
Abstract
Hemangiomas account for only 0.4% to 0.6% of all parotid tumors, making them extremely rare in adults. Unlike pediatric parotid hemangiomas, those in adults typically present as asymptomatic swellings of the parotid, have no skin discoloration, and usually do not regress spontaneously. Therefore, an accurate diagnosis of parotid hemangiomas in adults before surgical excision is generally challenging. Herein, we present 3 cases of adult parotid hemangiomas. The patients all received parotidectomies with tumor resection. Histopathological analysis of the resected specimens revealed numerous dilated, thin- or thick-walled (small, large, or variably sized) vessels lined with flattened endothelial cells. A diagnosis of cavernous hemangioma of the parotid gland was established only after the histopathological analysis. Parotid cavernous hemangiomas in adults are rare and often misdiagnosed before surgical resection. Clinical presentation and imaging features on ultrasonography, computed tomography, magnetic resonance imaging, and angiography may support an accurate preoperative diagnosis. Surgical resection proved a suitable treatment approach for our 3 cases.
Introduction
Hemangiomas are benign tumors of vascular origin characterized by the increased proliferation and turnover of endothelial cells. Hemangiomas can occur anywhere on the body, but 65% are located in the head and neck region. 1 They mostly affect the salivary glands, with the parotid gland being the most common site (81%–85%). Hemangiomas account for only 0.4% to 0.6% of all tumors in the parotid gland.2-4 Parotid hemangiomas typically occur in children and account for approximately 50% of parotid