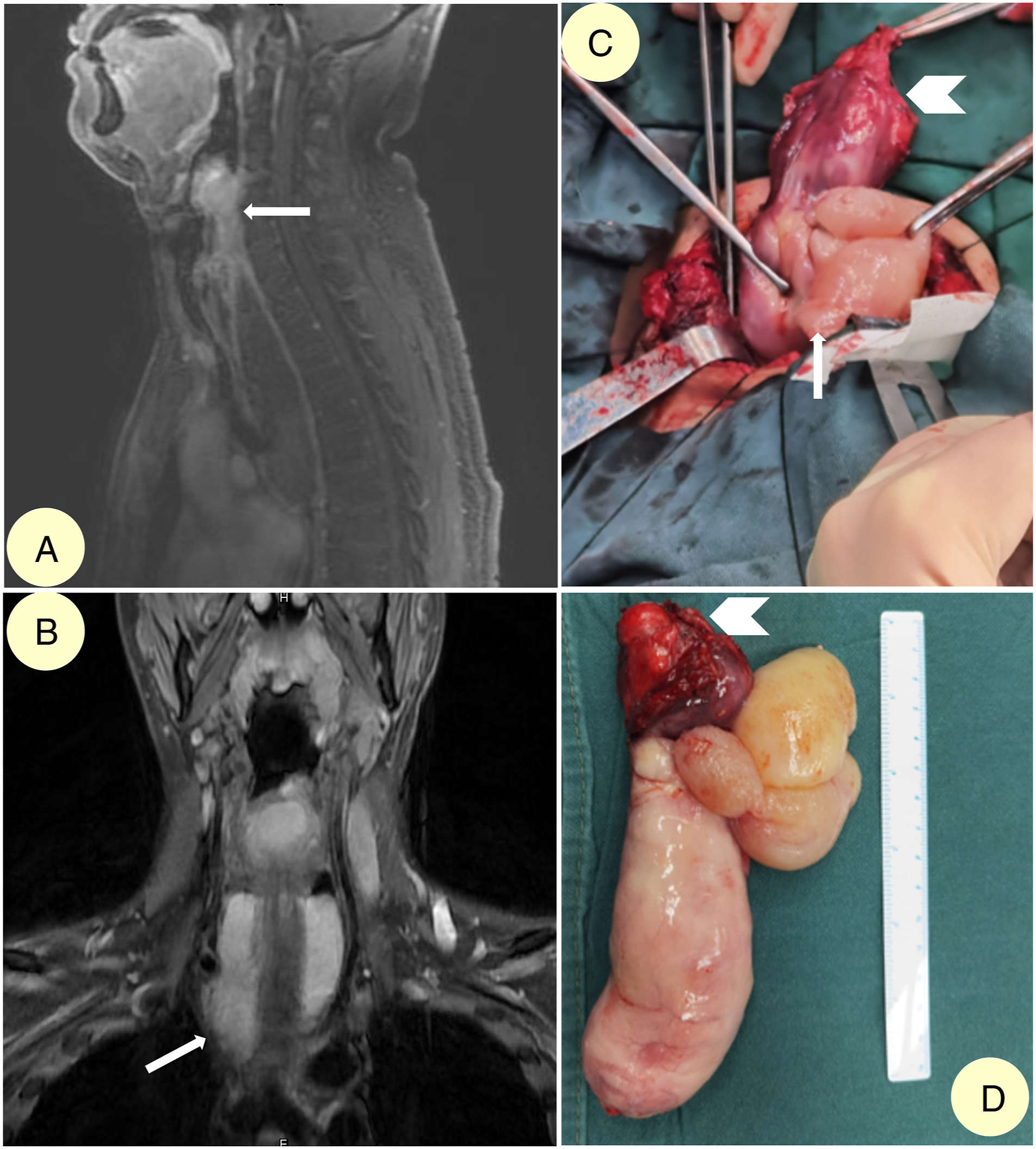
Although the symptoms improved considerably after the second surgery, the patient was presented to our department 4 years after surgery due to the recurrence of progressive dysphagia along with slight dyspnoea. A giant, irregularly shaped hFVP was detected after a careful preoperative workup, which included fibreoptic laryngoscopy, gastroscopy, CT, MRI and barium swallow test. The maximum width of the oesophageal tumour was approximately 6 cm near the oesophageal inlet, which was also enlarged (Figure 3 and Figure 4). Gastroenterologists and thoracic surgeons were consulted with, and they all agreed that we should try the transcervical approach first. Preoperative evaluations of the second patient. A, Endoscopic image illustrating hypopharyngeal pedicle (white arrow) on the left side, with prominent involvement of the laryngeal inlet; B, barium swallow test exhibiting filling defect from the left hypopharynx down to middle oesophagus; barium can flow down on all sides of the oesophageal mass, suggesting an intraluminal mass; C–E, T1WI, T1WI with contrast and T2WI image of the horizontal MRI scan of the oesophageal inlet, exhibiting a sizeable oesophageal mass (white arrows) with obviously enlarged oesophageal inlet. Preoperative MRI scans and intraoperative images of the second patient. A, Sagittal T1WI image of the whole hFVP; B, Coronal