
Abstract
Introduction
Otosclerosis is a disease of the temporal bone, responsible for 5–9% of all hearing loss cases. The disease develops within the bony labyrinth. Impaired metabolism causes the initial softening of the osseous tissue, followed by secondary pathological sclerosis. The disease progression usually affects the anterior niche of the oval window (fissula ante fenestram). Consequently, the base of the stapes becomes fixed, impairing the transmission of sound waves from the middle ear through the chain of ossicles to the inner ear. Conductive hearing loss is usually observed during the initial phase of the disease. However, as the disease progresses, the sensorineural component becomes evident as well. Sensorineural hearing loss (SNHL) is also observed in cochlear otosclerosis when otosclerotic foci develop within the cochlea. 1
The basic tool for diagnosis and control of otosclerotic treatment is an audiometric examination. The pure-tone audiometry (PTA) graph presents an image specific to conductive hearing loss. A pure-tone audiometry shows the sensorinural hearing loss with respect to cochlear otosclerosis. 2,3
Under normal conditions, the basic route of conduction for an acoustic wave to the receptor is air. Bone conduction (BC), a component of normal hearing, is referred to as indirect conduction and constitutes a weaker acoustic stimulus compared to air conduction.
The bone conduction threshold in otosclerosis can be affected by the presence of otosclerotic foci in the osseous capsule of the cochlea and the related progressing impairment of the sensorineural apparatus, Carhart’s effect, which is associated with the fixed base of the stapes in the oval window, as well as by mechanical or acoustic trauma during a surgery.
Carhart’s notch as observed in pure-tone audiometry was described for the first time in 1950 by Raymond Carhart, and defined as a 10–20 dB increase in the bone conduction threshold for the frequency of 2000 Hz. Based on many years of observations, a similar-looking notch may occur in the frequency range of 500–3000 Hz in the course of other middle ear disorders that limit the motion of the chain of auditory ossicles. These disorders include secretory otitis media, tympanosclerosis, or auditory ossicle malformations. The notch observed for the frequency of 2000 Hz seems to occur as a result of increased impedance in the oval window. According to a theory by Stenfelt et al., the presence of Carhart’s notch at 2000 Hz in otosclerosis links the changed bone conduction for this frequency with the otosclerotic process occurring in the niche of the oval window. 4,5
In literature, the incidence of Carhart’s notch in patients with otosclerosis ranges from 31% to 80% of cases. 6 The aim of the study is an audiometric assessment of the effectiveness of surgical treatment of otosclerosis depending on the preoperative incidence of Carhart’s notch.
Materials and methods
The analysis included 116 patients treated surgically for the first time due to otosclerosis between 2015 and 2018. Longitudinal retrospective interventional nonrandomized cohort study was performed. The patients were operated on at one site by surgeons with similar experience, using the same surgical technique. The patients who qualified for the study were 70 women aged 18 to 60 years and 46 men aged 27 to 57 years. The average age of the study participants was 40.87 years.
Criteria for inclusion in study: the first surgery due to otosclerosis, no congenital defects, no head injury in the patient’s history, and over 18 years old. Criteria for exclusion from the study: reoperation, congenital defects of the ear, head injury in the patient’s history, and under 18 years of age.
All patients gave their informed consent to the treatment and the participation in the study. The study was approved by the Bioethics Committee.
Before surgical treatment and 36 months afterward, each patient underwent a medical interview, an otoscopic examination, and an audiological evaluation consisting of the whispered voice test, the tuning fork tests, pure-tone audiometry, speech audiometry, and impedance audiometry.
Stapedotomy was the chosen surgical technique to treat otosclerosis for 104 patients due to the progression of the disease, whereas stapedectomy was necessary in 12 cases.
The audiometric tests were carried out in the soundproof and sound-absorbing cabin of the audiometric laboratory. Data obtained in the audiometric examination were prepared in accordance with the guidelines of the Committee on Hearing and Equilibrium American Academy of Otolaryngology–Head and Neck Surgery. 7
Polish speech testing was carried out using testing material which comprised of 10 balanced lists, each consisting of 24 one-syllable nouns. The test was balanced acoustically, grammatically, phonematically, semantically, energetically, and structurally.
Division of patients included to the study based on presence and absence of the Carhart’s notch in the established groups.
