
Abstract
The cricoid plays 2 key roles: phonation and maintenance of the airway frame, both of which are lost in cases of comminuted cricoid fractures. The management of these 2 functions becomes a challenge in planning surgical treatment. We report the treatment course in a case of traumatic comminuted cricoid fracture that was resolved with good airway and phonatory functions. A 25-year-old man fell down the stairs and complained of respiratory discomfort and hoarseness of voice. A computed tomography scan showed comminuted cricoid fracture; therefore, surgery was performed to restore the patient’s airway and phonation functions. We found that the airway was maintained by the anterior part and that the phonation depended on the posterior part of the cricoid. This novel concept helped clarify the treatment goal in this case of comminuted cricoid fractures. Furthermore, it is important that the anterior part of the cricoid is reconstructed with sufficient internal diameter, while the posterior part of the cricoid is reconstructed in the correct position.
Introduction
The cricoid maintains the airway by its chondral frame. It also has key roles in the phonatory function of the larynx as a foundation of arytenoids. 1 These 2 important roles are immediately lost in cases of comminuted cricoid fractures. 2 Therefore, surgeons must consider these 2 functions in the management of such cases.
In the management of comminuted cricoid fractures, the restoration of the airway is critical. 3 Phonatory function is likely to become a secondary priority and may be missed in the initial management of comminuted cricoid fractures because it is not considered life threatening. However, phonatory function should not be discounted because it significantly affects the quality of social living. 4 Reduction in the cricoid fragments as a secondary treatment after healing becomes more difficult because of the growth of fibrous tissue at the fracture points. Therefore, reduction in the framework of the cricoid for phonatory function in the initial management should be considered as important as the reconstruction of the airway.
Surgical treatment was performed in a case of comminuted cricoid fracture to restore the airway and phonatory functions at the same time. We report the treatment course in a case of traumatic comminuted cricoid fracture that resolved with good airway and phonatory functions.
Case Report
A 25-year-old man, under the influence of alcohol, fell down the stairs. Immediately after the fall, he complained of respiratory discomfort and hoarseness of voice and visited the emergency department at a district general hospital. Laryngeal endoscopy and a computed tomography scan revealed a hematoma in the larynx and mediastinal emphysema. The hematoma in the larynx and mediastinal emphysema spontaneously improved with rest for a few days. However, the hoarseness did not improve, thereby prompting his presentation on 9 days after the injury.
At presentation, there were no abnormal findings upon inspection of the anterior neck. There was no noted stenotic sound or respiratory discomfort. Phonatory function test revealed a maximum phonation time (MPT) of 4.8 seconds and mean flow rate (MFR) of 463 mL/s. The patient scored 36 points on the Voice Handicap Index (VHI)-10. A laryngeal endoscopy demonstrated the maintenance of mobility in the bilateral arytenoids. However, there was a white prominence on the dorsal wall of the larynx that caused glottic closure insufficiency by obstructing the movement of the vocal folds (Figure 1A). Furthermore, there was a noticeable gap in the levels of the right and left vocal folds. A computed tomography scan revealed a complete vertical fracture of the cricoid cartilage on the posterior lamina and the right and left sides of the arch. There was no fracture in the thyroid cartilage. The transverse diameter of the subglottic space was shortened by the overlapping of the pieces of the posterior lamina of the cricoid. Moreover, the fracture on either side of the median of the cricoid arch shortened the anteroposterior diameter of the subglottic space (Figure 1B). We planned a reconstructive surgery to restore the airway and phonatory functions. The surgery was performed 15 days after the injury.
