
Abstract

Significance statement
During the COVID-19 era, tracheostomy was widely performed on a large number of patients, who were in need of prolonged intubation. In this clinic, we present a modified approach, which combines the open and percutaneous methods, that was utilized by the surgeons in our department on COVID-19–positive patients with difficult neck anatomy inside the intensive care unit (ICU), who are not compatible for a percutaneous tracheostomy.
The procedure described is performed by 2 operating surgeons, at the bedside of the patient inside the ICU. All personnel had full personal protective equipment on (FFP3 mask, eye protection, full-body gown with water resistance, and double gloves). The patient under sedation, with adequate neuromuscular blocking in order to prevent coughing, was placed in a supine position; the neck is extended, and the head is stabilized. An antiseptic solution is applied at the anterior side of the neck and sterile drapes are placed. The thyroid notch, the suprasternal notch, and the inferior border of the cricoid cartilage are recognized.
After infiltration with a local anesthetic, a 3- to 4-cm transverse incision is made equidistant between the cricoid cartilage and the suprasternal notch. The subcutaneous tissues and the platysma muscle are dissected until the muscles below the hyoid are visible. The strap muscles are retracted laterally and the isthmus of the thyroid is identified and retracted. The anterior tracheal wall comes into view (Figure 1A). (Α) After the primary incision of the skin, the