
Abstract
Pulsatile tinnitus (PT) caused by a high-riding dehiscence jugular bulb (HDJB) is a rare but treatable otology disease. There are several managements include transcatheter endovascular coil embolization, transvenous stent–assisted coil embolization, or resurfacing the dehiscent bony wall of high jugular bulb under the use of microscope. Among those options, surgical resurfacing of HDJB might be an effective and safe choice with less destruction. However, previous studies approached middle ear cavity via microscope can only provide a lateral, indirect view, while resurfacing the vessel through a transcanal endoscopic ear surgery (TEES) approach may give surgeon a direct and easy way to manage HDJB. In this report, we presented a case of 40-year-old woman with HDJB and shared our clinical consideration and reasoning of the surgical management of PT via a transtympanic approach by TEES rather than a transmastoid approach.
Introduction
Pulsatile tinnitus caused by a high-riding dehiscence jugular bulb (HDJB) is rare and has been successfully treated either by endovascular approaches 1 or by resurfacing the dehiscent bony wall of high jugular bulb with bone cement, thus reinforcing the dehiscent jugular bulb and reducing focal turbulent flow. 2 However, there is lack of reports on resurfacing the vessel through a transcanal endoscopic ear surgery (TEES) approach.
In this report, we share our experience with and reasoning behind the surgical management of pulsatile tinnitus caused by a HDJB via a transtympanic approach by TEES rather than a transmastoid approach.
Case Presentation
A 40-year-old healthy female patient presented with a complaint of right pulsatile tinnitus for 5 years. The sound progressively became apparent during insomnia or fatigue and decreased during high-intensity exercise, with better sleep, or compression of the right side of the neck.
