
Abstract

Significance Statement
Currently, due to the spread of the COVID-19 pandemic, the need for long-term mechanical ventilation in many critically ill patients represents the most common situation for which tracheostomy is performed. Given the growing number of new procedures, it is possible to expect a future increase in the number of patients who will develop cicatricial tracheal stenosis. This condition should be kept in mind for patients with a history of mechanical ventilation who experience progressive dyspnoea. We present a case of a 64-year-old man who successfully underwent surgical treatment of tracheal stenosis after tracheotomy for COVID-19.
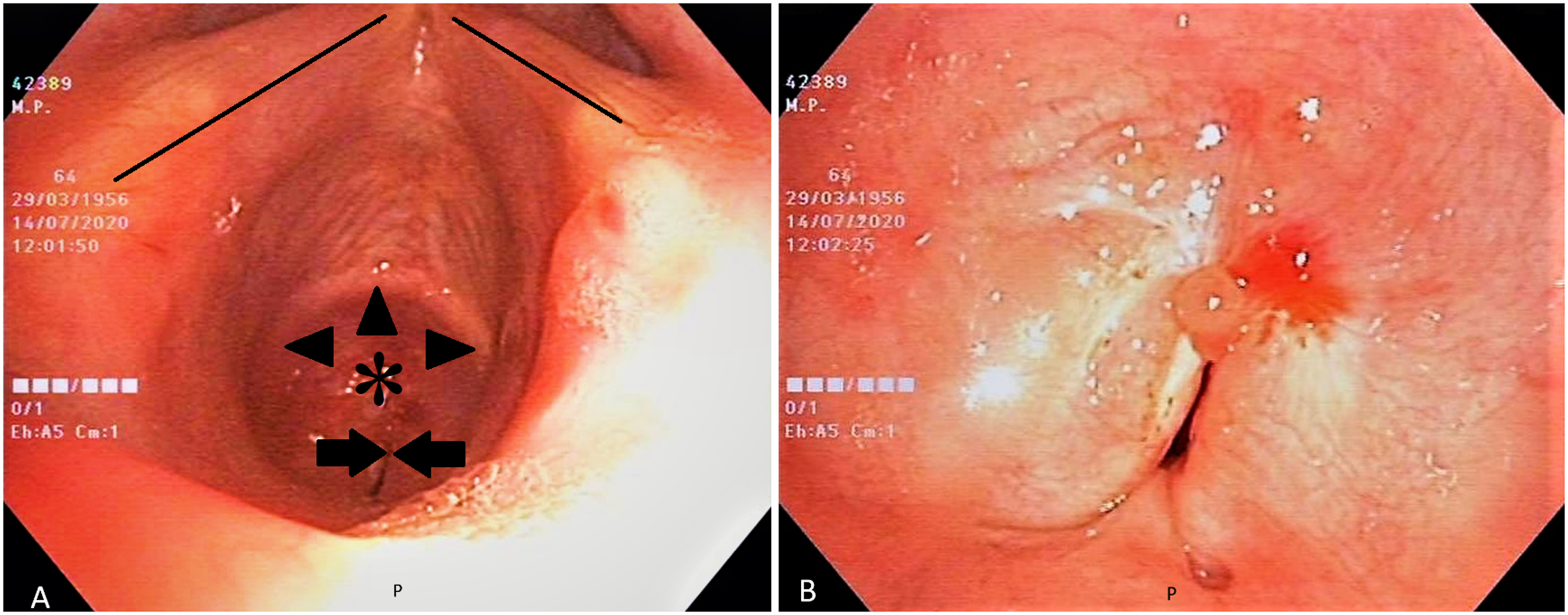
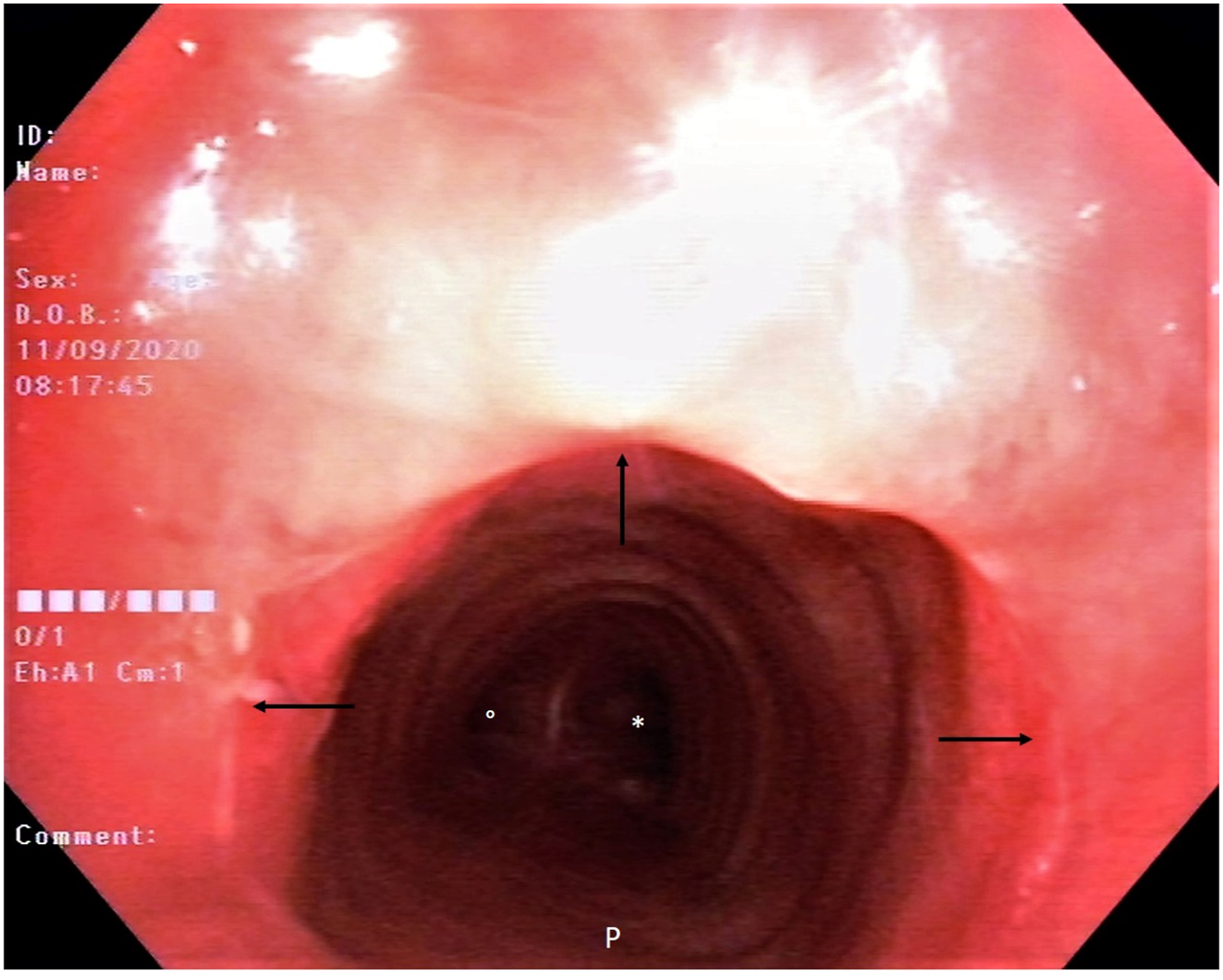
A 64-year-old man presented to the emergency department with dyspnoea on exertion and shortness of breath that started 2 months prior and progressively worsened. At admission, he had normal resting oxygen saturation and did not need immediate treatment or intubation. Six months prior, he had undergone mechanical ventilation via an orotracheal tube for the first week and then via a tracheotomy tube for the next 35 days for severe COVID-19 pneumonia. Lung CT scan showed no signs of pneumonia. High-resolution coronal CT scan of the chest (Figure 1) showed, passing through the tracheal lumen (white asterisks), severe stenosis of the lumen of the cervical portion of the trachea (opposing white arrowheads). Transoral flexible fibreoptic tracheobronchoscopy (Figure 2A) documents, just inferior to the vocal cords (black arrows) and the inferior border of the anterior arch of the cricoid cartilage (black arrowheads), tight concentric stenosis of the tracheal lumen (black asterisk). Residual respiratory patency (white opposing arrows), reduced to a small crack just in front of the posterior tracheal wall (grade III, Myer–Cotton classification), can be seen in detail in Figure 2B (opposing arrows). The patient underwent ‘open field’ tracheal resection of the stenotic segment, with tracheal reconstruction by direct termino-terminal anastomosis. Definitive pathology on mucosal specimens showed no signs of malignancy. The patient was discharged in good health on the 12th postoperative day. Transoral flexible fibreoptic tracheobronchoscopy performed about 2 months after surgery (Figure 3) showed no signs of relapse of the stenosis. The tracheal lumen at the level of the anastomosis, whose scar is clearly identifiable (arrows), was normally patent. Right (°) and left (*) main bronchi are clearly visible through the anastomosis. High-resolution CT scan of the chest: a coronal plane image passing through the tracheal lumen, showing severe stenosis of the lumen of the cervical portion of the trachea (opposing white arrowheads). Transoral flexible fibreoptic tracheobronchoscopy (A): Tight concentric stenosis of the tracheal lumen (asterisk), just inferior to the vocal cords (black lines) and the inferior border of the anterior arch of the cricoid cartilage (black arrowheads), can be seen. Tracheal patency is reduced to a small crack just in front of the posterior tracheal wall (black opposing arrows). (B): Residual tracheal patency in detail. Postoperative flexible fibreoptic tracheobronchoscopy showing no signs of relapse of the stenosis. Tracheal anastomosis is patent and clearly identifiable (arrows). Right (°) and left (*) main bronchi are clearly visible through the anastomosis.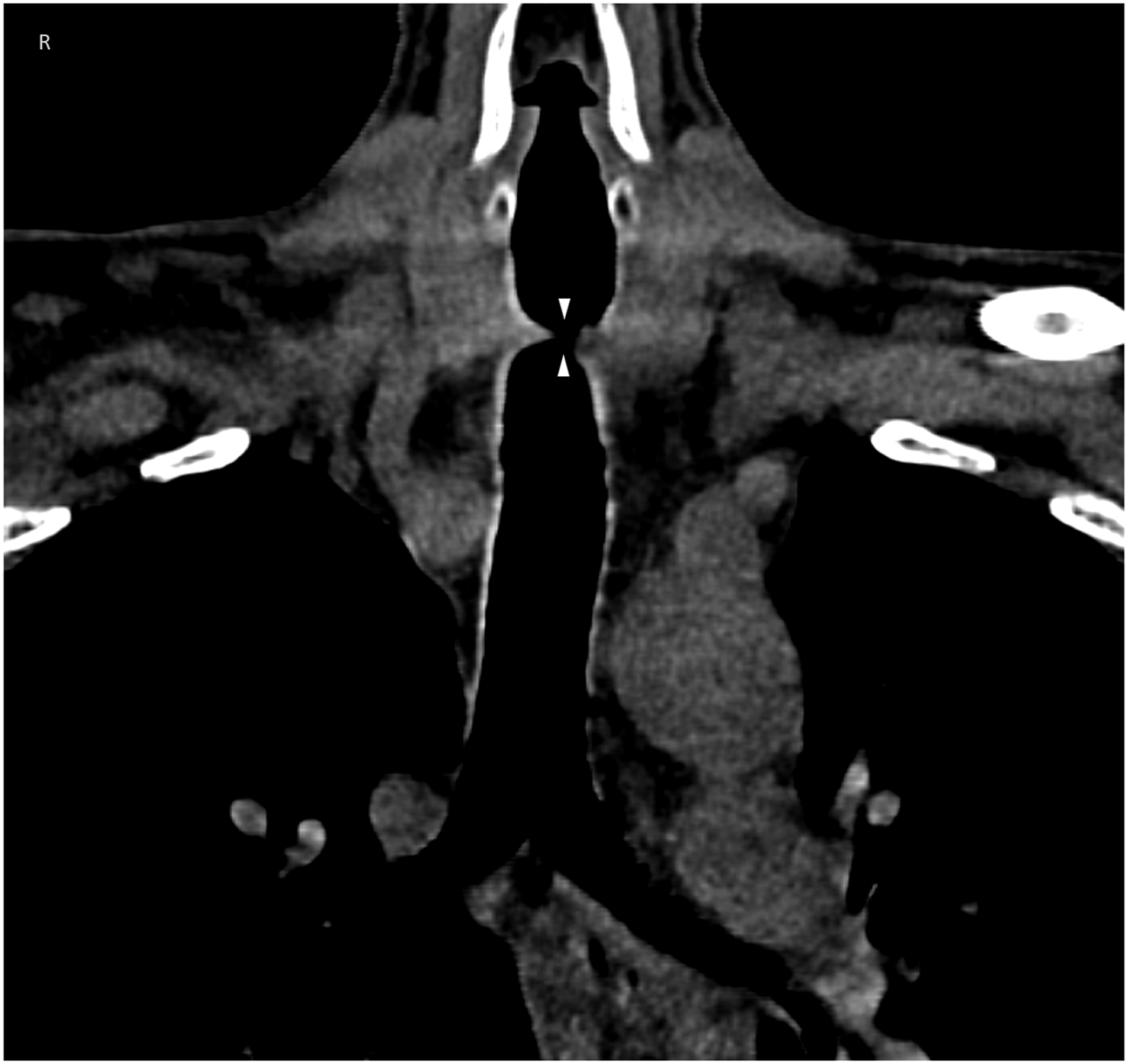