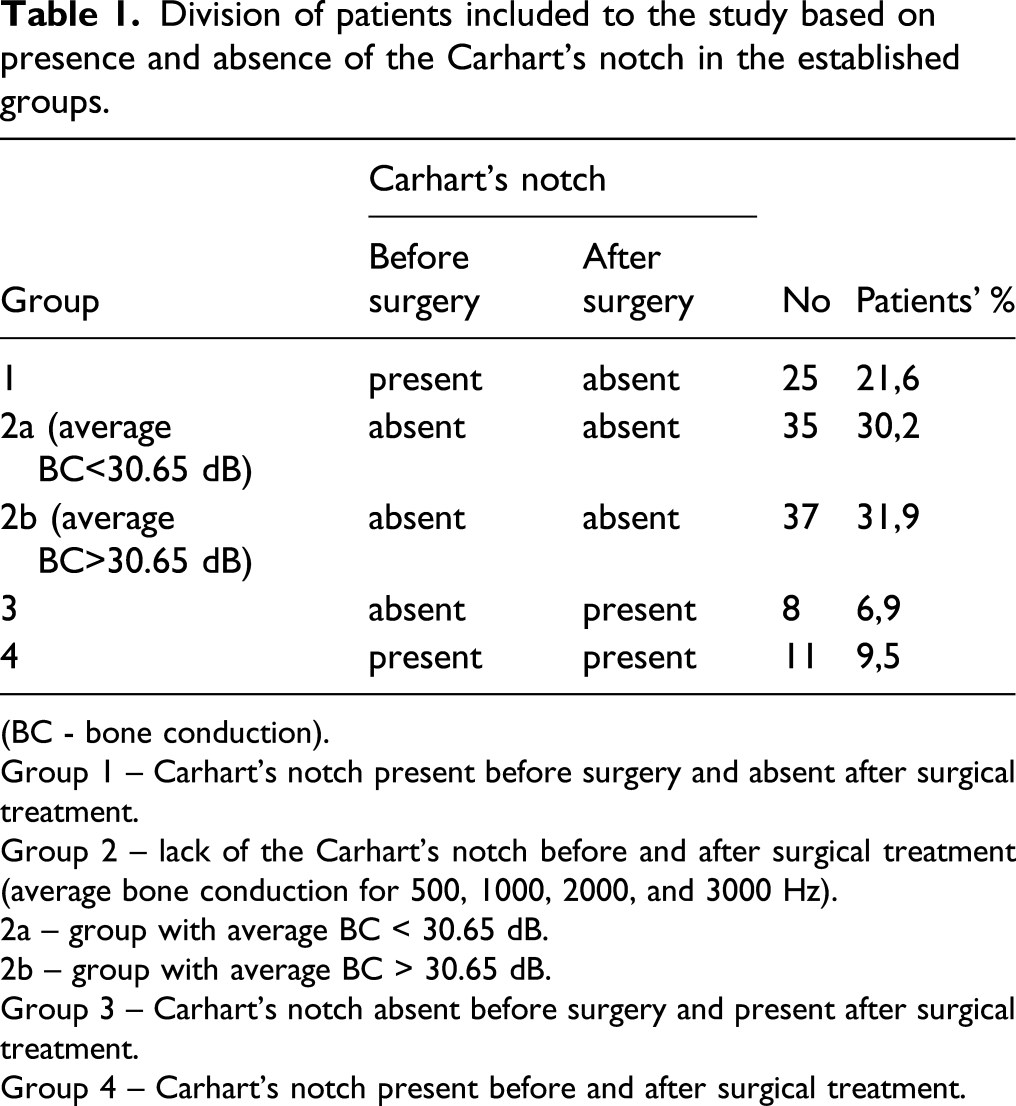
(BC - bone conduction).
Group 1 – Carhart’s notch present before surgery and absent after surgical treatment.
Group 2 – lack of the Carhart’s notch before and after surgical treatment (average bone conduction for 500, 1000, 2000, and 3000 Hz).
2a – group with average BC < 30.65 dB.
2b – group with average BC > 30.65 dB.
Group 3 – Carhart’s notch absent before surgery and present after surgical treatment.
Group 4 – Carhart’s notch present before and after surgical treatment.
Considering all the analyzed patients with preoperative Carhart’s notch presence, it was calculated that in these patients the mean value of bone conduction thresholds at 500 Hz, 1000 Hz, 2000 Hz, and 3000 Hz was 30.65 dB.
Assessing the impact of the performed surgical treatment on the improvement of hearing in PTA and speech audiometry, this value of bone conduction thresholds was a reference point for further analysis in patients who had no preoperative or postoperative Carhart’s notch. On this basis, the division of patients from group 2 (in which no Carhart’s notch was found both before and after surgery) was made into two subgroups with average bone conduction < 30.65 dB and with average bone conduction > 30.65 dB.
The groups are divided as follows: Group 1 (N = 25 patients) – Carhart’s notch present preoperatively and absent postoperatively. Group 2 (N = 72 patients) – Carhart’s notch absent pre- and postoperatively. 2a (N = 35 patients) – Group with average BC < 30.65 dB. 2b (N = 37 patients) – Group with average BC > 30.65 dB. Group 3(N = 8 patients) – Carhart’s notch absent preoperatively and present postoperatively. Group 4(N = 11 patients) – Carhart’s notch present pre- and postoperatively.
