
Abstract
Pott’s puffy tumor is a potential complication of acute frontal sinusitis, characterized by subperiosteal abscess and osteomyelitis of the frontal bone. It can be managed with a combination of open and endoscopic sinus surgery and intravenous antibiotic therapy. In the current report, a 15-year-old male presented with a classic case of Pott’s puffy tumor which was managed with bilateral ethmoidectomies, frontal sinusotomies, and frontal sinus trephination, resulting in discharge on intravenous antibiotic therapy and subsequent complete resolution of symptoms.
Introduction
Frontal sinus pathology can be complex and varied, which can introduce associated complications. Common pathological conditions of the frontal sinus include acute bacterial, acute invasive fungal or allergic fungal, or chronic rhinosinusitis. 1 Complications can include preseptal cellulitis and postseptal abscess of the orbit, among others. Medical therapy is usually first line for the treatment of frontal sinusitis and its complications, including antibiotics when indicated, along with adjuvant topical nasal corticosteroids, decongestants, and mucolytics. 2 Surgery is employed when the condition is refractory to medical therapeutics and includes approaches such as endoscopic sinusotomy, balloon catheter dilation, and frontal sinus trephination. 3
Pott’s puffy tumor is an uncommon but serious potential complication of frontal sinusitis, characterized by subperiosteal abscess of the frontal region. Symptoms include frontal scalp swelling, headache, fever, nasal discharge, photophobia, and tenderness of the frontal sinus. The infection may travel from the sinuses to the periorbital space and result in orbital cellulitis or orbital abscess. It can also migrate through the diploe veins into the intracranial space and result in epidural, subdural, or brain abscess. Antibiotic therapy for sinusitis sometimes fails and then most patients require surgery. 4
Case
An otherwise healthy 15-year-old male presented to an outside Otolaryngology clinic complaining of nasal obstruction, congestion, and facial pain of 2 weeks duration. He was treated initially with a course of amoxicillin followed by azithromycin and prednisone, with no clinical improvement. After developing swelling of the right eye and forehead, he was transferred to a tertiary care center for further evaluation and management. On presentation, he complained of headache and was unable to open the right eye.
The patient’s vital signs were within normal limits; he was afebrile. He had normal mental status. Upon manually opening the patient’s right eyelid, the pupils were equal, round, and reactive to light, extraocular muscles intact and were noted to have right orbital proptosis. The left eye also exhibited periorbital edema but retained normal visual acuity and extraocular movements (Figure 1A and B). The nasal examination revealed purulent secretions in the middle meatus bilaterally as well as purulent secretions dripping down the oropharynx. There was no meningismus or cervical lymphadenopathy.

