
Abstract
Horizontal canal fistulas are not uncommon in patients with cholesteatoma. Patients with canal wall down cavities and exposed horizontal canal fistulas develop significant dizziness with wind or suction exposure. Obliteration of mastoid cavities in patients with exposed fistulas can be challenging. We describe a patient with horizontal canal fistula and chronic dizziness from wind exposure who underwent successful mastoid cavity obliteration with preservation of hearing. Patients with horizontal canal fistulas in a canal wall down cavity can be managed with mastoid obliteration for relief of dizziness.
Introduction
Cholesteatoma-induced fistulas most commonly involve the horizontal semicircular canal (HSC). 1 After the HSC, the superior canal, posterior canal, and rarely the cochlea can be affected. 1 The incidence of cholesteatoma in adults is reported to be 9.2 per 100 000 per year, while 2.7% to 12% of these cases eventually lead to the occurrence of a labyrinthine fistula. 2 Further, 90% of the fistulas occur in the lateral semicircular canal. A significant number of HSC fistulas lead to sensorineural hearing loss (SNHL). Many surgeons will leave the cholesteatoma matrix on the HSC fistulas when faced with this problem intraoperatively. This, however, leaves the patient with chronic problems with dizziness after suctioning or wind exposure. Herein, we discuss a case of a previous HSC fistula in a patient with canal wall down mastoidectomy with emphasis on the management and avoidance of SNHL during repair.
Case
A 54-year-old male presented to us status post left-sided canal wall down mastoidectomy surgery and dizziness from air or wind exposure. The patient was unable to walk outdoors without covering the ear or using cotton in the ear. The patient had a history of migraine and would develop significant vertigo for a few days after getting suctioning in the ear canal. He was also unable to take part in water activities since his meatoplasty was very large and would not hold any type of earplug. His examination showed a horizontal canal fistula exposed in the cavity (Figure 1). Computed tomography imaging confirmed HSC fistula (Figure 2).
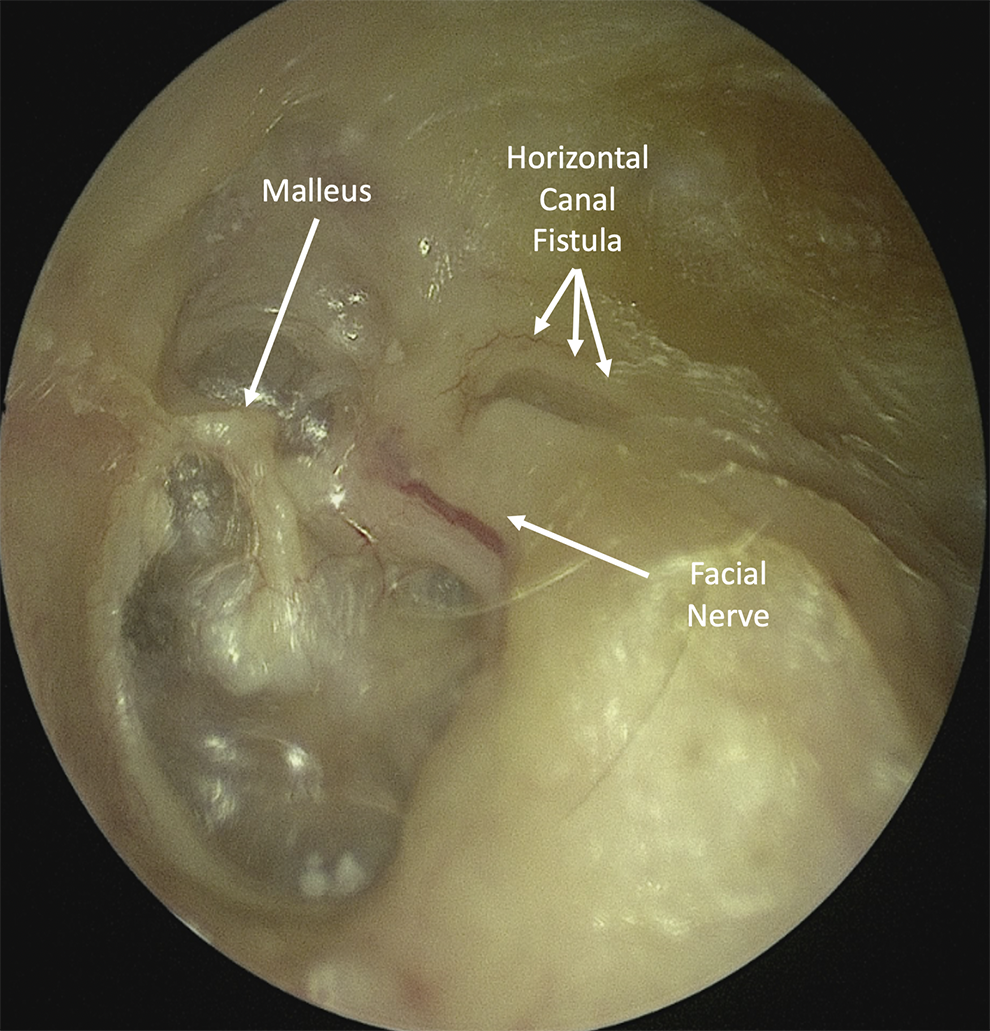
Left ear examination on presentation showing the horizontal canal fistula (short arrows) and exposed facial nerve (long arrows) in the canal wall down cavity.