The audiometric test results obtained in the relevant time interval were subject to analysis. Changes in the average air-bone gap (ABG); changes in the bone conduction values for the frequencies 500 Hz, 1000 Hz, 2000 Hz, and 3000 Hz; and changes in speech comprehension after surgical treatment were determined.
Preoperative results and results obtained at 36 months post-surgery were subject to a statistical analysis. The result analysis was carried out using the STATISTICA 13 suite (StatSoft Polska, Kraków, Poland). Chi-squared test, Pearson’s linear correlation, Student’s t-test, and one-way analysis of variance with small group adjustments were used. Statistically significant results of the variance analysis were examined post hoc using Tukey’s test. Statistical significance was established at P < 0.05.
Results
Variances’ analysis of average bone conduction thresholds before surgical treatment in the established groups.
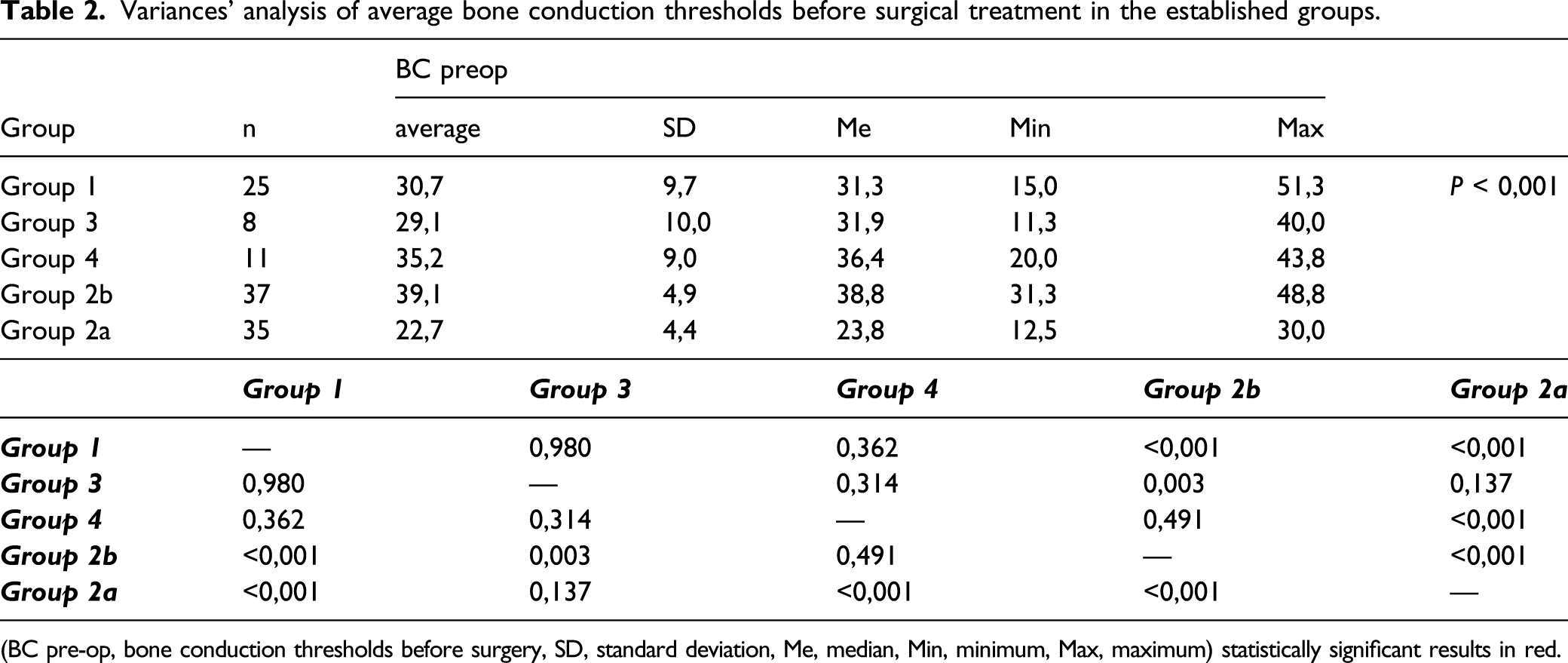
(BC pre-op, bone conduction thresholds before surgery, SD, standard deviation, Me, median, Min, minimum, Max, maximum) statistically significant results in red.
Variances' analysis of average bone conduction thresholds after surgical treatment in the established groups.
