
Abstract
Hypertrophic pachymeningitis (HP) is defined by inflammation and thickening of the dura mater, and the etiologic factors are idiopathic or secondary to various conditions. To date, HP in the internal auditory canal (IAC) has rarely been reported. There have only been 3 reports of HP in the IAC. Magnetic resonance imaging showed enhancement of along the IAC and vestibule. After antibiotic treatment, enhancement was reduced with visible seventh and eighth nerves. The patient underwent tympanomastoidectomy. To our knowledge, this is the first case of HP associated with a labyrinth fistula complicated by cholesteatoma. We report MRI image with literatures.
Case Report
A 66-year-old man was referred to our department after presenting to a local clinic with recent onset of intractable otorrhea and dizziness. The patient reported no history of surgery. He had been suffering from chronic otitis media on the left side for several years and was intermittently treated with antibiotics at local clinic. He experienced mild dizziness and otorrhea in the left ear. He did not show spontaneous nystagmus or signs of meningitis. Otoendoscopy revealed subtotal perforation with attic cholesteatoma in the left ear. The coronal view of temporal bone computed tomography revealed that the mastoid cavity was filled with soft tissue and was accompanied by a lateral semicircular canal fistula and new bone formations of the superior semicircular canal on the left side (Figure 1). Axial T1-weighted post-contrast magnetic resonance imaging (MRI) showed enhancement of the entire length of the internal auditory canal (IAC) dura (arrow) with the horizontal semicircular canal and cholesteatoma sac on the left side (Figure 2). No masses or lesions involving the eighth cranial nerve were visible. The patient showed no signs of nystagmus in the fistula test. Pure-tone audiometry measurements showed scale out on the left side. The patient was treated with a 3-week course of oral cefixime at a dose of 400 mg/d. With the antibiotic treatment, follow-up MRI revealed significantly reduced enhancement of the IAC and the seventh and eighth nerve bundles on the left side (Figure 3). However, there was no interval change in scale out of hearing on the left side.
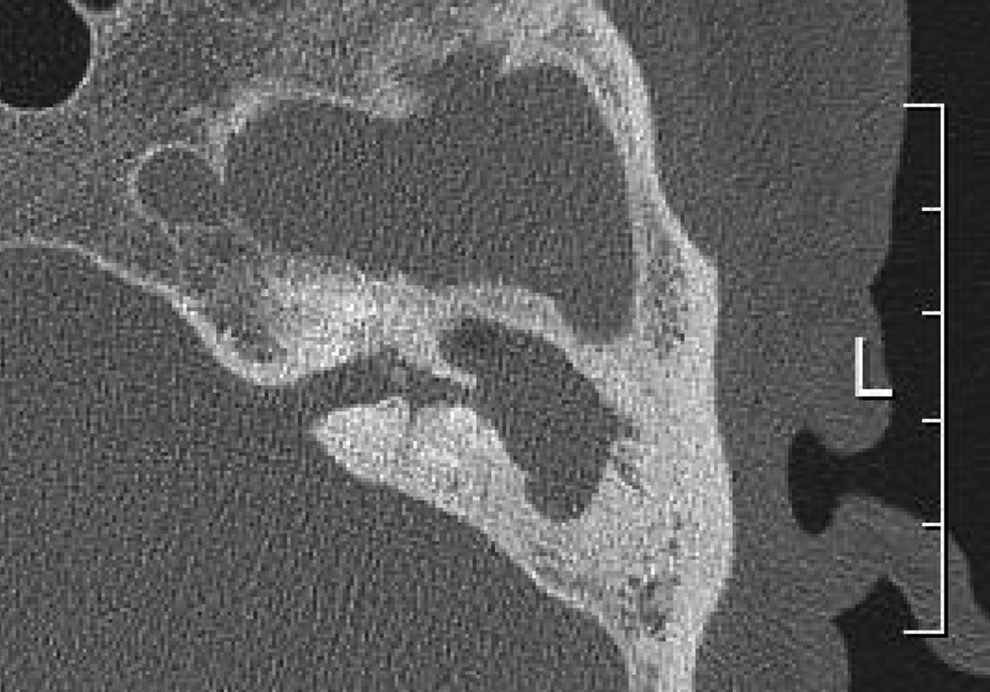
The axial view of temporal bone computed tomography revealed that the mastoid cavity was filled with soft tissue and was accompanied by a lateral semicircular canal fistula and new bone formations of the superior semicircular canal on the left side.
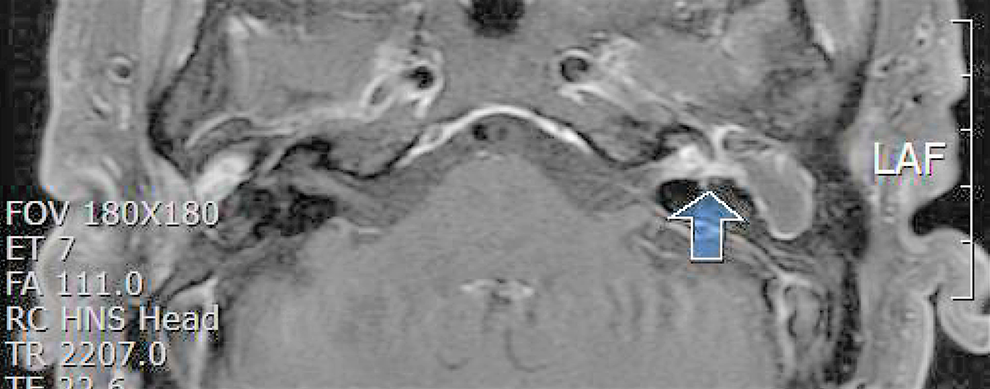
Axial T1-weighted post-contrast magnetic resonance imaging (MRI) showed enhancement of the entire length of the internal auditory canal (IAC) dura (arrow) with the horizontal semicircular canal and cholesteatoma sac on the left side.