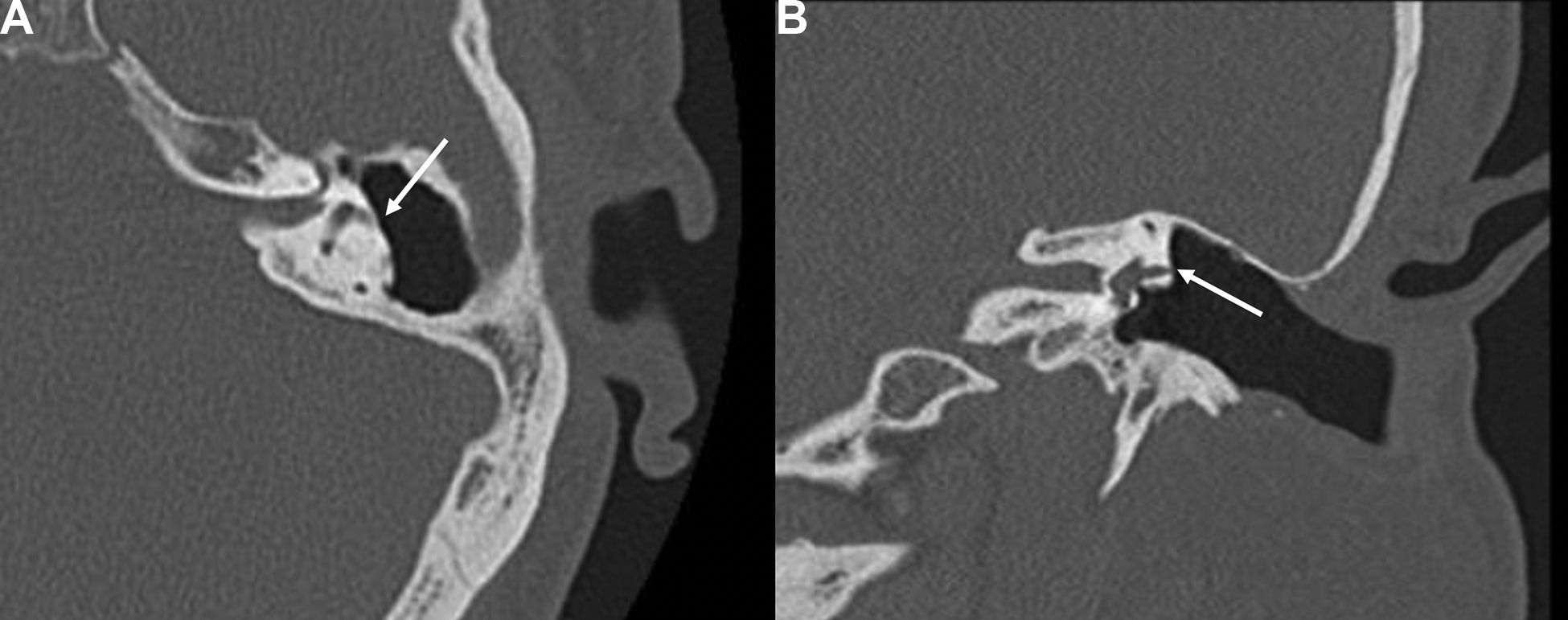
Computed tomography (CT) of the patient showing horizontal canal fistula on axial (A) and coronal (B) images.
After discussion with the patient, he underwent a mastoid obliteration procedure. Intraoperatively, using a postauricular approach, all skin was separated from the cavity. After all the skin from the cavity had been raised above and below the horizontal canal, the fistula is addressed as the last step of the operation. The epithelium over the HSC fistula is raised using a blunt instrument. The tip of the instrument is turned to be gently pressing on the epithelium or at the junction between the epithelium and the fistula. There was no instrumentation of the HSC fistula is performed. In this case, the Paparella drum elevator was used and flipped over so that the tip of the instrument was not in contact with the fistula. The nondominant hand used a 24 suction with “finger off the hole” technique to hold the epithelium as the instrument was used to dissect the epithelium of the fistula (Figure 3). A small piece of fascia soaked in dexamethasone 10 mg/mL was immediately placed over the intact fistula with no membranous disruption. The fascia is then covered with previously obtained bone putty and a 0.005-inch thick silastic was placed on that area. This step is performed to prevent inadvertent entry into the HSC in the future given the distortion of the anatomy after this surgery. The bone pate is then covered with cartilage and fascia and finally covered with the mastoid epithelium which was preserved (Figure 4). Postoperative hearing at 3 months postoperatively was the same as preoperatively, showing preservation of the bone conduction thresholds at 500 to 4000 Hz and air conduction at 8000 Hz. The patient’s wind-induced dizziness resolved.