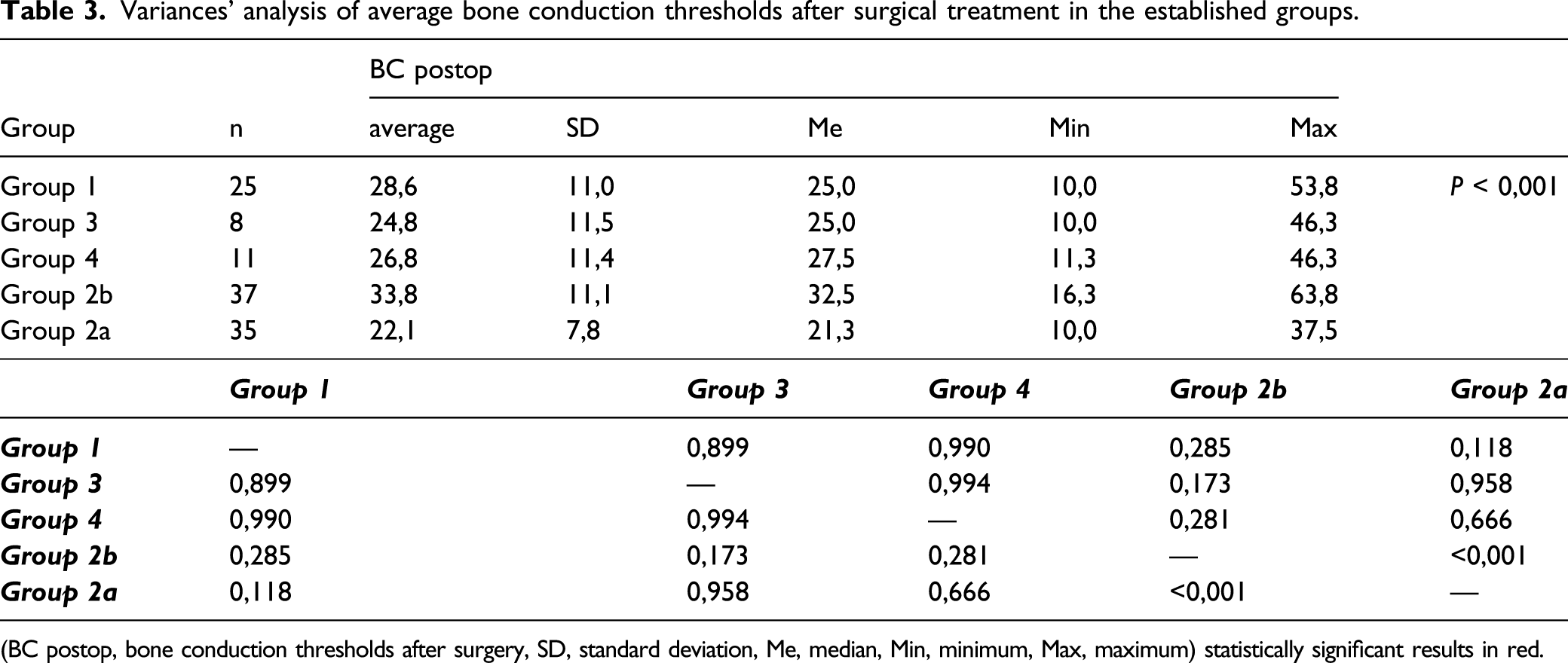
(BC postop, bone conduction thresholds after surgery, SD, standard deviation, Me, median, Min, minimum, Max, maximum) statistically significant results in red.
Variances’ analysis of average air-bone gap before surgical treatment in the established groups.
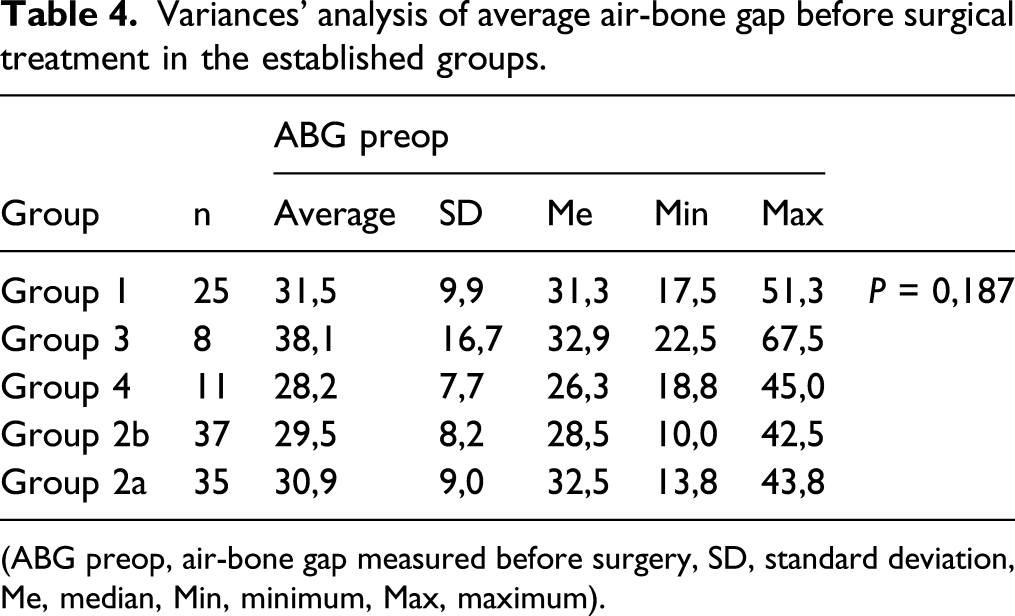
(ABG preop, air-bone gap measured before surgery, SD, standard deviation, Me, median, Min, minimum, Max, maximum).