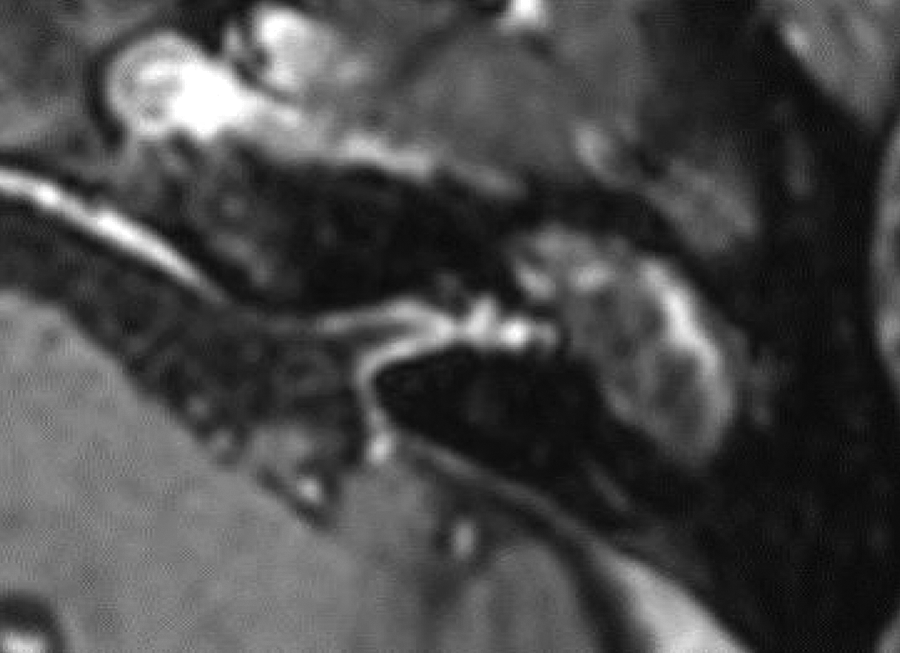
With the antibiotic treatment, follow-up magnetic resonance imaging (MRI) revealed significantly reduced enhancement of the internal auditory canal (IAC) and the 7th and 8th nerve bundles on the left side.
The patient underwent canal wall down mastoidectomy with tympanization and mastoid obliteration. Dehiscence of the tympanic and second genu portion of the facial canal was found. Majority of the cholesteatoma matrix was removed from the middle ear and mastoid cavity, except for the fistula area. After irrigation with a small suction tip, the remaining matrix around the fistula was completely dissected using the non-suction technique with intraoperative dexamethasone injection as previously reported. 1 The fistula area was repaired by a bone plate with fibrin glue. The neodrum was made by a thin slice of cartilage and perichondrium, and mastoid obliteration was performed by demineralized bone matrix with an anteriorly based periosteal flap. The canal skin was repositioned over the perichondrium. The external auditory canal (EAC) was packed using gelfoam and Merocel. Three weeks after the operation, the EAC Merocel packing was changed with ciprofloxacin soaked Merocel, and remained gelfoam on the neodrum was preserved. The EAC Merocel packing was changed every 3 weeks in the outpatient clinic. The patient was instructed to administer ciprofloxacin ototopical drops in the head-held position for 3 minutes to allow soaking of the Merocel in the ear canal. At the 3-month postoperative follow-up, otoendoscopy showed normal EACs and tympanic membrane.
Discussion
Hypertrophic pachymeningitis (HP) is defined by inflammation and thickening of the dura mater, and the etiologic factors are idiopathic or secondary to various conditions. 2 To date, HP in the IAC has rarely been reported. There have only been 3 reports of HP in the IAC. One case was accompanied by sudden hearing loss, while the other 2 cases were accompanied by immunoglobulin IgG4 disorder.3-5 To our knowledge, this is the first case of HP associated with a labyrinth fistula complicated by cholesteatoma.
In the present case, HP of the IAC and vestibule was secondary to the labyrinthine fistula complicated by cholesteatoma. Cases of a labyrinthine fistula carry a higher risk of profound hearing loss by cholesteatoma invasion or its dissection during the surgery. 6 Large fistulas are associated with an increased likelihood of severe sensorineural hearing loss and deafness. 7 In the present case, the preoperative hearing examination revealed deafness.
Computed tomography and MRI are of the highest importance for detecting pathologies of HP or labyrinthine fistula. In the present case, MRI revealed enhancement of the vestibule and lateral semicircular canal extending to the entire length of the IAC. Antibiotics and steroids have been used to treat HP before surgery. In the present case, MRI showed significantly reduced enhancement of the IAC and the seventh and eighth nerve bundles after the antibiotic treatment. Iaccarino et al 8 reported reduction of the IAC enhancement by medication to be indicative of a cold phase in which inflammation in the IAC has ceased and surgical treatment is required. Surgical removal of the cholesteatoma, which is the main source of infection, followed by labyrinthine fistula repair and postoperative temporal bone MRI for monitoring the progressive regression of the HP of IAC is considered to be the best treatment option.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.