subcutaneous fat and the platysma are dissected and the strap muscles and thyroid retracted, until the trachea is visible (yellow arrow) and (B) punctured with a needle connected to a syringe, to verify the location inside the lumen.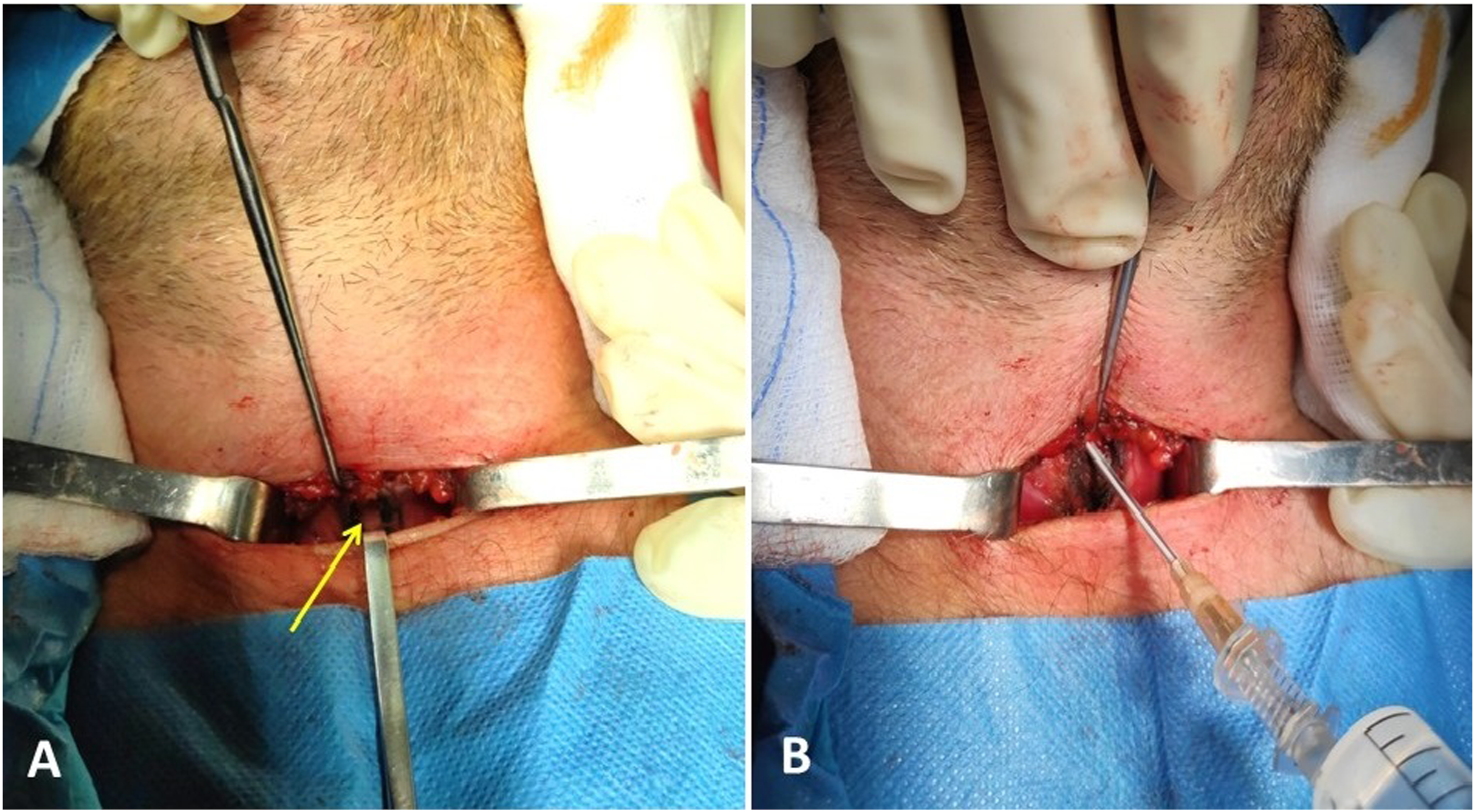
Next, the anesthesiologist moves the endotracheal tube slightly superiorly. The trachea is punctured between the second and third tracheal cartilage, with the needle included in the percutaneous tracheostomy set angled slightly caudally. Its location is confirmed via aspiration with a syringe filled with natural saline, with bubbles emerging when the tip of the needle is inside the lumen (Figure 1B).
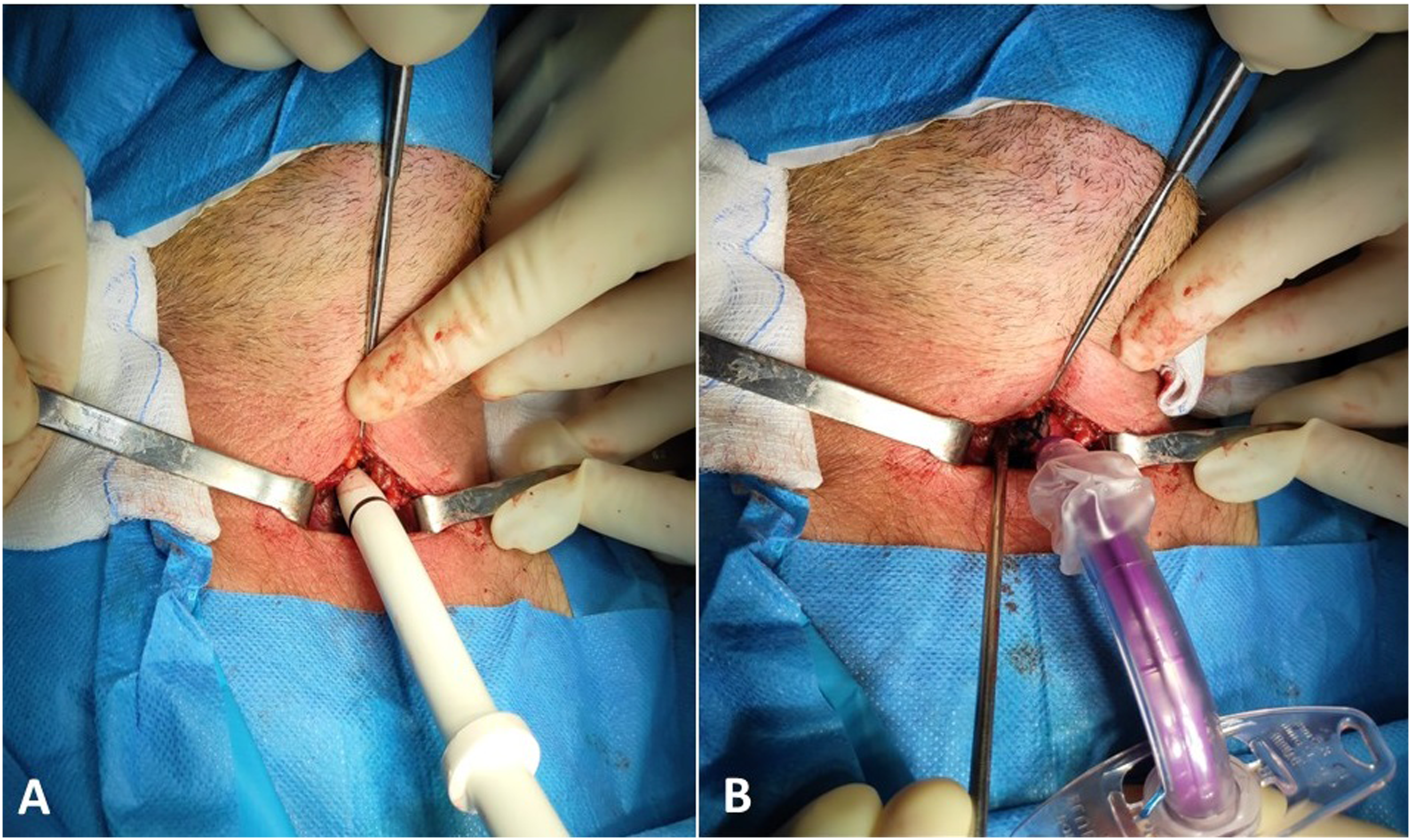
The syringe is disconnected, and the guidewire is placed through the needle-sheath inside the trachea (Figure 2A). The sheath is cautiously removed, and primary dilation begins with the forceps included in the tracheotomy set (Figure 2B). The tracheal dilator is carefully fed through the wire (Figure 3A), creating an opening through which the tracheostomy tube is placed under direct vision through the guidewire (Figure 3B). Afterward, the wire is removed, the cuff is inflated, and the tube is connected to the ventilator, confirming its position. The tracheostomy site is checked for bleeding, loose sutures are applied on the skin, the tube is secured, and proper dressing is placed. (Α) A guidewire is fed through the needle sheath. (B) After its removal, primary dissection with the forceps included in the percutaneous dilatational tracheostomy set begins. (Α) The tracheal dilator is carefully fed through the wire, creating an opening in the anterior tracheal wall. (B) The tracheostomy tube is placed under direct vision through the guidewire.