Otoscope, audiogram, and impedance testing appeared normal. Temporal bone magnetic resonance imaging with angiography showed no imaging evidence of a brain tumor, and there was normal blood flow bilaterally in the sigmoid sinuses, jugular bulbs, and jugular veins. Minimal carotid atherosclerosis without significant hemodynamic changes was found through a carotid ultrasound. Temporal bone computed tomography (CT) clearly demonstrated a right high-riding and dehiscent jugular bulb protruding into the mesotympanum (Figures 1A, 1B). Computed tomographic and clinical images (A) coronal and (B) axial views of high-resolution CT of temporal bone showing high dehiscent jugular bulb (arrow). (C) Simple mastoidectomy approach could only reveal easily touch bleeding of lateral side of jugular bulb (arrow) at mastoid portion. (D) Transtympanic approach by TEES: after trimming of inferior bony wall of left external acoustic canal, jugular bulb (big arrow) attached to basal turn of cochlea (small arrow) at hypotympanum, and round window (arrow head) could be seen clearly. (E) Pledget (arrow) was used for division. (F) Bone wax (arrow) was inserted for separation of jugular bulb and cochlea.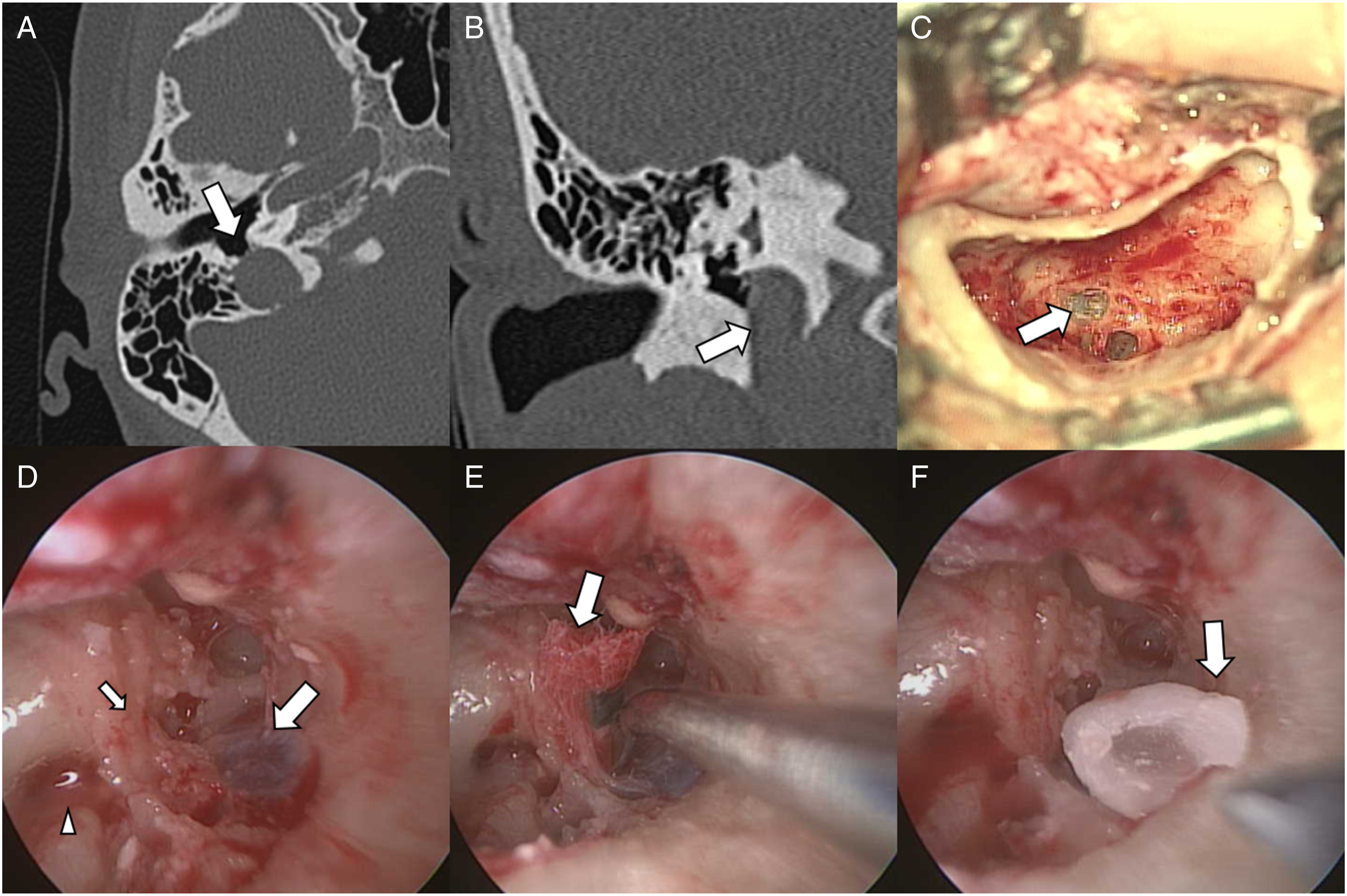
Initially, a simple mastoidectomy was performed, but easy, touch-induced bleeding of the lateral side of jugular bulb at the mastoid portion was noted (Figure 1C). Next, we tried a transtympanic approach using TEES for the purpose of exposing the jugular bulb at the hypotympanum after trimming of the inferior bony wall of the left external acoustic canal. The jugular bulb was noted at the hypotympanum, close to the basal turn of the cochlea and round window. After removing the thin bony wall covering the HDJB with a diamond burr, we divided the HDJB from the cochlea easily with gelfoam and pledget. Bone wax and temporalis fascia were inserted for the purpose of separation (Figures 1D-1F).
The follow-up tinnitus handicap inventory showed dramatic improvement (from 82 to 0). The tinnitus visual analog scale showed the same result (ranging from 8 to 2).
Discussion
We proposed a novel technique to resurface the HDJB via a transtympanic approach via TEES.