T2WI image of the upper part of hFVP; C, Intraoperative image of pulling out the oesophageal mass (white arrow) after severance of its hypopharyngeal pedicle (white arrowhead); D, The whole 15-cm-long hFVP, with a richly vascularised hypopharyngeal pedicle (red upper part, white arrowhead), and a wide (6-cm diameter) and multilobular proximal section. Note: MRI: magnetic resonance imaging; hFVP: fibrovascular polyp with hypopharyngeal pedicle.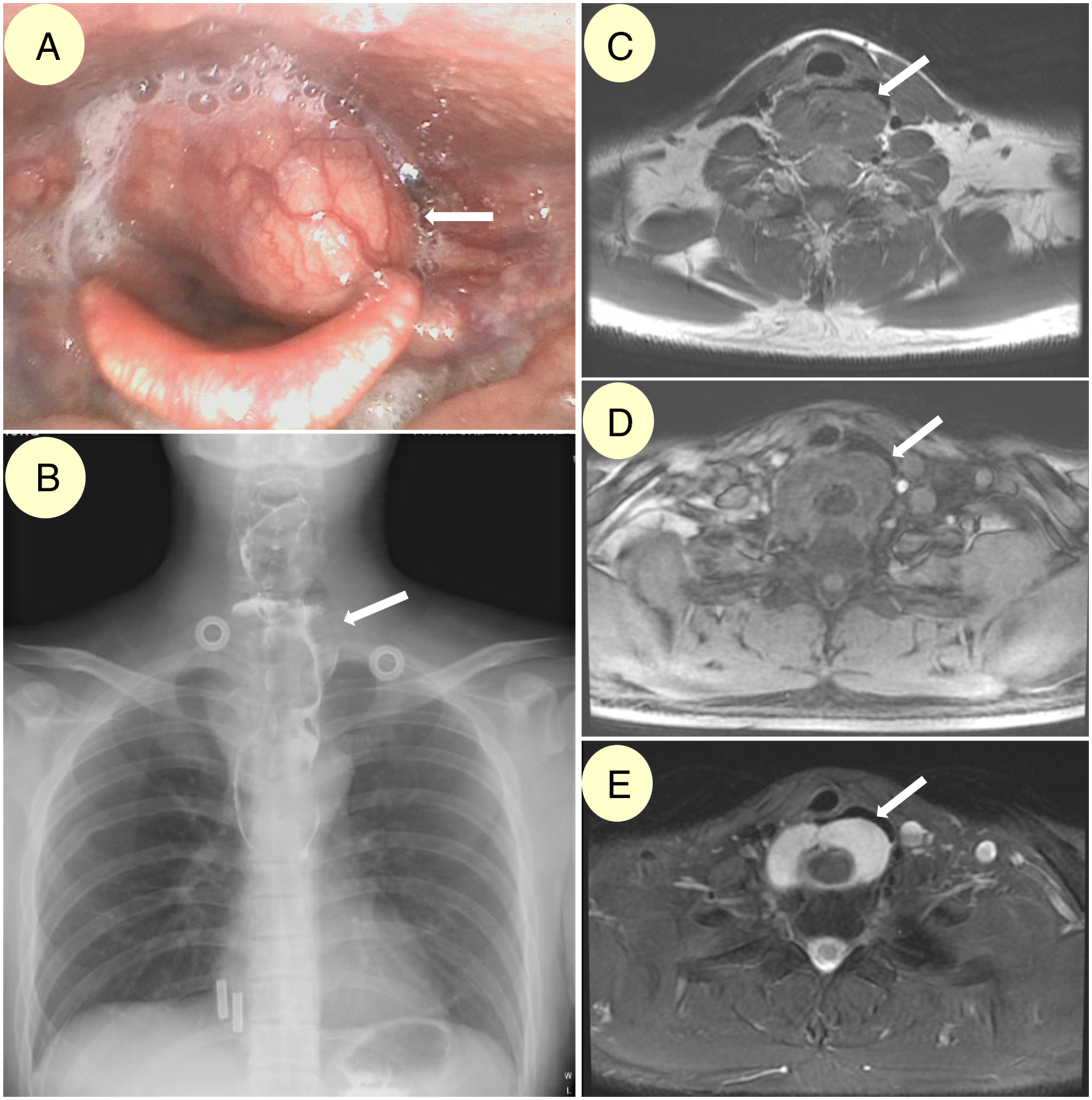
During surgery, the hypopharyngeal pedicle was found to be thick, with an area of approximately 4.5 cm2 and located majorly on the medial wall of the left pyriform sinus. Some parts were found in the post cricoid region, which caused the blockage of the laryngeal inlet. The hypopharyngeal pedicle was completely severed, and haemorrhage was rather heavy and diffuse. After achieving haemostasis, the oesophageal tumour (15 cm in length) was pulled out smoothly, and a giant multilobular tumour with the maximum width immediately below the hypopharyngeal pedicle was discovered (Figure 4). Recovery of the patient was smooth. The final pathology report could not rule out liposarcoma based on immunohistochemistry assays. The patient was informed, and agreed to routine observation (without postoperative radiotherapy or chemotherapy). No recurrence was detected during the 6-month follow-up period.