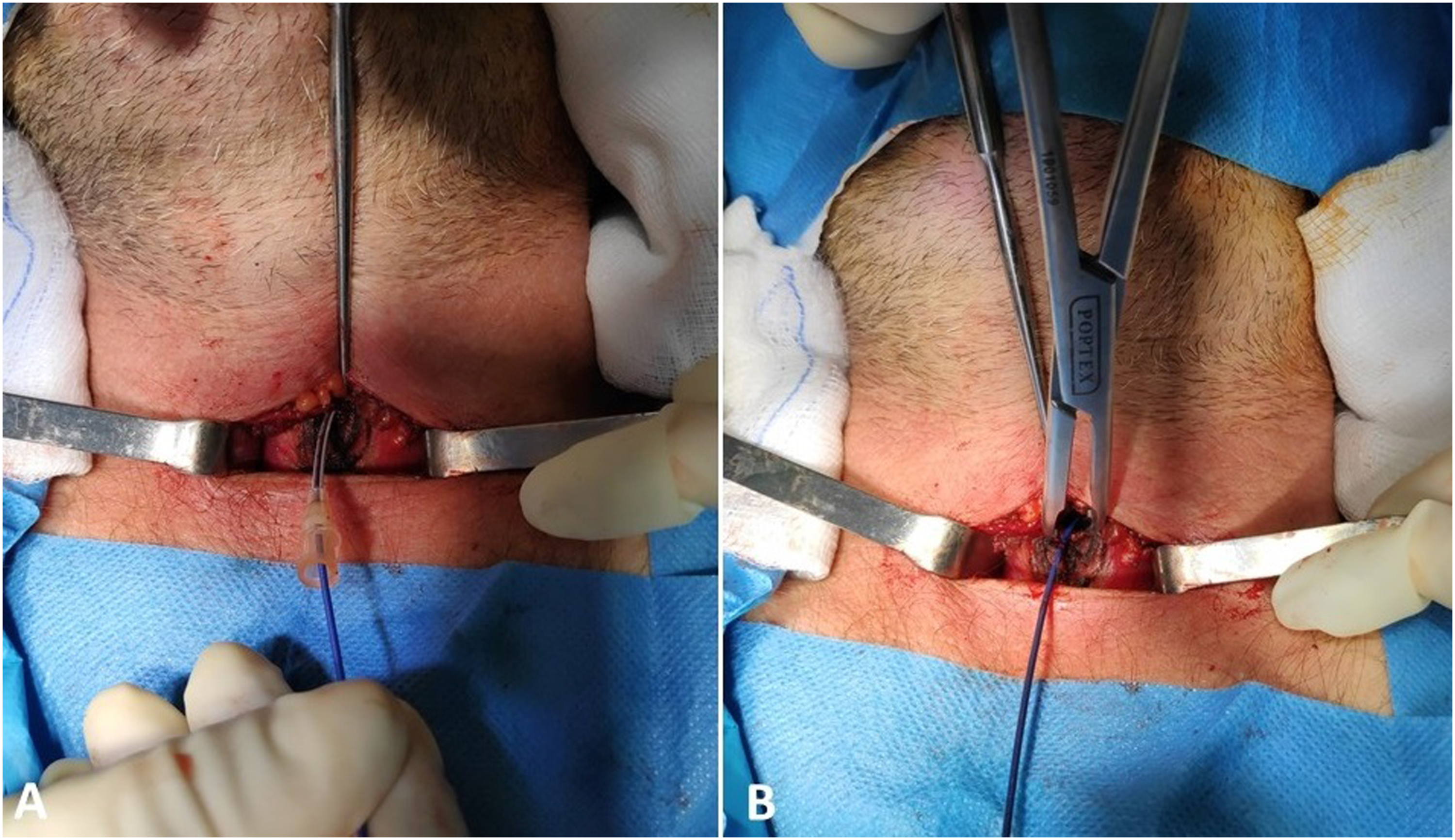
During the pandemic, 8–13% of COVID-19–positive patients were in need of a tracheotomy, 1 due to prolonged intubation or requirement of it, the majority of whom were obese with a difficult neck anatomy.2,3 In such patients, a percutaneous dilatational tracheostomy (PDT) could not be performed with adequate safety in the ICU, so they had to be transferred to the operating room for a surgical tracheotomy, a process that is time- and resource-consuming. 2 Furthermore, the availability of operating tables and personnel was limited due to the reformation of many of them as ICU rooms. Under these conditions, we devised a modified technique, which has been used in over 50 patients to this day, combining both approaches, with the scope to perform a tracheostomy safely at the bedside for more patients, without the need of an operating room. This technique incorporates the advantages of PDT and expands its indications while decreasing its limitations.
Comparing our method with the classic percutaneous and surgical approaches, it can be performed safely at the bedside without the need for a patient transfer. By using the modified Seldinger technique after the exposure of the trachea, the surgeons, as well as the whole ICU area, are less exposed to the patient’s expiratory aerosol that occurs during the tracheotomy.
Certain limitations exist regarding technical difficulties that might occur, which heavily depend on the experience of the surgeon (anatomical variants, presence of thyroid mass, cervical trauma, and previous operation at the insertion site). During the operation, the isthmus of the thyroid is never divided. In our experience, this step saves time and decreases the possibility of a post-surgical bleeding. However, we should mention that 2 out of the 52 patients that were operated via our method had post-operative hemorrhage on the third day and were transferred operated for hemostasis. Both patients had an enlarged thyroid, uncorrected coagulopathy, and the bleeding site was the isthmus. Like the PDT, our approach was not used in emergency situations, pediatric patients, or patients with a neck mass located medially. In those cases, a surgical tracheostomy was preferred.2,3 In case of a revision surgery due to complications, the open approach offers an easier surgical access. Finally, we observed a short healing time after the removal of the tracheostomy tube, similar to that of the PDT, usually without the need for a second operation.2-6
In conclusion, our modified approach is safe for patients with a short neck, with or without restricted neck extension, and morbid obesity, as well as in some cases of an enlarged thyroid, a neck mass, or prior neck operations.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Consent
We declare that written informed consent for patient information and images to be published was provided by the patient.