Variances' analysis of average air-bone gap after surgical treatment in the established groups.
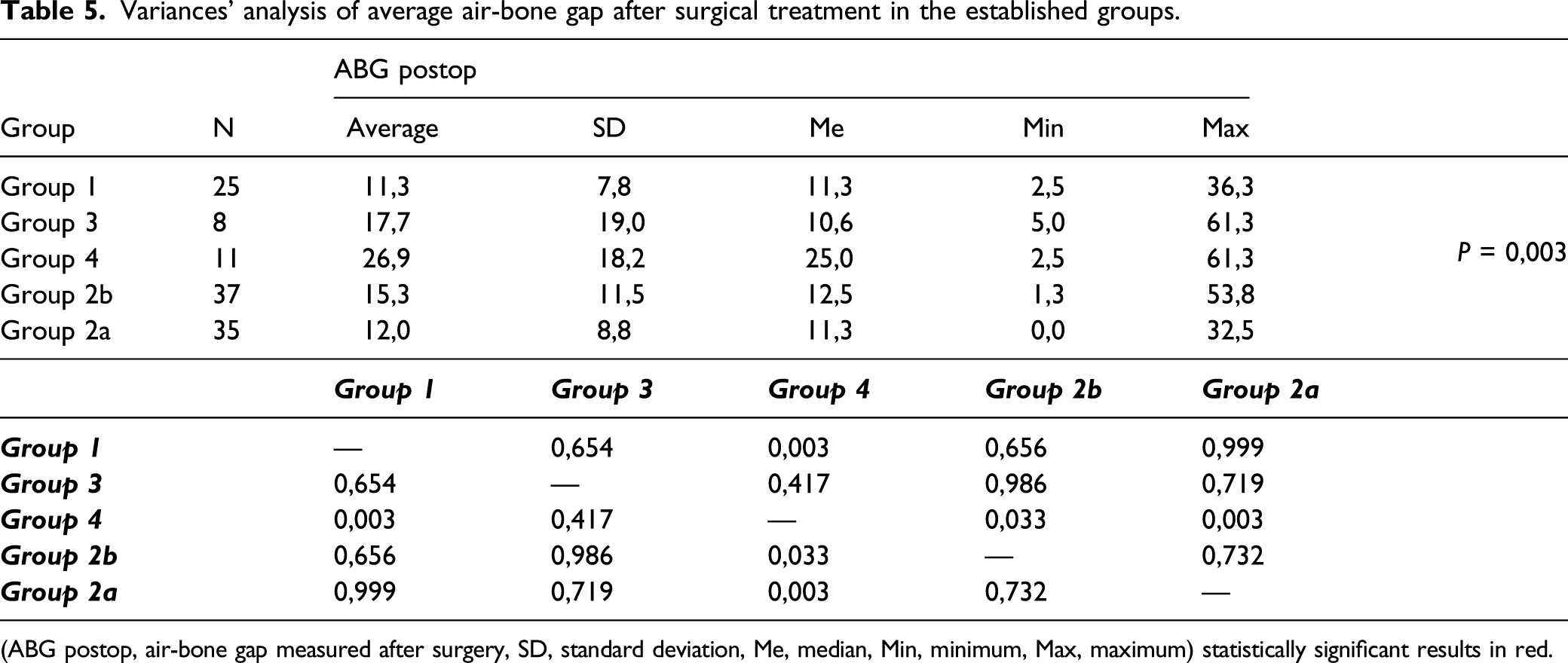
(ABG postop, air-bone gap measured after surgery, SD, standard deviation, Me, median, Min, minimum, Max, maximum) statistically significant results in red.
Based on the above data, by examining the groups’ average pre- and postoperative ABG in the operated ear, it was found that the presence of Carhart’s notch over a longer observation has adverse effects on the size of the postoperative ABG, and consequently on hearing improvement after surgical treatment.
Change in air-bone gap before and after surgical treatment in the established groups on the 2000 Hz frequency.
