
Abstract
Current treatment guidelines recommend surgical excision of papillary thyroid carcinoma. However, the precise surgical treatment, including thyroid lobectomy, total thyroidectomy, and the need for neck dissection, is dictated by disease extent and tumor cytology. Incidental papillary thyroid carcinoma discovered during another surgery therefore presents a surgical conundrum due to lack of information. Surgeons must consider short- and long-term surgical morbidities, as well as individual patient factors, when deciding how to treat an unexpected thyroid carcinoma.
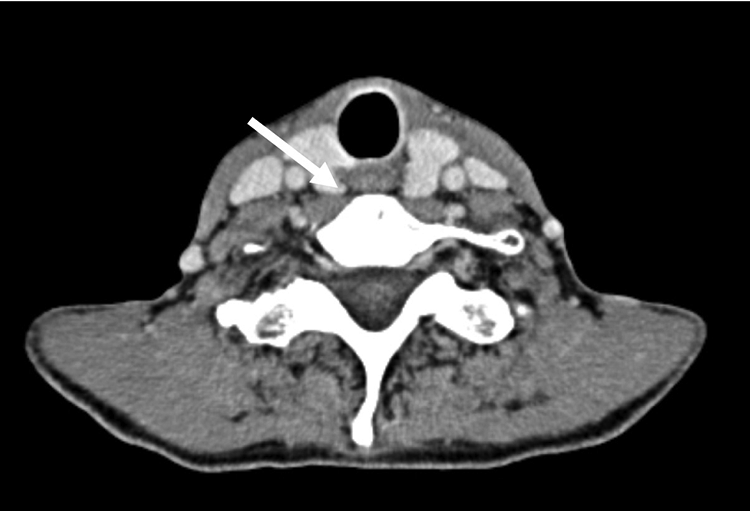
A 77-year-old female patient was referred to our clinic for the management of primary hyperparathyroidism (pHPT). Her past medical history was significant for diabetes mellitus and stage III chronic kidney disease. Previous laboratory analysis showed a slightly elevated calcium level of 10.8 mg/dL and a parathyroid hormone level on the upper side of normal at 59.4 pg/mL. Further 4D computed tomography (CT) imaging revealed a suspected left superior parathyroid adenoma (Figure 1). Importantly, the patient had known left Thyroid Imaging Reporting & Data System (TI-RADS) 4 and TI-RADS 5 benign follicular thyroid nodules (Figure 2), with a 0% to 3% implied risk of malignancy on fine needle aspiration (FNA). She was consented for a left parathyroidectomy, possible parathyroid exploration, and possible hemithyroidectomy in the event of an intrathyroidal parathyroid gland.
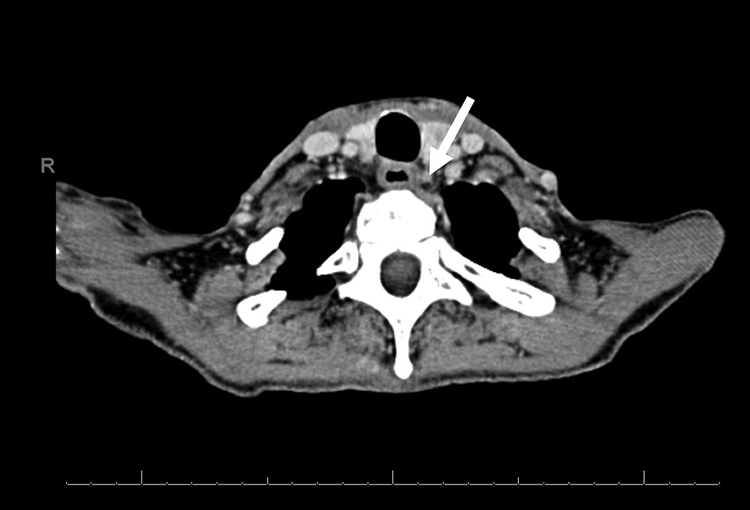
Axial 4D computed tomography scan demonstrating the suspected left superior parathyroid adenoma.