tumors that develop in the first year of life. 3 Most parotid hemangiomas grow during a child’s first 6 to 8 months, followed by involution during the first decade of life. 5 By contrast, parotid hemangiomas in adults are quite rare3,4,6 and usually do not regress spontaneously. 3 In infants, hemangiomas typically manifest outwardly as reddish or purpuric skin lesions. In adults, asymptomatic swelling of the parotid gland occurs. 7 Therefore, an accurate diagnosis of parotid hemangiomas in adults before surgical excision tends to be challenging. Here, we present 3 cases of adult parotid hemangiomas to illustrate their clinical presentations, clinical courses, and outcomes.
Case Report
Case 1
A 48-year-old man with a history of asthma presented to our otolaryngology clinic with a 3-week history of swelling over the left side of the face. The swelling was not accompanied by pain and did not change in size during meals or during bending or straining movements. On physical examination, a mass was palpated over the left infra-auricular area. The mass was elastic, nontender, nonfluctuating, and nonpulsatile, and the overlying skin was normal in color, texture, and temperature. We did not detect any palpable mass over the right parotid area or any associated cervical adenopathy. Intraoral examination revealed a normal parotid duct (Stensen’s duct) opening. No pus was released from the orifice after massage.
Ultrasonography indicated a hypoechoic, well-defined tumor measuring approximately 3.0 × 1.7 × 1.3 cm3 over the parotid tail. A diagnosis was not possible after fine-needle aspiration (FNA) because of the negligible observed cellularity. Computed tomography (CT) revealed