Discussion
FVPs have been named as fibromas, fibrolipomas, myxofibromas, polyps and pedunculated lipomas, all of which have been grouped and classified under FVP, according to the recommendations of World Health Organization’s International Histological Classification of Tumours. 6
Locating the exact origin or pedicle of an FVP, particularly the hFVP, is essential for an accurate diagnosis. Since hFVPs are extremely rare, they are easily overlooked, which leads to recurrence of symptoms and unsuccessful surgical procedures, causing physical, economical and psychological burden to patients. Thus, gastroenterologists and thoracic surgeons should be aware of hFVPs. Additionally, a consensus should be reached that otolaryngologists should be consulted with whenever the pedicle of a FVP is not definitely confirmed, and whenever a hypopharyngeal one is suspected. Moreover, fibreoptic laryngoscopy should be included as a routine examination in the diagnostic workup of FVPs to avoid misdiagnosis.
The hFVPs likely originate as nodular submucosal thickenings that elongate progressively due to the combined forces of the local peristalsis and the friction created by the traction of moving debris. 1 FVPs may even grow into the stomach with a length of 26 cm. 5 Hence, we believe one advantage of managing hFVPs through an open transcervical approach is that, any redundant mucosa around the stalks of hFVPs could be removed, because this manoeuvre may prevent further recurrences caused by the continuous propulsive forces of the oesophagus. 2
Histologically, giant oesophageal polyps are covered by the squamous epithelium and have a fibrovascular axis comprising various types of adipose and connective tissues and a well-developed vascular network. 12 Hence, it is our belief that the vasculature within the hypopharyngeal pedicle would gradually increase to sustain a giant and growing oesophageal mass, and the size of the pedicle itself would also gradually increase. Therefore, we believe another important advantage of utilizing the open transcervical approach to deal with hypopharyngeal pedicles is that, haemorrhage can be better managed than transoral endoscopic approach. In this study, broad hFVPs with a high degree of vasculature were discovered. Diffuse and heavy haemorrhage was observed after the complete severance of hypopharyngeal pedicles, although no apparent bleeding vessel could be identified. Therefore, achieving haemostasis was challenging even with constant suction and bipolar coagulation. A postoperative haemostatic was required. In an open approach, constant suction and bipolar coagulation are very convenient in dealing with heavy haemorrhage, which would not be so easy for transoral endoscopic approaches, for their limited access to hypopharynx, and for lack of apparent haemorrhaging vessel to clip on.
Furthermore, when proximal oesophageal mass was wide, leading to secondary expansion of oesophageal inlet, transcervical incisions were useful to make hypopharyngeal and even cervical oesophageal incisions that were big enough to allow extraction of giant oesophageal mass. If minimally invasive techniques (like transoral robotic approach) were to be tried for giant masses with broad hypopharyngeal pedicles, diffuse and heavy haemorrhage would be adequately managed, yet extraction routes might still be a problem, since hypopharynx is a relatively narrow passage, and masses as bulky as 6 cm in diameter would not be able to pass through.
However, the transcervical approach does not always provide a significant outlet for the removal of hFVPs. For example in Case 1, the oesophageal tumour had the maximum width at its middle part, which is relatively far from the unexpanded oesophageal inlet and gastric cardia, preventing the oesophageal tumour from being pulled up or pushed down. Retrospectively reasoning, the transcervical and transthoracic approaches should be combined for removal of such cases of hFVP.
This study is limited by a small sample size, which is because of the rare incidence of hFVP. Moreover, the diagnostic workup and treatment algorithm presented in the present study were mainly based on our reasoning and experience, and require further validation through the clinical observation of more cases.
Conclusion
hFVPs are rare tumours of the upper aerodigestive tract, and their accurate diagnosis relies on careful diagnostic workup, especially fibreoptic laryngoscopy. Complete surgical removal of hFVPs with proper management of the pedicles is essential for their successful treatment and prevention of recurrence. The surgical approach should be customised according to the shape and size of the oesophageal tumour, especially after determining the location of the maximum width of the tumour. The transcervical approach is an excellent method for achieving haemostasis and removing giant, irregularly shaped hFVPs.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by Research and Development Project of Scientific Research Instruments and Equipment of Chinese Academy of Sciences-major instruments project [grant number YJKYYQ20180039], Digestive Medical Coordinated Development Center of Beijing Municipal Administration of Hospitals [grant number XXZ0604], and Key Science and Technology Program of Beijing Municipal Commission of Education [grant number KZ202110025035].