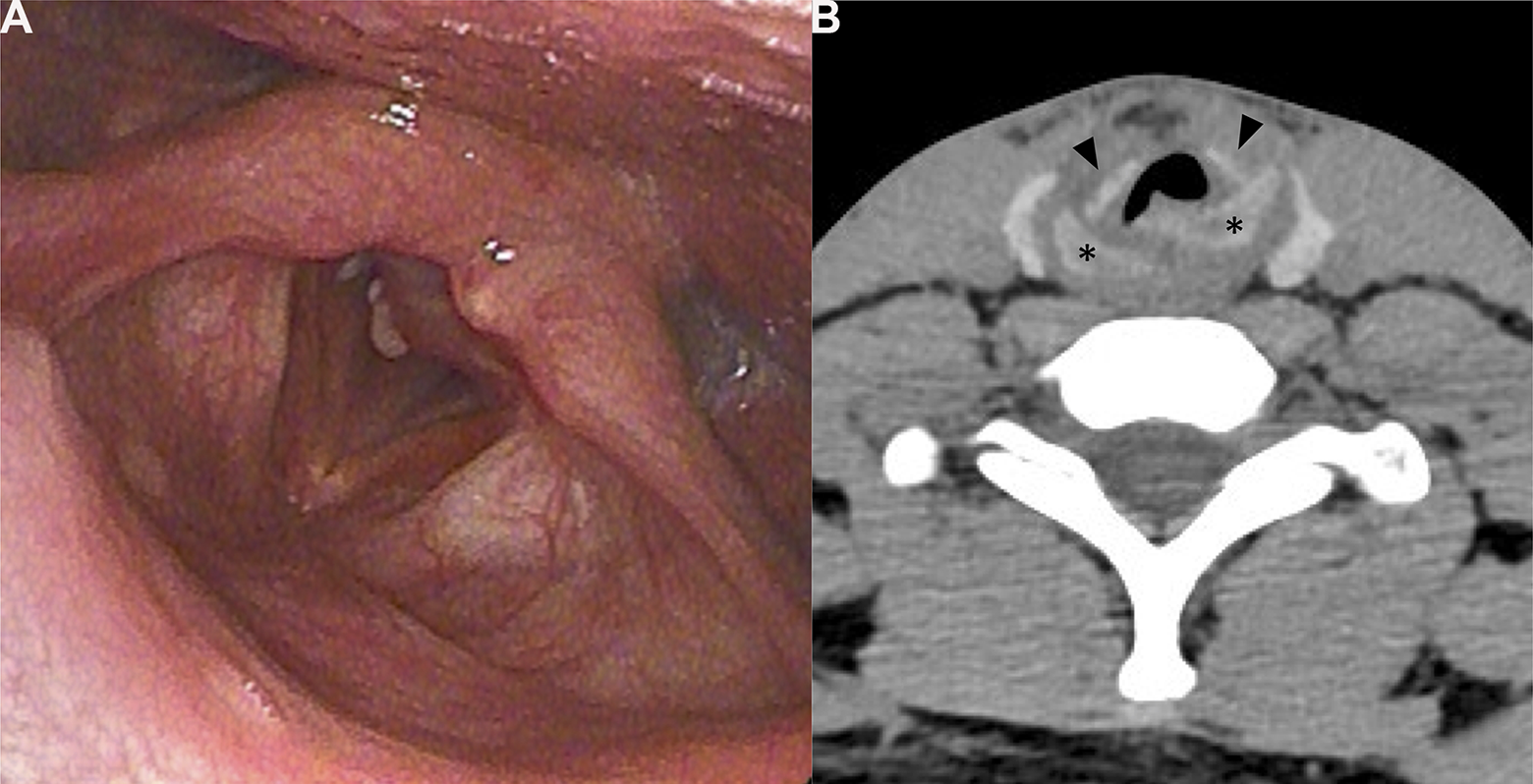
(A) A laryngoendoscopic image acquired at the initial visit. A white prominence is noted at the dorsal wall of the larynx. (B) A computed tomography image of the cricoid acquired at the initial visit. ▴, anterior arch; *, posterior lamina.
Intraoperative Findings
For airway management, we began with tracheostomy under local anesthesia. We created a tracheostomy site as far as possible from the cricoid for the final closure of tracheostomy at the end of the surgery. After a vertical median neck incision, the thyroid was split and a tracheostomy was performed between the third and fourth tracheal rings. The patient was then intubated, and general anesthesia was induced. The arch of the cricoid was fractured to pieces on the median and bilateral sides. We used an anterior laryngeal fissure approach with a vertical incision from the cricothyroid membrane to the first tracheal ring. The subglottic lumen was opened like a double door with fulcrum points that were of the fractured points of either lateral side of the cricoid. We inspected the posterior wall of the larynx (Figure 2A), the posterior lamina of the cricoid fractured at the median, and the edges of the fracture exposed through the mucosa. The edges of the fracture were irregular; hence, the edges did not coaptate as well as before.