a well-defined lobular nodule with mild enhancement in the parotid gland (Figure 1). A parotidectomy with tumor excision was performed. During the surgery, a well-defined, dark red tumor was noted in the deep lobe of the parotid gland, with adhesion to the cervical branch of the facial nerve (Figure 2). (Case 1) (A) Noncontrast CT image (axial view): a 2.1 cm, well-defined, lobular mass in the left parotid gland. (B) Contrast-enhanced CT image (axial view): mild enhancement (white arrow). (Case 1) Surgical specimen: a well-defined, dark red tumor (white arrow) in the deep lobe of the left parotid gland, measuring 3.2 × 2.2 × 1.5 cm3.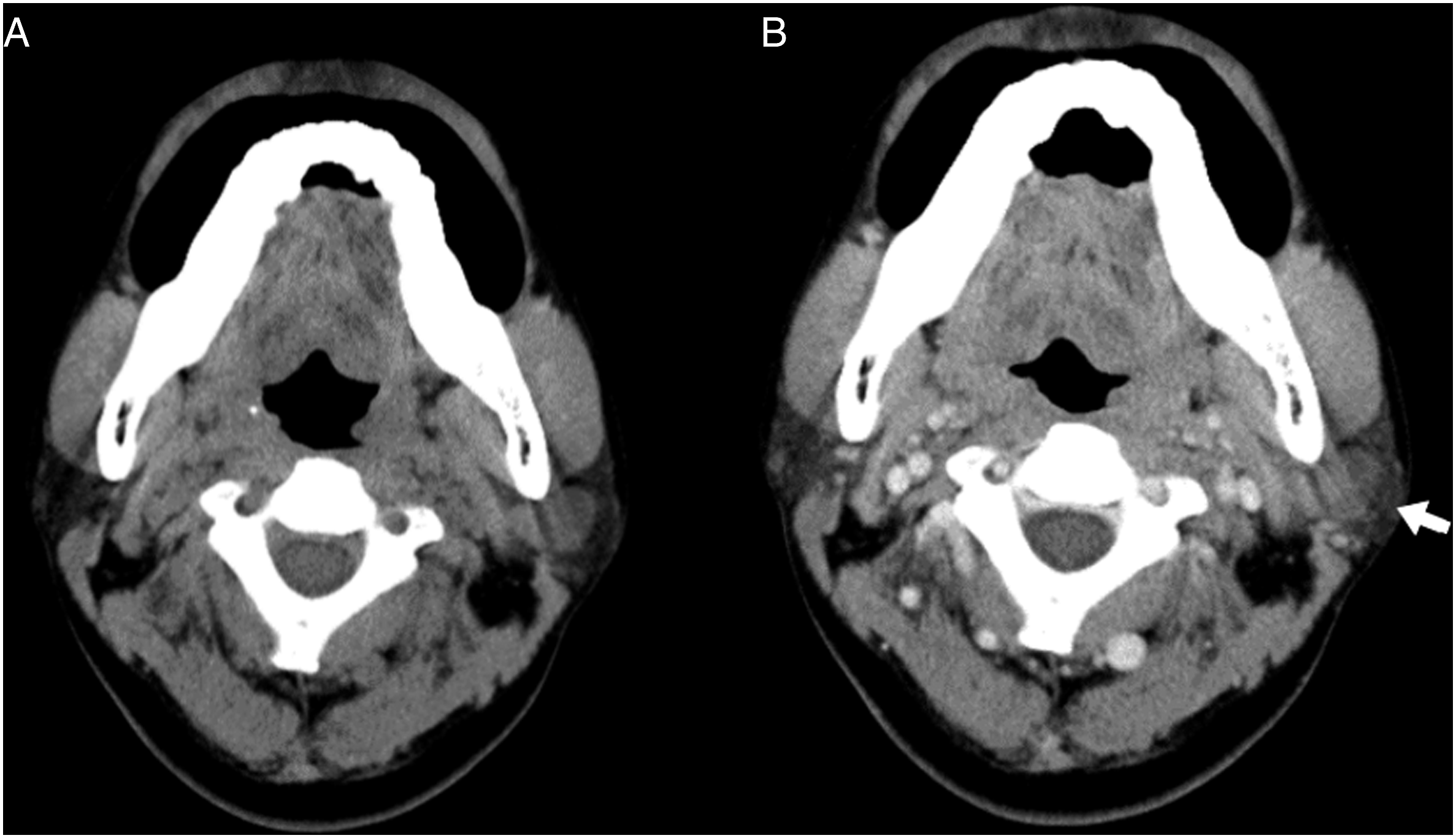

Under a microscope, the lesion was composed of numerous dilated, thick-walled vessels of various sizes in dense collagenous stroma and lined with flattened endothelial cells (Figures 3A and 3B). Verhoeff–Van Gieson stain revealed no connection between the arteriole and vein or elastic membrane. The vascular spaces were lined with CD31-positive endothelial cells. Moreover, the peripheral parotid tissue was unremarkable, with no evidence of malignancy (Figures 3C and 3D). The postoperative period was uneventful, and the patient was followed up for 3 months. (Case 1) (A) (B) Histopathology of the tumor is composed of numerous dilated, thick-walled vessels of varying sizes surrounded by dense collagenous stroma (H&E 10X). (C) The vascular spaces were lined by CD31-positive endothelial cells (CD31 40×). (D) Neither elastic membrane nor connection between arteriole and vein is detected by Verhoeff–Van Gieson stain (VVG 10×).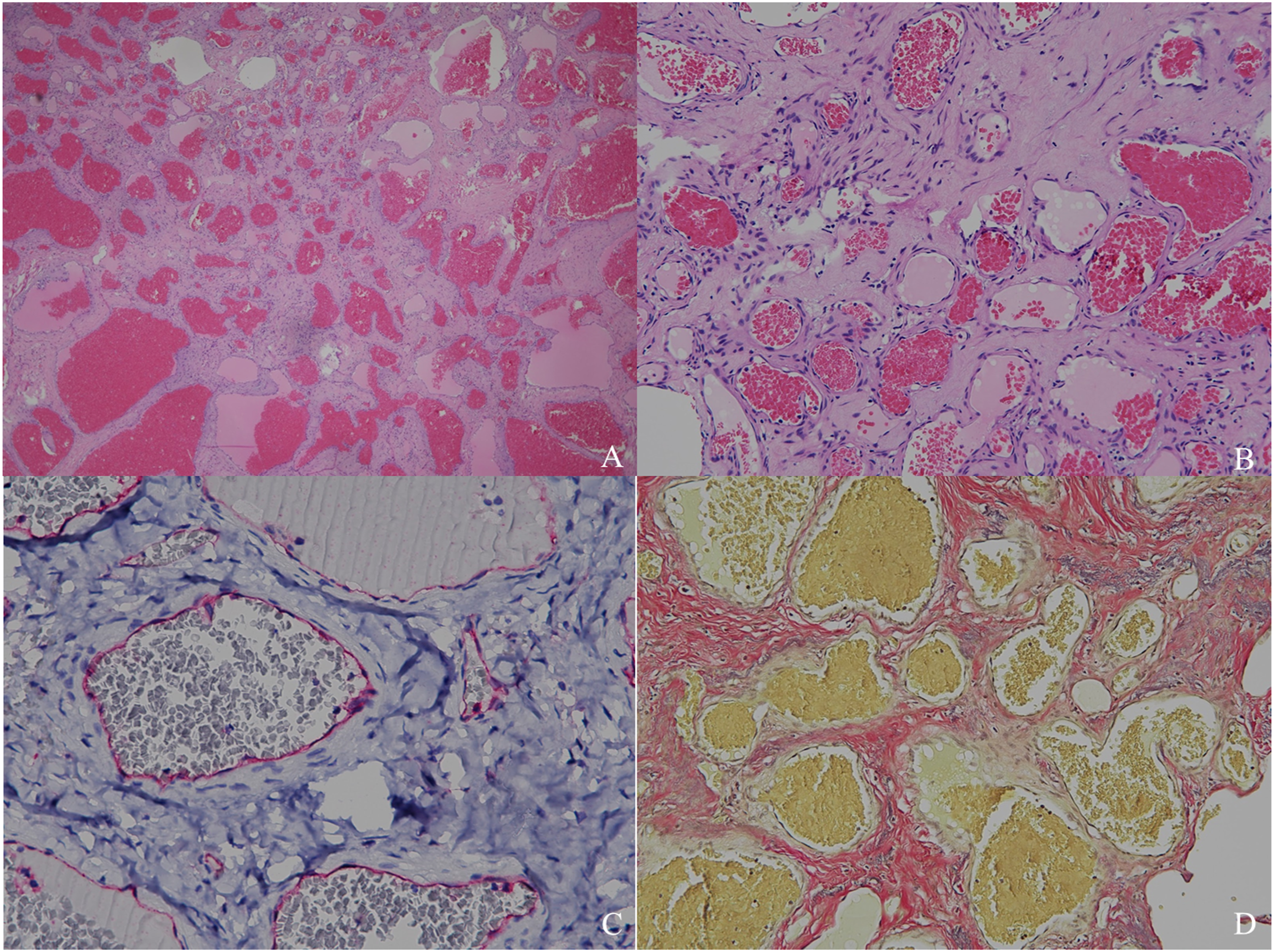
Case 2
