
Abstract
Button battery ingestion in pediatric populations is a common occurrence with severe sequelae. Multiple case reports have established the occurrence of death, fistula formation, mucosal erosion, esophageal perforation, and bleeding post-ingestion of button batteries. However, there is a gap in the literature on the occurrence of bilateral vocal cord paralysis post-lithium battery ingestion. We present a case in which a 12-month-old male developed bilateral vocal cord paralysis following ingestion of a button battery. We compare our case to eleven other reports that exist in the literature based on age, sex, time until removal, clinical presentation, day upon which vocal cord paralysis developed, anatomic location, and post-operative course. We conclude that bilateral vocal cord paralysis is a time-sensitive complication which requires prompt diagnosis. Any child with stridor following button battery ingestion should undergo consultation with pediatric otolaryngology immediately. In addition, long-term follow-up is necessary to evaluate return of normal vocal cord function.
Keywords
Introduction
Between 1990 and 2009, over 65000 pediatric patients presented to emergency departments in the United States due to battery-related exposures, with battery ingestion comprising over 50 000 of these visits. 1 Additionally, button battery ingestion (BBI) data from 1985 to 2009 indicate a 6.7-fold increase in the number of ingestions associated with major complications or death. 2 Generally speaking, foreign body ingestion can be complicated by the substance, size, shape, composition, and location of the object. Button battery injuries can be specifically dangerous given their composition of caustic materials, which create hydroxide radicals within tissue and can result in coagulative necrosis. 3 Outcomes from ingestion can range from caustic injury to death. Data from the National Poison Data System and National Battery Ingestion Hotline illustrate a worsening trajectory of outcomes post-BBI. Therefore, BBI remains an important and epidemiologically relevant topic in pediatric otolaryngology. 4
Although death is the most feared complication from BBI, there are other life-altering complications that mandate immediate attention. These complications include massive bleeding from esophageal-aortal fistula, stenosis, perforation with mediastinitis, and reintubation following dyspnea and stridor. 5 Given enough time, the toxic and erosive nature of lithium batteries can lead to esophageal perforation.
There is a gap in the literature regarding long-term follow-up and vocal cord recovery following BBI. Pediatric cardiac surgery is another cause of vocal cord paralysis and can serve as a model for understanding recovery in patients post-BBI. A retrospective case study analyzing pediatric vocal cord paralysis after cardiac surgery revealed a median time until diagnosis of vocal cord paralysis of 20 days. A median time of 6.6 months was required for vocal cord refunction, and this only occurred in 35% of patients. 65% of patients had persistent vocal cord paralysis at a median follow-up time of 16.4 months. 6 An additional study indicated that complete recovery can occur in up to 61% of patients within 10 months, but feeding complications can still persist requiring gastrostomy tube placement in up to 45% of patients. 7 Hence, there has been no clear consensus in the literature regarding long-term outcomes. Treatment modalities for bilateral vocal cord paralysis include cordotomy, arytenoidectomy, tracheostomy, and re-innervation. 8 Destructive procedures should be avoided in children with a chance of return of vocal cord function.
In this case report, we offer the additional complication of vocal cord paralysis, which has been infrequently mentioned in the literature as a complication following BBI. While this complication is exceedingly rare, the potential sequelae are severe. Hence, complications from lithium battery ingestion, including vocal cord paralysis, should be evaluated in any child presenting with stridor following battery ingestion.