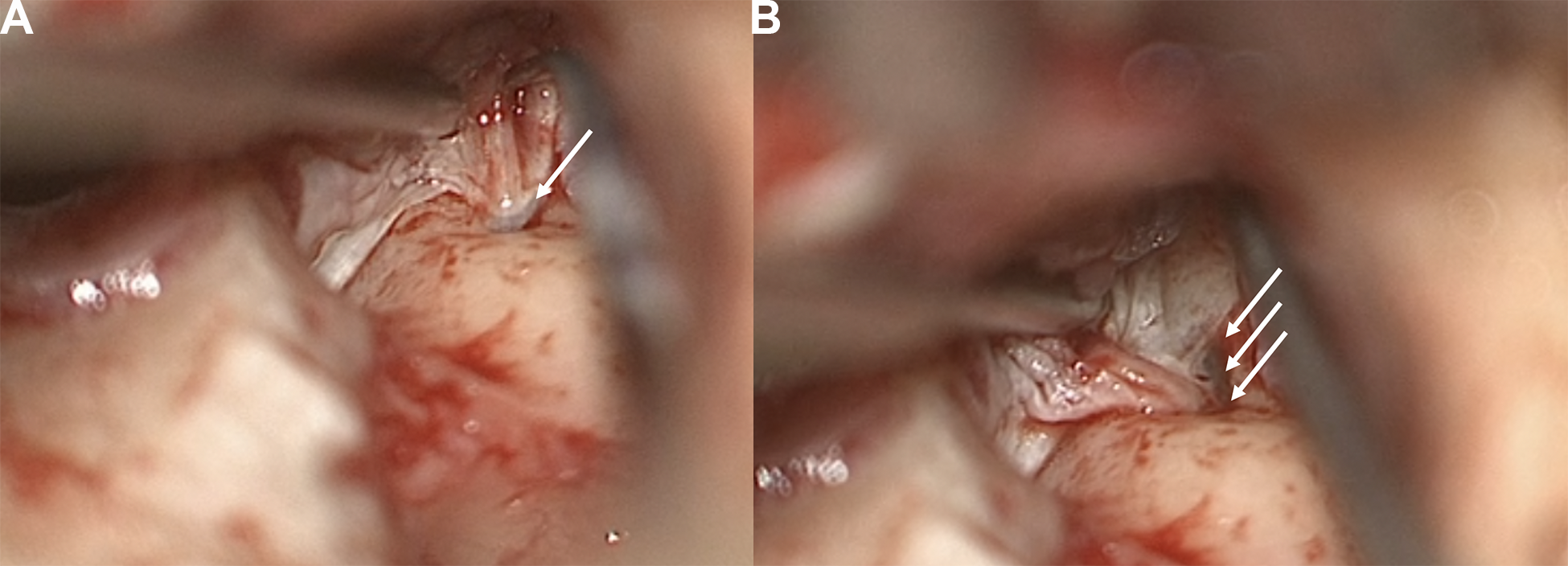
Intraoperative images showing the last separation of the epithelium from the fistula (A) (arrow) and the exposed fistula (arrows) (B).