A 61-year-old woman visited our otolaryngology clinic for an examination of an incidental left preauricular mass detected by magnetic resonance imaging (MRI). She eventually developed mild tenderness over the mass. No postprandial pain or swelling was observed. A clinical examination revealed an elastic, tender, mobile mass measuring approximately 3.0 × 2.5 cm2 without skin changes in the left preauricular area. MRI of the head and neck revealed a lobulated tumor that was T2 isointense. Mild and heterogeneous enhancement after intravenous contrast administration, without extension to adjacent structures, was noted (Figure 4). (Case 2) (A) Contrast-enhanced T1-weighted MRI image (coronal view): Lobulated parotid mass with mild and heterogeneous enhancement (white arrow). (B) Contrast-enhanced T2-weighted MRI image (coronal view): isointense mass.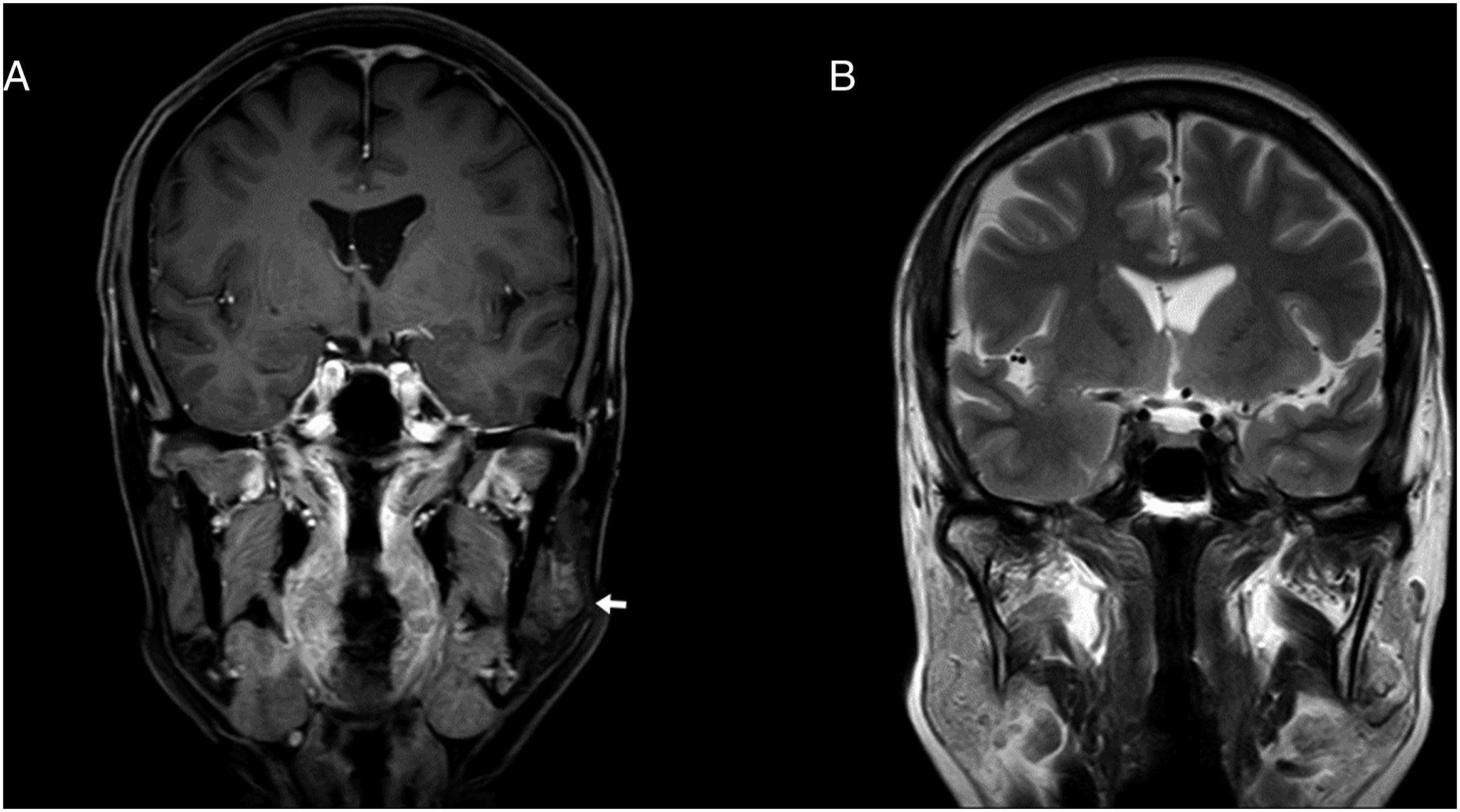
A partial parotidectomy with facial nerve preservation was performed. Intraoperatively, a cystic tumor located in the deep lobe of the left parotid gland was observed. The tumor was gray-brown in color and firm to the touch. A histopathological examination of the specimen revealed numerous dilated thin-walled vessels lined with flattened endothelial cells that were highlighted through CD34 staining. These results suggested a cavernous hemangioma of the parotid gland. The patient was followed up for 3 months and remained asymptomatic throughout that period.
Case 3
A 22-year-old man presented with a 2-year history of a right infra-auricular mass. The mass had slowly increased in size and become tender. Head and neck CT revealed a 4 cm, lobulated, well-defined, and hyperdense mass with faint enhancement in the parotid gland.