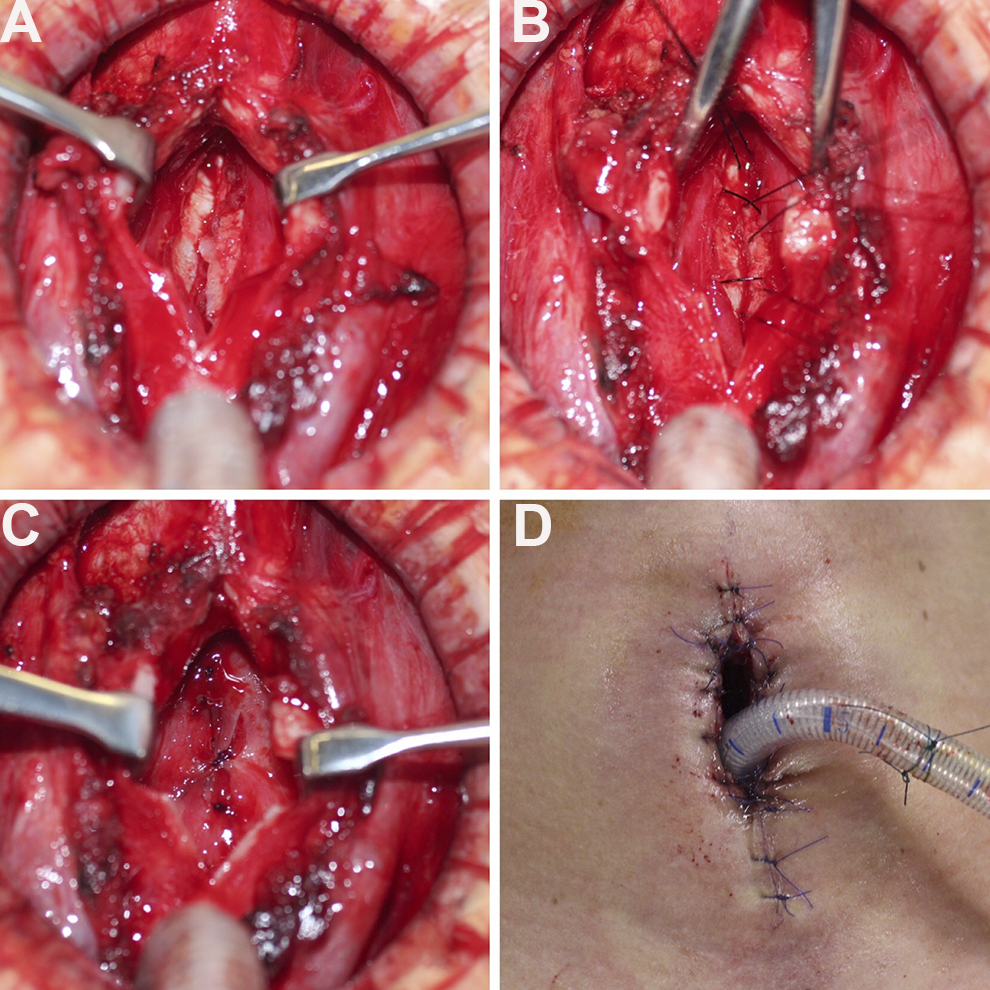
Intraoperative photographs of the surgical field. (A) The subglottic lumen was opened. (B) Two sutures were used to fix the posterior wall of the cricoid. (C) The torn mucosa was sutured. (D) We sutured the ends of the laryngeal fissure to the cutaneous cut ends and formed a laryngocutaneous fistula.
We shaved the irregular fracture ends with a messer and reduced them to align at the level of the right and left arytenoids. We used 2 sutures with small needles: 12-mm, 1/2 R, swaged needles with a taper point, and 3-0 Nylon Suture (Bear Medic Co.; Figure 2B) because the working space was small. We sutured the torn mucosa with the same thread and needle (Figure 2C). To ensure that the comminuted and loose pieces of the cricoid arch would be fixed tightly and would also serve as a luminal supporting material, we sutured the ends of the laryngeal fissure to the cutaneous cut ends and formed a laryngocutaneous fistula (Figure 2D). We then closed the caudal tracheostomy using sutures. Although not required, we placed a T-tube (KOKEN) through the laryngocutaneous fistula for airway safety in the immediate postoperative period.