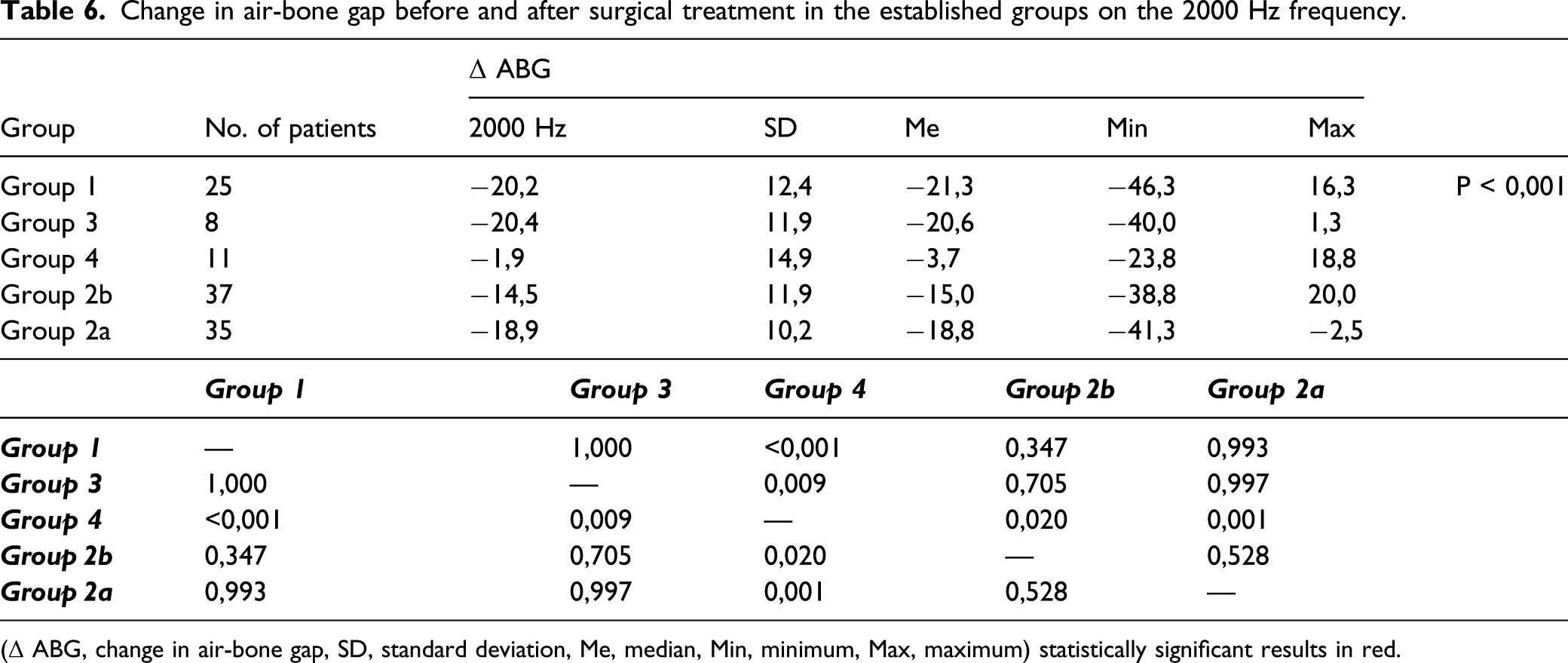
(Δ ABG, change in air-bone gap, SD, standard deviation, Me, median, Min, minimum, Max, maximum) statistically significant results in red.
Variances’ analysis of the sound pressure level necessary to achieve 100% speech understanding before surgery in the established groups.