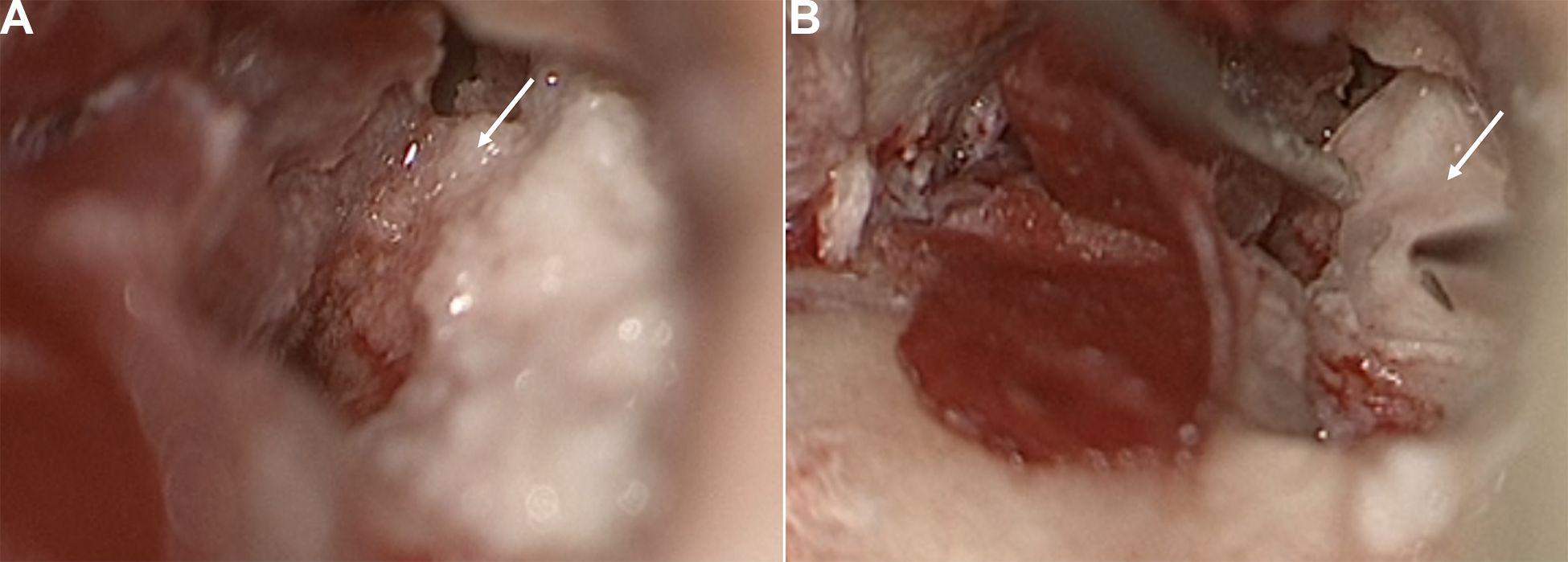
(A) Bone pate covering the fistula (arrow); and (B) silastic over the bone pate (arrow).
Discussion
Horizontal semicircular canal fistula is the most common labyrinthine fistula in cholesteatoma and has been described to be present in up to 5% of cholesteatoma cases. It is associated with deafness postoperatively in about 20% of cases. 1,3 There are 2 options intraoperatively to manage the fistula. The first is to remove the matrix and repair over the horizontal canal. This carries the risk of hearing loss but lowers the chance of dizziness after surgery. The second option is to leave the matrix adherent to the HSC fistula and perform a canal wall down procedure. This option leaves the patient with a lifetime of problems with dizziness with wind or suctioning, though has a lower risk of SNHL. The intraoperative choice is best to be made based on the patient’s priorities, which should be discussed preoperatively.
We have been successful in removing the cholesteatoma from the HSC fistula in over 25 cases without SNHL. In patients who have presented to us with a previous fistula, such as the case above, we have successfully separated the epithelium of the cavity and obliterated the area over the HSC with bone pate without SNHL.
The surgical technique that can assure success depends on meticulous dissection. It is important to work very slowly with a 24 suction with the finger off of the hole on the edge of the epithelium holding tension but with no contact of the suction with the HSC fistula. The instruments used for dissection should be a broad flat instrument with the tip at the junction of the epithelium and fistula or on the epithelium away from the fistula. If the epithelium is strongly adherent to the fistula, the tip of the sickle knife can be used gently to take down the adhesions of the cholesteatoma with the tip toward the epithelium at the junction of the epithelium and the fistula. The surgeon should dissect from above and below to isolate the HSC. A piece of fascia soaked in dexamethasone should be ready and nearby in the mastoid to place quickly onto the fistula. Sometimes, it is difficult to locate the fistula in a cholesteatoma case and the surgeon can suction the keratin debris and look through the matrix for the location of the HSC fistula, which will look dark. After covering with fascia, the HSC should be covered with bone pate, and subsequently with thin silastic for future identification. We additionally use cartilage and another layer of fascia to insulate the HSC from the canal as part of the mastoid obliteration. The patient should be placed on postoperative antibiotics. We commonly use doxycycline 100 mg twice a day for 7 days. We also soak the bone pate and cartilage in topical ofloxacin prior to placement.
Patients with horizontal canal fistulas in a mastoid cavity can be successfully managed with mastoid obliteration. Obliteration of the mastoid requires meticulous dissection to separate the epithelium from the fistula and immediately cover the fistula. Additionally, the usage of bone pate over the fistula and obliteration of the mastoid will eliminate the dizziness from wind or suction exposure.
Footnotes
Authors’ Note
This manuscript is original and has not been submitted elsewhere in part or in whole.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.