Cicatricial stenosis of the trachea should be considered for dyspnoeic patients with a history of mechanical ventilation. Intubation-related tracheal ischaemic lesions are the initial injury that eventually causes stenosis. Currently, due to the spread of the COVID-19 pandemic, the need for long-term mechanical ventilation and tracheostomy is increasing. 1 Thus, the number of patients who will develop cicatricial tracheal stenosis is likely to increase in the future. 2 The management of tracheal stenosis is still controversial. The aim of the treatment is to restore the airway patency and preserve swallowing and voice. Endoscopic or open surgical approaches are treatment options. On the basis of the type and grade of the stenosis, surgical treatment can be performed using ‘open field’, ‘endoscopic balloon dilatation’, ‘endoscopic laser-assisted’ or ‘endoprostheses’ procedures. 3 Endoscopic approaches are the first-line treatment options in ‘thin and young’ stenosis. But prolonged orotracheal intubation or tracheostomy can cause traumatic injury to the cartilage. Open surgical techniques could be the treatment of choice in patients with no severe comorbidities if the cartilage scaffold is disrupted. Given the complexity of this condition, multidisciplinary management in high-volume centres would be worthwhile.
Footnotes
Acknowledgements
The authors would like to thank the medical and nursing community worldwide who care daily for COVID-19 patients.
Author Contributions
DG, CB and AC: conception and design of the work, analysis and interpretation of data, drafting of the article and final approval. RP and AG: acquisition of data, critical revision of the article for important intellectual content and final approval.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.