Case report
The patient presented to the hospital at 12 months of age with hematemesis and respiratory distress after an unwitnessed foreign body ingestion. A STAT chest radiograph revealed a button battery lodged in the esophagus at the level of the thoracic inlet [insert Figure 1]. The timing of the BBI was not known. The ingestion resulted in a mass effect with inflammation, which deviated the airway anteriorly. Oxygen therapy was initiated and the patient was rushed to the operating room where flexible and rigid esophagoscopy was performed with successful removal of the foreign body. Findings included erythema of 75% of the esophageal lumen circumference and edema of the posterior tracheal wall. The patient subsequently received 550 mg IV ceftriaxone and 0.4 mg of dexamethasone every 6 hours at 2 mL/hour in the pediatric intensive care unit. The pediatric gastroenterology team inserted an 8FR nasogastric tube via wire-guided fluoroscopy. After 48 hours, esophagastroduodenoscopy revealed gray brown discoloration in the upper esophagus at the 13–14 cm mark; the mid and distal esophageal mucosa appeared normal. Bronchoscopy revealed an anatomically intact trachea, carina, and mainstem bronchus. The patient was stable at discharge despite minor stridor. Chest radiographs of the patient upon arrival to the emergency room, revealing a button battery lodged in the esophagus at the level of the thoracic inlet.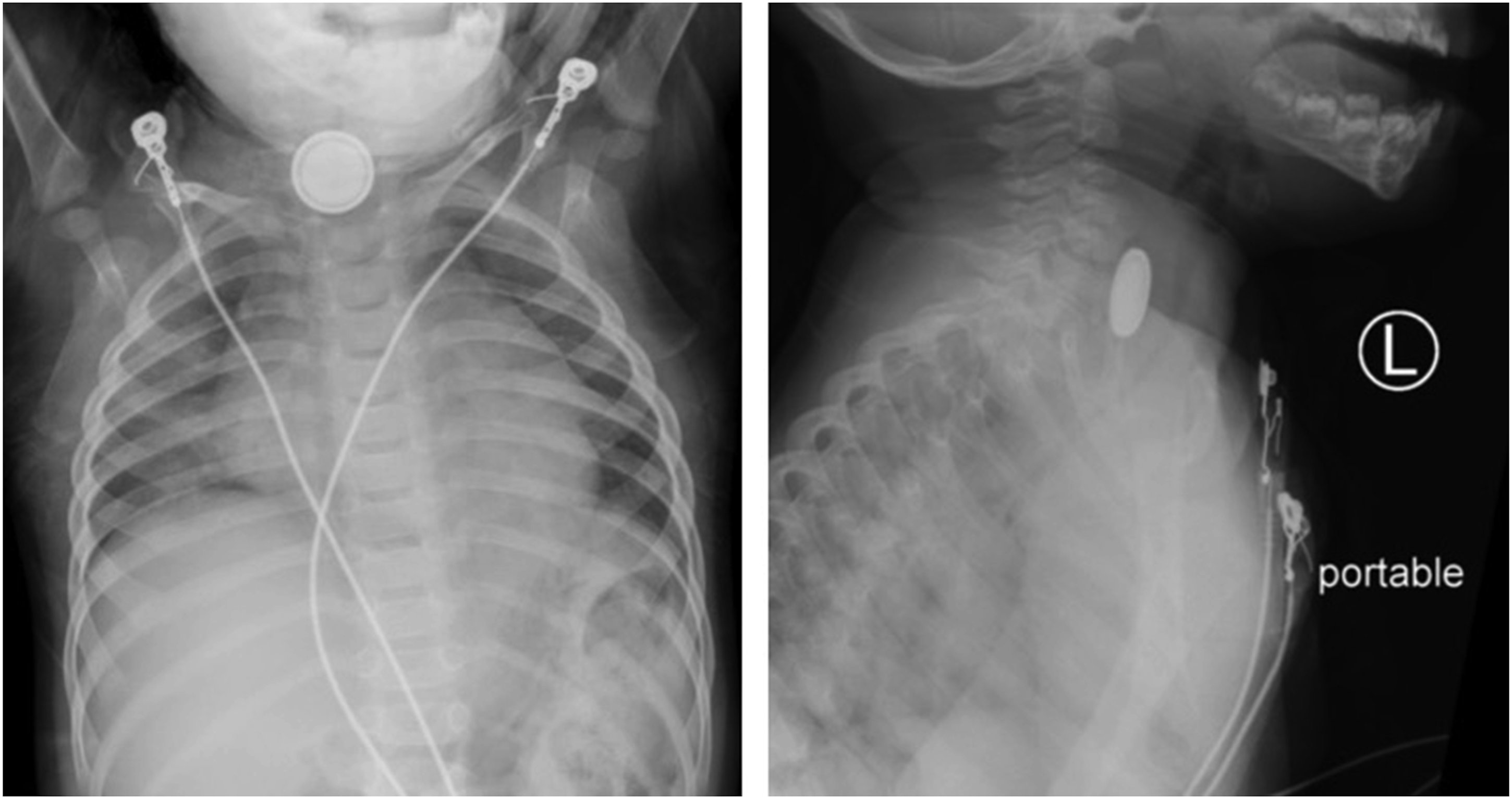
At 1-month follow-up, the patient was referred for evaluation of persistent stridor. Flexible fiberoptic laryngoscopy performed in office revealed significant bilateral vocal cord paresis versus paralysis and paradoxical vocal cord adduction on inspiration was noted. To rule out other airway lesions, the patient was brought to the operating room for formal airway evaluation, which revealed a small scar band on the posterior aspect of the esophageal introitus.