Axial contrast-enhanced computed tomography demonstrating the left-sided thyroid nodules, which were benign on fine needle aspiration.
During surgery, dissection of the area of suspected parathyroid adenoma revealed a dark, nodular mass, which was sent to pathology for frozen section analysis. To our surprise, pathology identified two lymph nodes with a 0.5 cm focus metastatic papillary thyroid carcinoma. Given that the patient was previously consented for a hemithyroidectomy and had known left-sided thyroid nodules, we decided to proceed with a left hemithyroidectomy. The left superior and inferior parathyroid glands were identified and were grossly normal in appearance. In anticipation of a future right completion thyroidectomy, the left parathyroid glands were tagged with suture but left in situ to reduce the risk of iatrogenic hypoparathyroidism. Pathology evaluation of the left thyroid lobe confirmed a 0.9 cm papillary thyroid carcinoma with classic papillary architecture. On follow-up, the patient ultimately decided to proceed with a completion hemithyroidectomy and right parathyroid exploration, which identified a right superior parathyroid adenoma.
Papillary thyroid carcinoma is the most common primary thyroid malignancy, accounting for 80% to 85% of thyroid cancer cases and occurring predominantly in females. 1 Concurrent nonmedullary thyroid carcinoma in patients with pHPT was first reported by Ogburn and Black in 1956, with further studies identifying an incidence of thyroid malignancy in 2% to 15% of pHPT patients.2,3 Specifically, Bentrem et al reported that 12% of incidental thyroid lesions found in patients undergoing pHPT surgery were malignant papillary carcinomas, indicating an overall malignancy rate of 2%. 4 Their findings support preoperative thyroid imaging and FNA biopsy of patients with HPT to assess for concurrent pathology. Ultrasound is the first-line imaging modality for evaluating the thyroid due to its wide availability, relative simplicity, and lack of ionizing radiation. 5 Overall sensitivity and specificity of FNA for thyroid malignancy is 0.72 (95% CI: 0.69-0.74) and 0.83 (95% CI: 0.81-0.85). 6 Four-dimensional CT can be used to identify parathyroid adenomas and is able to localize an adenoma to a quadrant with 87% sensitivity when used as a first-line modality. However, intrathyroid parathyroid adenomas and thyroid nodules can present with similar contrast enhancement patterns, leading to false-positive or false-negative results. 7 Similarities in contrast enhancement between thyroid tissue and parathyroid adenomas likely led to the incorrect identification of metastatic papillary thyroid cancer as a left superior parathyroid adenoma in this case (Figure 3).
Axial 4D computed tomography at 85-second washout demonstrating the right adenoma. Note the similarity in contrast enhancement with the suspected adenoma in Figure 1.
Limited literature exists on the management of incidentally discovered thyroid carcinoma during another surgery. Treatment of papillary thyroid carcinoma is primarily surgical, either total thyroidectomy or thyroid lobectomy, with the primary goal of preventing disease recurrence. Total thyroidectomy not only lowers the risk of locoregional recurrence but also isolates thyroglobulin as a sensitive postoperative marker for residual or recurrent disease surveillance. 8 However, total thyroidectomy can be associated with additional complications including temporary or permanent hypoparathyroidism (3%-10%),9,10 bilateral vocal cord palsy (0.4%-14%), 11 and life-long thyroid hormone replacement. To limit patient morbidity, thyroid lobectomy should be considered in patients with low- or intermediate-risk papillary or follicular thyroid carcinoma. 12 However, for patients with regional nodal involvement, total thyroidectomy is recommended. 13
In this patient’s case, we decided to proceed with an initial thyroid lobectomy based on the known left-sided thyroid nodules. Furthermore, we had already discussed the details of thyroid lobectomy with her as part of the preoperative informed consent process. Otolaryngologists must consider individual patient characteristics and surgical morbidity when determining best treatment course for incidental papillary thyroid carcinoma.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.