
Abstract
We present a case of an 80-year-old female patient who had an extensive dural bleed after endoscopic sinus surgery. A review of the literature regarding the surgical tools and materials used to treat dural hemorrhage was performed. We describe our preferred method of using the combination of endoscopic bipolar, DuraGen Plus, and DuraMatrix to stop significant dural bleeding and show effective hemostatic regulation.
Introduction
The skull base is a critical region between the anterior portion of the brain and the posterior area of the nose, mouth, and throat. Endoscopic sinus surgeries are difficult procedures that require appropriate hemostasis for their success. To provide the best outcome in hemorrhagic complications, the selection of suitable surgical material and equipment is of utmost importance for the success of these surgeries. 1 We now report a case of a patient who had an excessive dural bleed after endoscopic sinus surgery and were treated with appropriate equipment and technique with consideration to the patients’ religious restrictions as a Jehovah’s Witness. This religion believes that it is against God’s will to receive blood, even if it’s the patient’s own blood products.
Case
An 80-year-old female patient presented with a frontal sinus mass (Figures 1 and 2). The mass was biopsied for marginal zone lymphoma with extranodal involvement of the left orbit. The patient completed her chemotherapy 2 months prior. She presented to the emergency department with left preseptal cellulitis for 3 days with significant eyelid swelling and ecchymosis (Figure 3).
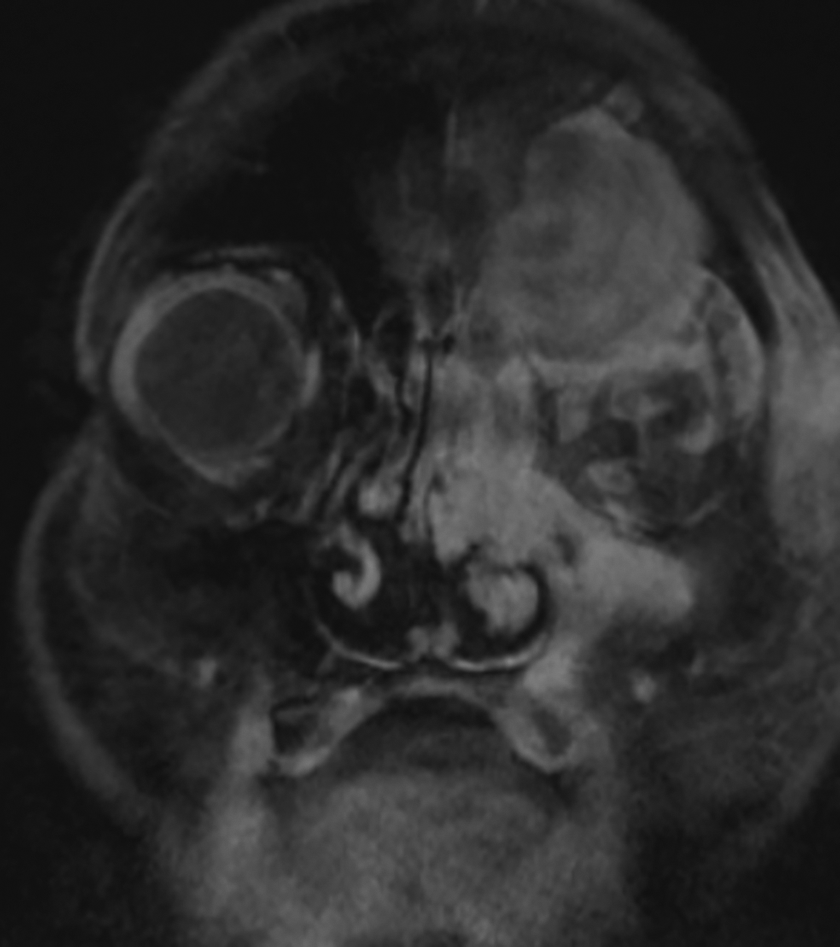
Magnetic resonance imaging (MRI): left ethmoid frontal sinus mass.