Postoperative Course
On postoperative day 30, laryngeal endoscopy showed full bilateral arytenoid motion and improved glottic closure. Maximum phonation time was 9.2 seconds, MFR was 404 mL/s, and VHI-10 was 37 points. On postoperative day 60, we decannulated the T-tube. When the patient closed the laryngocutaneous fistula with his hand, MPT was 12.6 seconds, MFR was 204 mL/s, and VHI-10 was 32 points. On postoperative day 72, we closed the fistula with a local flap under local anesthesia after fixing the laryngocutaneous fistula. Afterward, there was no complaint of respiratory discomfort. A year after the second operation, laryngeal endoscopy showed a broad subglottic space without stenosis; MPT was 12.1 seconds, MFR was 194 mL/s, and VHI-10 was 29 points.
Discussion
The cricoid has 2 roles: phonation and maintenance of the airway structure. This makes it difficult to plan the treatment strategy for comminuted cricoid fractures. Therefore, we considered these 2 functions in isolation, taking into account the cricoid structure that was important for each function. For the airway, it is important for the internal diameter of the cricoid to be sufficiently wide.
The trachea maintains its internal diameter even though the chondral frame is only in its anterior half. 5 Hence, the airway is maintained mainly by the anterior arch at the level of the cricoid, making it difficult to reconstruct the shattered anterior arch of the cricoid with a broad lumen. The fragments of the anterior arch of the cricoid are too small and too thin to be fixed with plates or sutures. Furthermore, the commercially available laryngotracheal stents do not have a diameter that is broad enough to keep the anterior arch of the cricoid. On the other hand, since the anterior part of the cricoid maintains the airway, the arch of the cricoid does not require reconstruction into its original configuration.
In the current case, we created a laryngocutaneous fistula with comminuted fragments of the cricoid arch. The laryngocutaneous fistula is less likely to develop stenosis because it allows for the lumen of the laryngeal space to be sufficiently wide. Finally, we closed the cutaneous fistula using a local flap. We aimed to create a broad lumen by multistep surgery.
As a result, we achieved a sufficient internal diameter at the subglottic space. It has been reported that a similar surgery was able to close the tracheal framework defect to less than 50% of the whole circumference of the trachea without airway stenosis. 6 Although it is bothersome that a cutaneous fistula is created temporarily, a multistep surgery for airway reconstruction is a good treatment strategy to ensure safety and efficacy in obtaining an adequate airway.
For phonatory function, it is important that the vocal processes of the left and right arytenoids fit vertically and anteroposteriorly to prevent glottal insufficiency. Arytenoids are located on the posterior lamina of the cricoid. 7,8 Therefore, to improve phonatory function, it is important that the dislocated pieces of the posterior lamina of the cricoid be reduced and fixed firmly in its original configuration.
In the current case, we obtained a clear surgical field of the posterior part of the cricoid by opening the anterior arch of the cricoid and then corrected the fracture fragments. We fixed the pieces of the posterior lamina with sutures as opposed to plate fixation due to the lack of ossification of the cricoid because the patient was young. In addition, we could not obtain a broad working space during the operation. Therefore, we needed to use a small needle and thread, 9 as described above. As a result, we reconstructed the pieces of the posterior lamina of the cricoid and achieved a good phonatory function.
We found that the airway was maintained by the anterior part, and the phonatory function depended on the posterior part of the cricoid. This novel concept allows for the treatment goal to be more focused in cases of comminuted cricoid fractures. In surgical treatment planning, it is important that the anterior part of the cricoid be reconstructed with sufficient internal diameter. It is also important that the fragments of the posterior part of the cricoid be reconstructed in the correct position.
Footnotes
Authors’ Note
The corresponding author has obtained written informed consent that the patient provides patient information and images to be published.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by JSPS KAKENHI Grant Number JP21K16858.