There were two different pathways (transmastoid and transtympanic) used to manipulate the HDJB.2-4 The use of the transmastoid approach made it possible to touch the lateral surface of the jugular bulb, but it was not possible to deal with the anterior and medial surface contact with the cochlea in the hypotympanum. The axis toward the lateral surface of the HDJB could increase the risk of bleeding injury to the jugular bulb due to difficulty with dissecting more than half of its circumference, and there was potential risk of injury to the inferior petrous sinus. 5
We tried a simple mastoidectomy first and found that the surgical axis was not suitable. Then, we tried a transtympanic approach via TEES. Trimming the inferior canal wall gave us better surgical field exposure by allowing the insertion of the endoscope and diamond burr to occur at the same time. The endoscope provided better and more direct vision of the contact plane of the HDJB with the cochlea, which was our main concern in the treatment of pulsatile tinnitus (Figure 2A). HDJB resurfacing by TEES. (A) The middle ear cavity and the high dehiscent jugular bulb are widely exposed via TEES approach by elevating the tympanomeatal flap after widening the tympanic annulus by drilling the posteroinferior meatal wall. (B) The dehiscent portion of the JB is separate from the cochlea and covered by bone wax extra-luminally.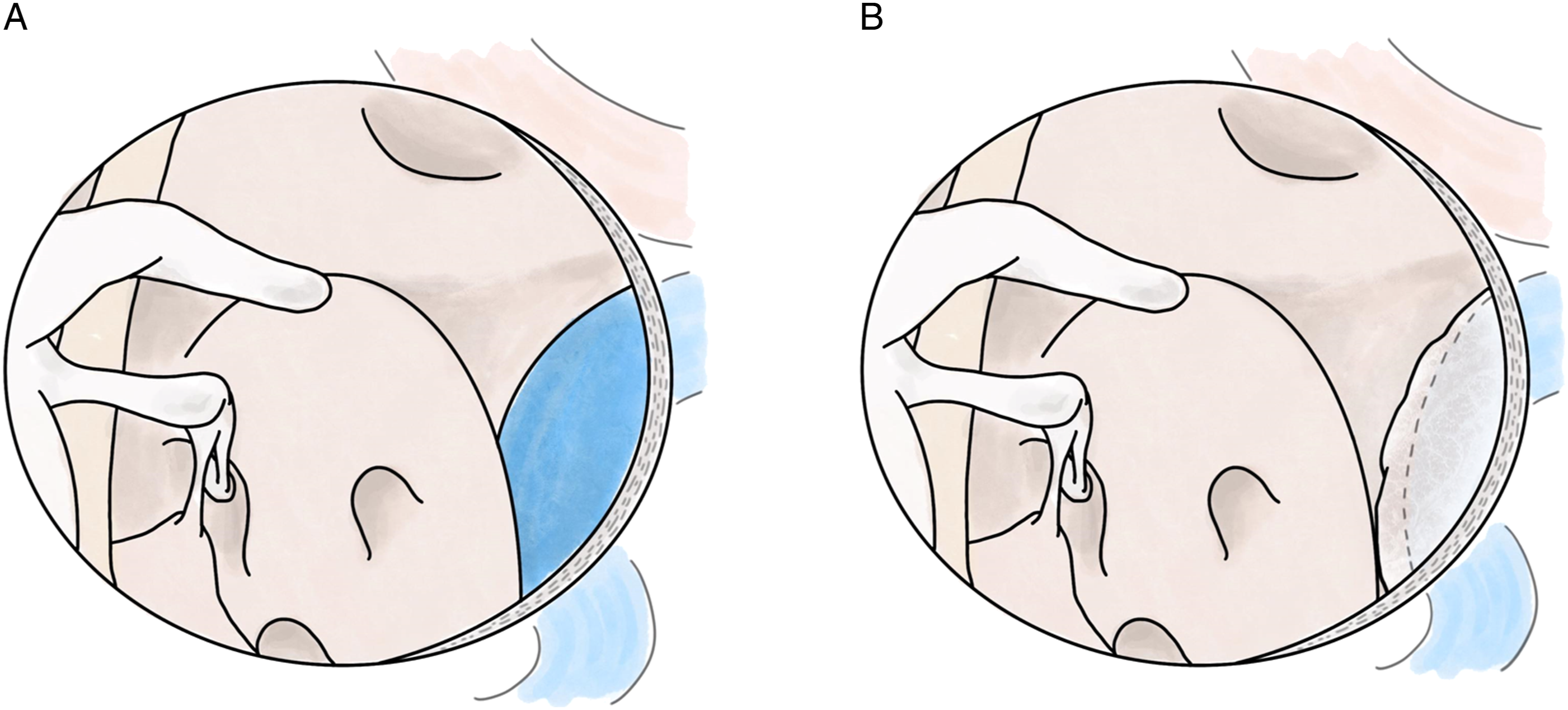
Compare to the traditional resurfacing technique, which only blocks air conduction of sound,2,6 insertion of bone wax or other material between the cochlea and the HDJB plus covering the jugular wall made it possible to block both the air and bone conduction (Figure 2B). We believe that this technique could lead to better outcomes.
To our knowledge, this is the first report discussing the resurfacing of a HDJB via a transtympanic TEES approach. Also, it is a minimally invasive, effective surgical treatment option in patients with HDJB.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.