At 2-month follow-up, there was no clinical improvement. Persistent stridor and respiratory distress with increased activity were noted. A tracheostomy tube was placed to relieve the respiratory distress.
At 9-month follow-up, the patient was noted to have regained partial function of both vocal cords on flexible fiberoptic laryngoscopy but was unable to tolerate attempts at decannulation.
Continued follow-up revealed no improvement of vocal cord function. The patient underwent laryngotracheal reconstruction with posterior costochondral graft at 23 months. The patient tolerated the procedure well and underwent decannulation at 3-month post-op. The patient has adequate respiratory function with vocal cord paralysis on continued long-term follow-up.
Methods
A literature search of PubMed, EMBASE, and Scopus from 1990 to 2021 for the terms “button battery ingestion,” “button battery ingestion and vocal cord paralysis,” and “button battery ingestion and vocal fold paralysis” was performed. Informed consent for patient information in this case was provided.
Results
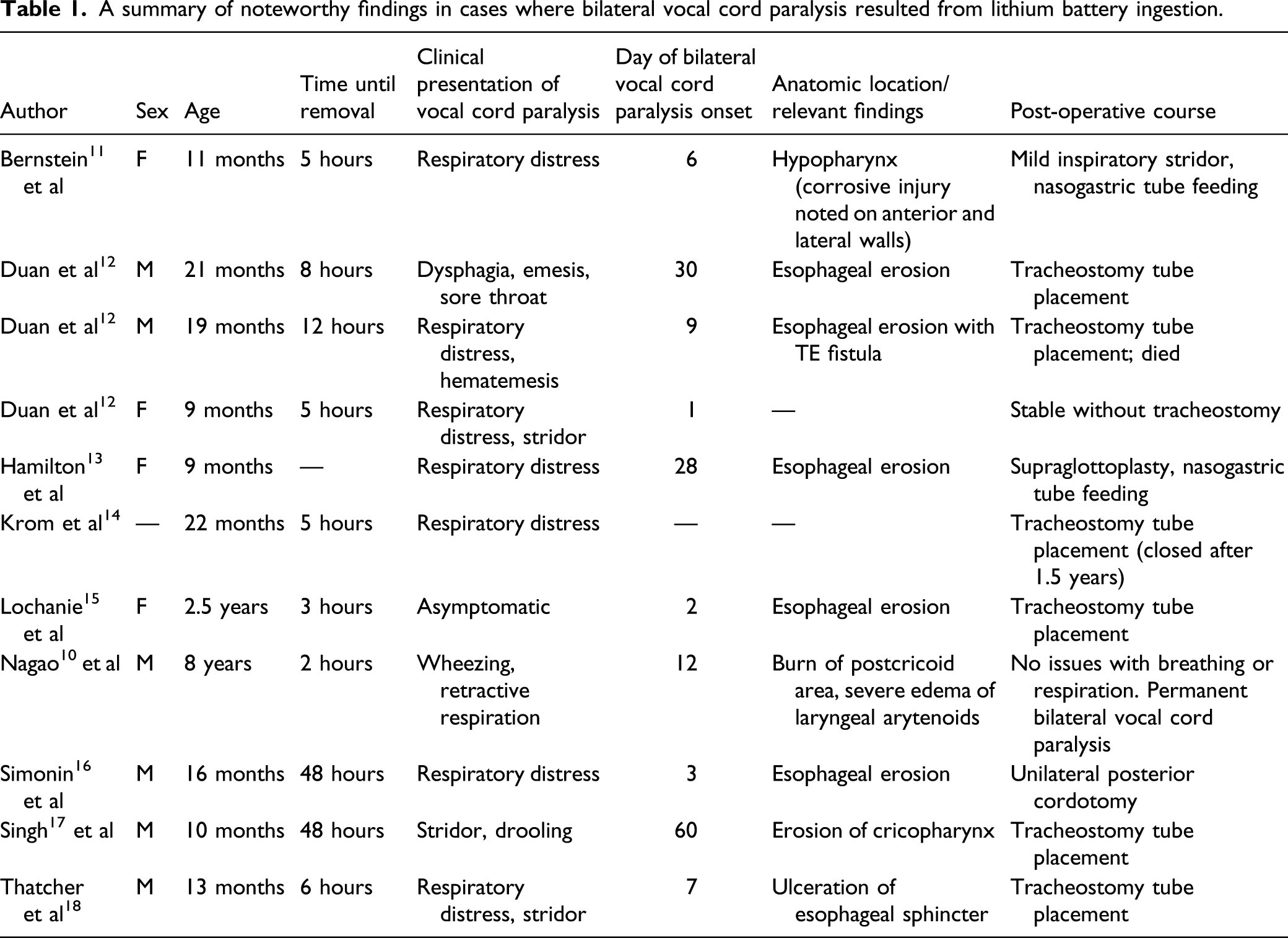
A summary of noteworthy findings in cases where bilateral vocal cord paralysis resulted from lithium battery ingestion.