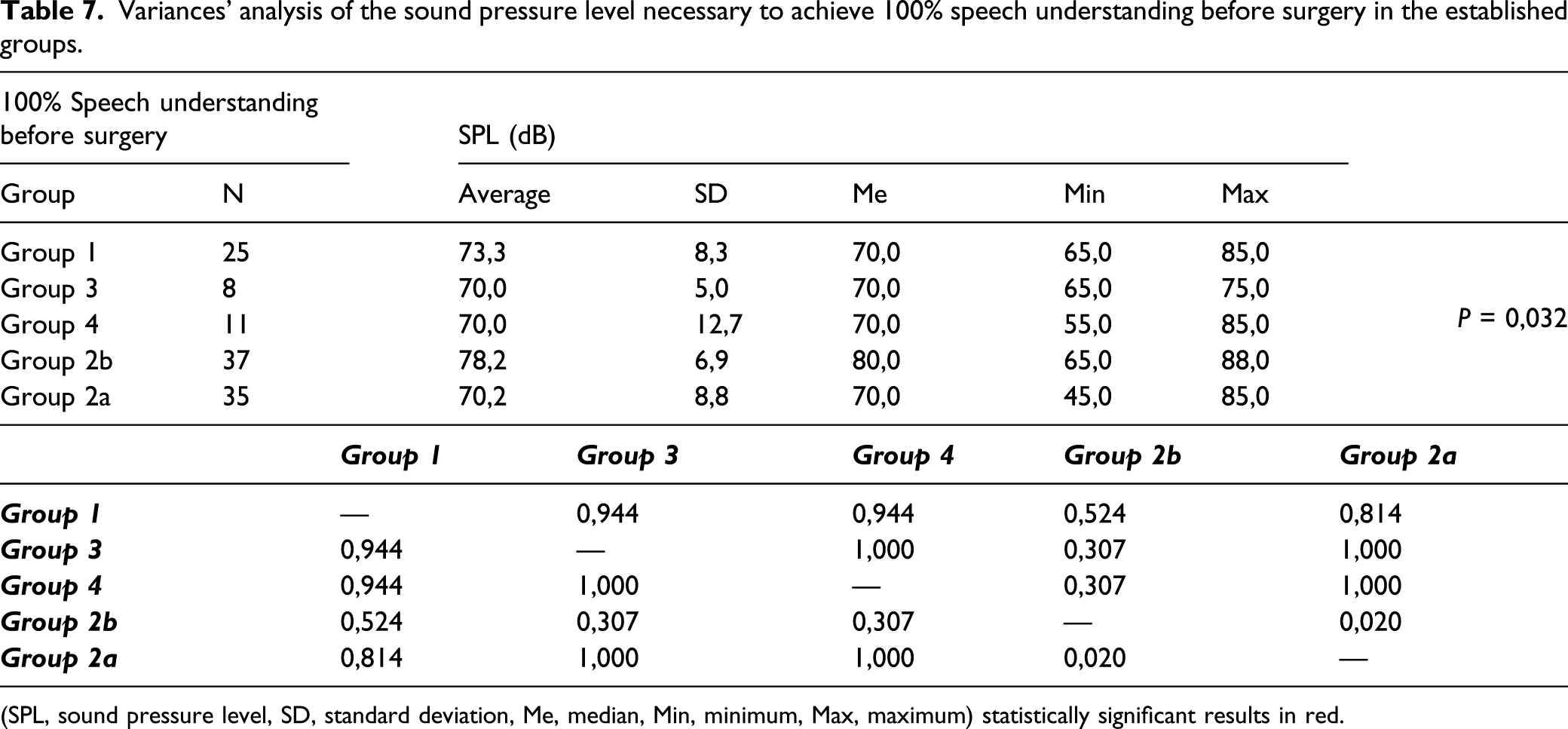
(SPL, sound pressure level, SD, standard deviation, Me, median, Min, minimum, Max, maximum) statistically significant results in red.
Variances’ analysis of the sound pressure level necessary to achieve 100% speech understanding after surgery in the established groups.
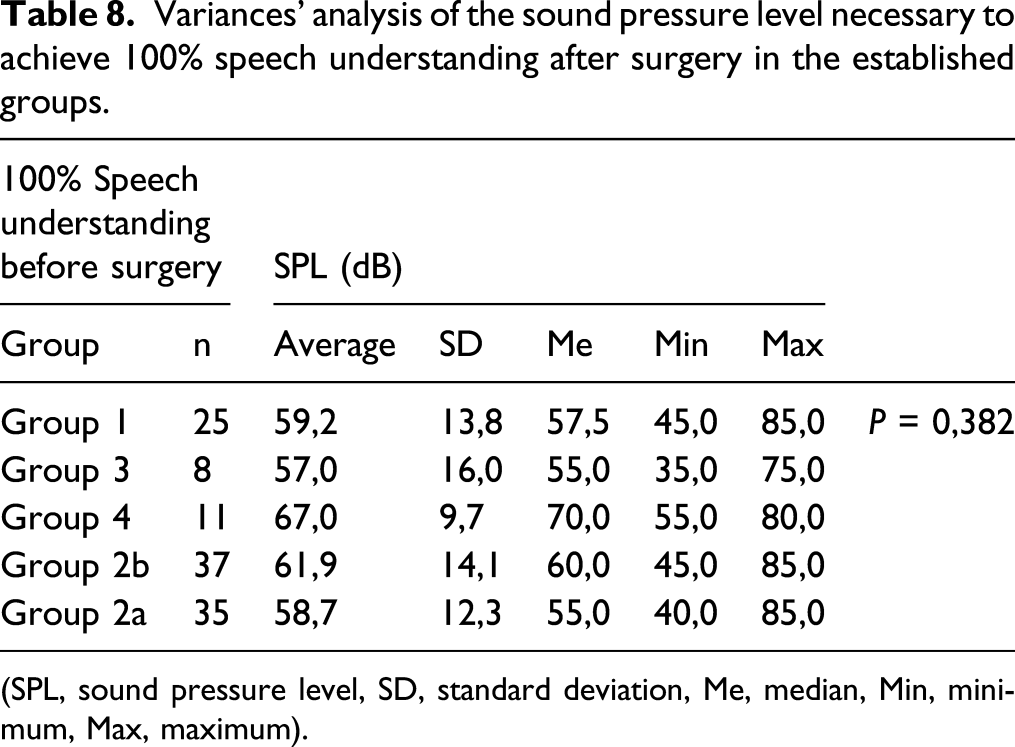
(SPL, sound pressure level, SD, standard deviation, Me, median, Min, minimum, Max, maximum).