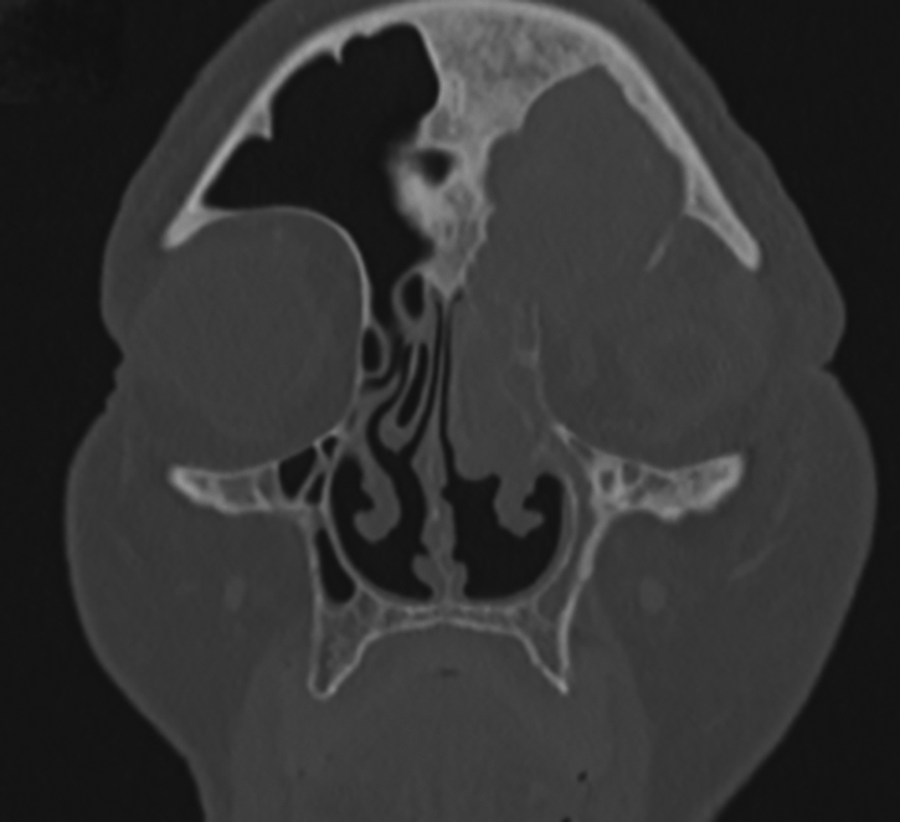
Computed tomography (CT) imaging.

Left eye preseptal celluitis.
The patient was taken to the operating room by another otolaryngologist where an endoscopic sinus surgery and washout were performed. The intraoperative findings included extensive osteoneogenesis of the frontal recess with inflamed mucosa that limited the visibility of the operating area. The patient had bleeding of the dura that occurred during the frontal sinus drill-out, without an obvious cerebrospinal fluid (CSF) leak; therefore, the frontal sinus was packed with gel foam.
Postoperatively, the patient had constant serosanguinous drainage and clear rhinorrhea, concerning possible CSF leakage. The patient began to develop shortness of breath, and there was a significant drop in the postoperative hemoglobin, requiring a blood transfusion. The patient was a Jehovah’s Witness and refused the transfusion. The hematologists recommended intravenous iron, folate/B12, epoetin alfa, desmopressin acetate, and aminocaproic acid, which were administered.
On the following day, the patient was taken to the operating room for exploration and repair of the skull base defect by the senior surgeon (J.D.S.). The cavity was inspected and the nasal packing was removed. The exposed dura continued to bleed from within the frontal sinus. A malleable endoscopic suction bipolar was used for hemostasis on the dura. DuraGen Plus (Integra Lifesciences) was then used as in inlay, followed by DuraMatrix (Stryker) as an overlay to repair the skull base defect. Additionally, Tisseel sealent and a frontal sinus spacer with gel foam were placed in the area. The packing and spacer were left for 2 weeks and then removed. The patient was doing well postoperatively with no recurrent bleeding or CSF leak after 6 months.
Discussion
Hemostasis is crucial in any surgical procedure, especially in endoscopic sinus surgery. In these operations, hemostatic regulation can be the determining factor for the success of surgical treatment. Although blood transfusions are rare in endoscopic sinus surgery, transfusions are usually required in preoperative anemic patients and in trauma cases. 2 The deep religious convictions of Jehovah’s Witness are against accepting homologous or autologous whole blood, packed red blood cells, or platelets. However, the religious understanding does not prohibit the use of albumin, immune globulins, and factor replacement for hemophilia treatment.
Postoperative hemorrhage can be a serious complication that can present in the recovery room after endoscopic sinus surgery, requiring urgent decompression. 3 The selection and combination of appropriate tools and supplies are crucial to effectively stop hemorrhagic obstacles. According to Zymberg et al, after the accurate identification of a dural bleed, the use of an endoscopic bipolar is necessary to stop high flow dural hemorrhage. 4 In a literature search, there were no reported cases that used the specific combination of endoscopic bipolar, DuraGen Plus, and DuraMatrix to stop significant dural bleeding after endoscopic surgery. DuraGen Plus is a soft, malleable, and absorbent collagen matrix that is used to repair dural defects, while DuraMatrix is resorbable collagen used for mechanical strength in the dural region. The use of DuraGen Plus as a semimalleable sheet to close the frontal sinus cavity is a great tool to isolate the frontal sinus and eliminate CSF leakage. 5 We found that the use of DuraMatrix as an overlay above the DuraGen Plus is an effective method for CSF leak repair in areas where vascularized pedicled flaps are not available or required.
Footnotes
Authors’ Note
This manuscript is original and has not been submitted elsewhere in part or in whole.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.