Discussion
Adverse events from BBI are increasing in the literature because they power small, easily accessible devices such as electronic games and watches. 2 The metallic and shiny appearance can attract children who often mistake the battery as an edible item. 19 Appropriate management of battery ingestion is integral in optimal patient outcomes. The mainstay treatment for isolated batteries located in the gastroesophageal junction rarely requires intervention and can be managed by close monitoring. 20 However, button batteries located in the esophagus require timely endoscopic removal. A study evaluating 1891 foreign body ingestions resulted in prompt endoscopic removal for all objects when the anatomic location was the esophagus. 21 Endoscopic removal in the esophagus is more urgent since electrolysis reactions can occur in this type of environment. In a study of porcine esophagi, a battery was placed in order to determine the molecular impact on the tissue. Coagulation necrosis occurred at the positive pole of the battery and deep liquefactive necrosis occurred at the negative pole. Tissue damage was noted within the lamina muscularis within 12 hours, and damage continued while residual voltage was still contained within the battery. Hence, geographic and anatomic considerations should reinforce the urgency and necessity of prompt diagnosis. 22
In general, the clinical diagnosis of battery ingestion can be difficult in a pediatric population given the overlapping presentation with acute viral illness. Fever, cough, decreased appetite, and decreased fluid intake with vomiting can create a classic clinical presentation for both pathologic states. However, button battery injury is time sensitive, and the diagnosis should ideally be made within 2 hours in order to prevent mucosal damage. While coins and button batteries can appear similar on X-ray imaging, a double ring or halo sign can help differentiate the two objects. 22
Vocal cord paralysis is a life-altering condition that can be a severe complication of lithium battery ingestion. The severity, time frame, and outcome of vocal cord paralysis following BBI have not been well understood. Only a few cases have been reported in the literature, as summarized in Table 1.
The presentation of this complication has been reported primarily under the age of 1 years old. However, a case has been reported in later childhood. 10 Of note, a majority of these case reports presented with respiratory distress including stridor, retractive respirations, drooling, and wheezing. Hence, any form of respiratory distress in a patient with potential foreign body ingestion should result in an urgent chest radiograph to rule out this complication. The onset of vocal cord paralysis does not necessarily have to occur earlier in disease course. Late presentation up to 2 months post-endoscopic removal has been reported previously in the literature; this delayed presentation is similar to our own reported case. 2 The most common finding on endoscopy in the reported cases was erosion of the esophageal mucosa. Our recommendation is to visualize movement of the vocal cords via laryngoscopy immediately post-endoscopic removal of a lithium-based battery. Diagnosis in each case was made multiple days after endoscopic removal. Earlier visualization and recognition could lead to earlier intervention. Additionally, since respiratory distress was a delayed complication in each case, earlier visualization of the vocal cords could help predict a source of possible respiratory demise in the pediatric population.
Conclusion
The purpose of this case illustration was to highlight a relatively rare consequence of lithium battery ingestion in pediatric populations and compare it to eleven previously established cases in the literature. This case was unique in that partial recovery of the vocal cords was noted at the 9-month follow-up visit. Bilateral vocal cord paralysis should be kept on the differential post-endoscopic removal of the foreign body, and a delayed presentation should be expected. Atypical or lasting respiratory distress should raise suspicion of bilateral vocal cord paralysis. These cases often require airway intervention such as a tracheostomy and airway reconstruction.
Footnotes
Author Note
Meeting: Presented at 15th Annual Academic Surgical Congress, Orlando, FL, February 2020.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
Our institution does not require ethical approval for reporting individual cases or case series.
Informed consent
Written informed consent was obtained from a legally authorized representative for anonymized patient information to be published in this article.
Statement of human and animal rights
This article does not contain any studies with human or animal subjects.