Discussion
Improved hearing is one of the main goals of the surgical treatment of otosclerosis. It is considered from the perspective of closing the air-bone gap and improving bone conduction and speech comprehension.
Numerous publications discuss the influence of Carhart’s notch observed preoperatively on hearing improvement prognoses. Lamblin et al. 6 indicate that this notch, observed in preoperative pure-tone audiometry is an unfavorable factor when it comes to bone conduction improvement prognoses. Sabbe et al. 8 emphasize that the best bone conduction improvement after stapedotomy is observed at the resonance frequency of the chain of auditory ossicles (2000 Hz). As a result of the above correlation, a statistically significant change is observed in bone conduction in the group with Cahart’s notch, compared to patients without Cahart’s notch in pure-tone audiometry before surgical treatment. The analysis indicated Cahart’s notch in preoperative pure-tone audiometry as a statistically significant improvement factor for average bone conduction. In the analysis of the value of bone conduction assessed postoperatively, a statistically significant difference was found between the groups with preoperative Carhart’s notch (group 1 and group 4) and groups without Carhart’s notch (group 2 and group 3). The above data indicate that over a longer perspective (such as the 3 years of observation as a part of this study), a statistically significant improvement of bone conduction occurred in patients without postoperative Carhart’s notch.
The effects of middle ear surgery on the function of the inner ear and speech comprehension improvement have been discussed for a long time. 9,10 Surgical treatment improves patients’ quality of life and speech audiometry results. A finding discovered in this study is that speech comprehension improves in patients with preoperative Carhart’s notch and that the same does not happen in the case of persistent Carhart’s notch after surgical treatment. The most important component when it comes to speech comprehension is improved bone conduction up to 3000 Hz; higher frequencies contribute to sound quality. 11 -13
A comparison between patients from the two groups without preoperative Carhart’s notch found that when it comes to high-level sensorineural hearing loss (according to the criteria used for the analyzed group–above 30.65 dB), no beneficial effects of the surgery on speech comprehension were observed. Deep sensorineural hearing loss (group 2b) observed before surgical treatment in patients without Carhart’s notch led to worse speech comprehension compared to the group with better inner ear function but without Carhart’s notch.
A statistically significant improvement in speech comprehension was observed in the cases of lower-level sensorineural hearing loss without Carhart’s notch determined by preoperative PTA, as well as in patients with preoperative Carhart’s notch determined by PTA that disappeared after surgical treatment.
The analysis of the effects of Carhart’s notch on maintaining the air-bone gap after a surgery as part of the 36-month observation in the groups found that the presence of Carhart’s notch has adverse effects on the size of postoperative air-bone gap, and consequently the postoperative hearing improvement as well.
Persistent Carhart’s notch turned out to be a bad prognostic factor for closing the air-bone gap after surgical treatment in patients with otosclerosis (P < 0.001). The above correlation is consistent with the findings of other authors. 14 -17
No hearing improvement in postoperative patients with otosclerosis accounts for approximately 10% of all cases in literature. In this study, group 4, which had the worst result for air-bone gap closure and required an auditory stimulus of the highest intensity to achieve 100% in speech audiometry, accounted for 9.48% of all the study subjects. This result is consistent with the data available in the literature. Persistent Carhart’s notch, which was maintained for 36 months after the surgery, therefore had adverse effects on the air-bone gap change (P < 0.001), and consequently on postoperative hearing improvement.
The air-bone gap getting reduced below 20 dB in the subjects of the study is consistent with the findings of other authors (Szymański 2002 – more than 90% achieved air-bone gap reduction to below 20 dB; Sommers 1994 – air-bone gap was reduced below 20 dB in 94% of the patients). 2,3 In this study, an equivalent result was obtained in 90.5% of the subjects.
Conclusions
In a long-term observation post-stapedotomy, average bone conduction values improve. Nevertheless, the improvement is less evident in patients with preoperative Carhart’s notch. The disappearance of Cahart’s notch after surgical treatment of otosclerosis is a good prognosis for improvement in speech audiometry. Deep sensorineural hearing loss in the absence of Carhart’s notch in PTA constitutes a bad prognostic factor for improvement in speech audiometry in patients qualified for surgical treatment of otosclerosis.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Financial disclosure
This research was supported by statutory funds of the Department of Otolaryngology of the Jagiellonian University, Krakow, Poland.