After the patient received antibiotic treatment and hydration for 10 days, the symptoms of acute parotitis were completely resolved. A partial parotidectomy with tumor excision was then performed. Microscopic examination of the specimen revealed a tumor composed of numerous small vessels lined by flat endothelial cells in healthy parotid gland tissue. The final diagnosis was a cavernous hemangioma. The patient recovered, and no recurrence was noted after a follow-up period of 3 months.
Discussion
Hemangiomas are benign and congenital neoplasms of vessels, and they are characterized by 3 stages: endothelial cell proliferation, rapid growth, and spontaneous involution. Their pathophysiology includes various genetic and cellular factors, particularly monocytes, which are considered potential ancestors of endothelial cells in hemangiomas. An imbalance in angiogenesis, which causes the uncontrolled proliferation of vascular elements associated with substances such as vascular endothelial growth factor (VEGF), basic fibroblast growth factor, and indoleamine 2,3-dioxygenase, is believed to be the origin.8,9 Hemangiomas are the most common type of tumor that develops in infancy. They appear more often in female patients than in male patients and may fluctuate in size with pregnancy and menarche, suggesting that the endothelial cells may be responsive to circulating hormones. 1 Hemangiomas of the major salivary glands, especially the parotid gland, are common in the pediatric population, with 90% of cases developing within the first 3 decades of life. They are the most common lesions of the major salivary glands that develop during infancy and early childhood.
In adults, hemangiomas are extremely rare presentations of a parotid mass. The World Health Organization Classification of Tumours, published in 2005, states that only approximately 50 cases had been noted globally, mostly as case reports.1,7 No data exist on the recent prevalence of parotid hemangiomas in adults, and the cavernous type is the only one described thus far. 10 Conventionally, parotid hemangiomas can be histologically classified as capillary, cavernous, or mixed. 2 Capillary hemangiomas contain many small capillaries lined with a single layer of endothelial cells supported in a connective tissue stroma of variable density. Cavernous hemangiomas consist of large, thin-walled vessels lined with epithelial cells separated by a thin layer of connective tissue septa. 8 Both capillary and cavernous hemangiomas develop in children, whereas only cavernous hemangiomas have been reported in adults. 10 Nagao et al. presented a series of 20 cases of cavernous hemangiomas of the parotid gland. The mean patient age was 26 years. 11 Cavernous hemangiomas typically grow slowly and remain asymptomatic for long periods of time until sudden growth induces pain or cosmetic concerns.1,7,12 Bluish discoloration of the skin in patients with cavernous hemangiomas is extremely rare. In adults, pleomorphic adenoma and Warthin tumors are the most common benign tumors of the salivary glands. 7 Because of their rarity, a diagnosis of parotid hemangiomas based on clinical assessment and imaging results in adults is challenging.7,12
Ultrasonography is an essential imaging modality for salivary gland tumors.7,13 Parotid hemangiomas are commonly characterized by well-defined borders and heterogeneous or homogeneous echogenicity. 14 Moreover, their greyscale sonographic appearance is nonspecific. 15 The detection of blood vessels in hemangiomas may be difficult. Color-coded duplex sonography detects only blood flow and not the extent of vascularity. Nevertheless, duplex ultrasonography is an essential part of the examination, and the examiner should endeavor to detect as many intratumoral vessels as possible. 16 CT scans assist doctors with locating parotid tumors and determining their relationships with adjacent structures. The typical CT imaging feature of a parotid hemangioma is an enhanced, well-circumscribed, lobulated parotid mass with homogeneous density. MRI is useful in evaluating parotid hemangiomas and their extensions.17,18 On an MRI image, parotid hemangiomas typically appear as well-defined, lobulated, and homogeneously enhancing lesions with homogeneous T1 hypointensity and T2 hyperintensity with variable vascularity. The lesions may appear heterogeneous when small focal areas of fat replacement are present.3,10 FNA is useful in the preoperative diagnosis of tumors of the head and neck. 19 However, FNA or core needle biopsy in hemangiomas primarily yield blood products and are unlikely to provide sufficient tissue for histologic analysis. 20 Therefore, FNA should be avoided when a vascular lesion is suspected to avoid iatrogenically induced hematoma.3,7,21 Angiography is the gold standard modality for the diagnosis of arteriovenous malformation, but it is not routinely performed to diagnose hemangiomas. However, it may be useful when prominent feeding arteries are present.14,22
Parotid cavernous hemangiomas in adults do not regress, necessitating complete surgical resection. In most cases, parotid hemangiomas are diagnosed after histopathological examinations of the parotidectomy specimen. If the hemangioma is large, magnetic resonance angiography or intra-arterial digital subtraction angiography should be performed preoperatively to investigate the vascular supply of the tumor. Preoperative transarterial embolization is advisable in large and well-vascularized tumors to reduce tumor size and intraoperative bleeding. 23 For infantile hemangiomas, other nonsurgical treatments have been developed, including endovascular sclerotherapy and the administration of vincristine, propranolol, or intralesional or systemic corticosteroids. However, the effectiveness of these treatments for cavernous hemangiomas remains unclear.7,24,25 Therefore, nonsurgical treatments are recommended only when surgery is contraindicated or refused. 26
Cavernous hemangiomas histologically appear as blood-filled vascular channels of varying sizes. The vessels are lined with flattened endothelial cells without atypia and with a thin wall supported by a dense collagen layer.7,27 In one study, hemangiomas displayed increased endothelial cell proliferation and angiogenesis under immunohistochemistry (IHC) staining. Overall, IHC assessment confirmed the typical indicators of vascular neoplasm, namely, the increased expression of VEGF and Ki-67. 28 Moreover, in those with hemangiomas, endothelial markers, such as CD31, CD34, ERG, FLI1, and factor VIII, are strongly positive. Hemangiomas are negative for D2-40, a selective endothelial marker. 29
Conclusion
Parotid hemangiomas in adults are rare and are often misdiagnosed before surgical resection. Clinical presentations and images from sonography, CT, MRI, and angiography can enhance diagnostic accuracy. Surgical resection yielded favorable outcomes for our 3 patients.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.