Preoperative photograph demonstrating significant forehead edema, right periorbital erythema, and inflammation.
The patient’s white blood cell count was elevated at 21.9 K/µL (normal 5.0-10.0 K/μL) with 69% neutrophils (normal 40%-60%), C-reactive protein level was elevated at 8.41 mg/dL (normal 0.3-1.0 mg/dL), and his COVID-19 test was negative.
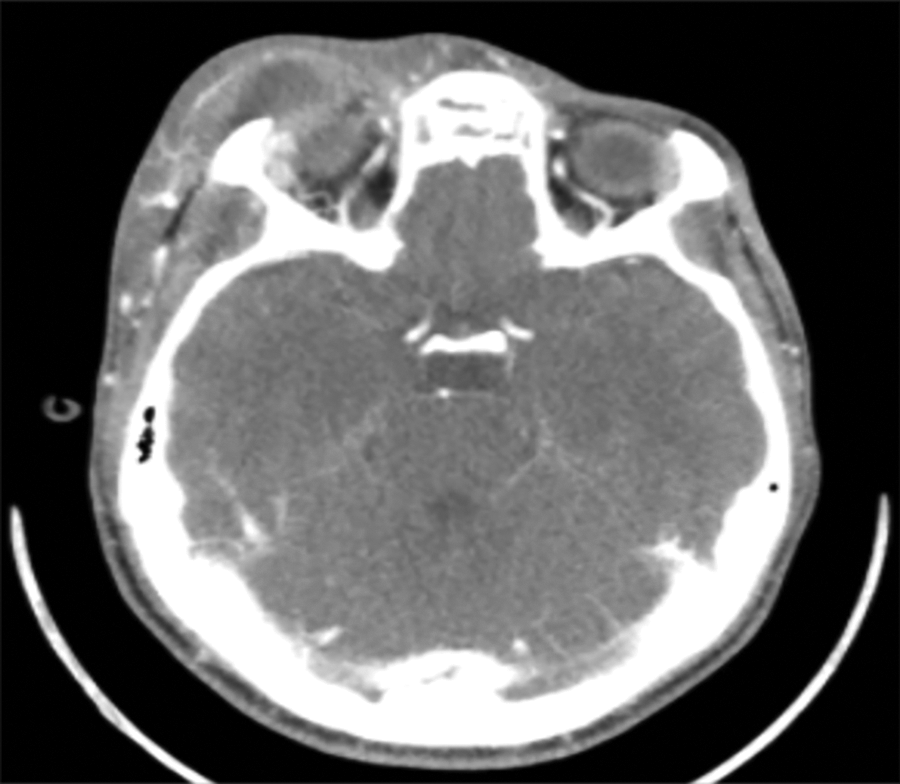
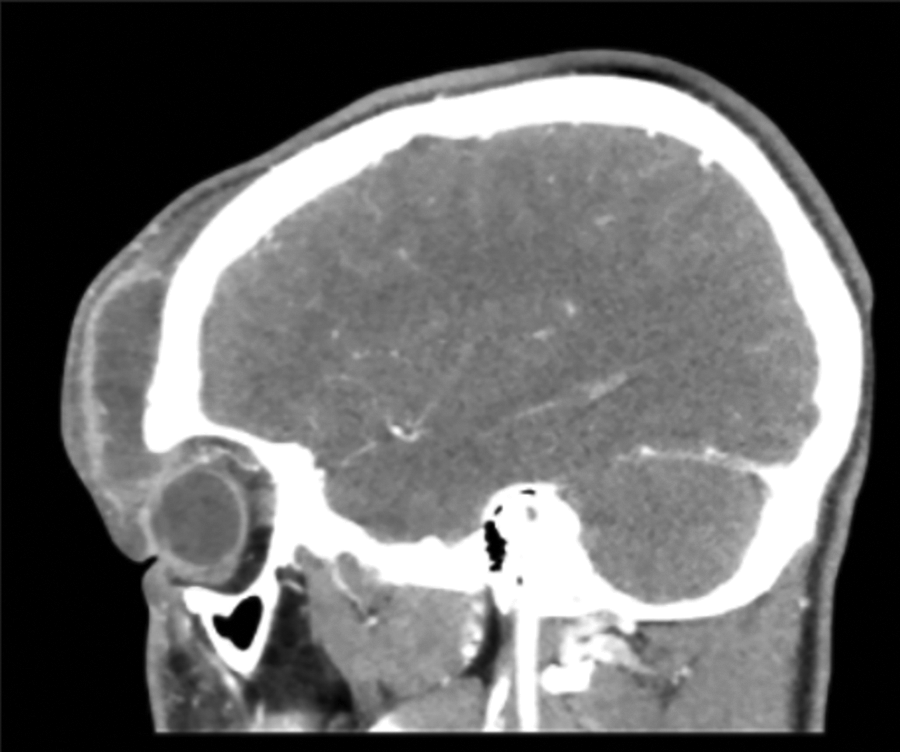
A computed tomography (CT) scan with contrast was performed and revealed a rim-enhancing fluid collection over the right frontal bone that measured 2.0 × 5.2 × 5.2 cm (Figure 2). The bone beneath the fluid collection demonstrated a permeative pattern of destruction with multiple areas of cortical breakdown along with the anterior table, involvement of the diploic space, and several small foci of dehiscence of the posterior table. There was adjacent dural enhancement but no evident intracranial fluid collection. There was complete opacification of both frontal sinuses and the anterior ethmoid air cells bilaterally (Figure 3).
Sagittal computed tomography (CT) scan with contrast through the right orbit demonstrating significant frontal abscess with rim enhancement.
Axial computed tomography (CT) scan with contrast through the orbit demonstrating periorbital edema and fluid collection.
The patient was admitted for intravenous (IV) antibiotic therapy with vancomycin, ceftriaxone, and metronidazole. He was also treated with a nasal decongestant (oxymetazoline), a steroid spray, and saline rinses. The patient was subsequently taken to the operating room for bilateral endoscopic ethmoidectomies and frontal sinusotomies with image guidance, a right medial eyebrow incision and drainage of the forehead and the right orbital subperiosteal abscess, as well as an endoscopically assisted frontal sinus trephination with complete washout. A Penrose drain was placed in the subperiosteal space, and a butterfly catheter was inserted into the frontal sinus. Cultures were obtained and grew Streptococcus intermedius, a highly pyogenic gram-positive microaerophilic bacteria of the Streptococcus viridans group.
Following surgery, the patient remained admitted for continued IV antibiotic therapy. Additionally, the frontal sinuses were irrigated with oxymetazoline and saline twice daily via the butterfly catheter that was left in place. The drain and catheter were removed on postoperative day 4 as he demonstrated significant improvement, and a peripherally inserted central catheter (PICC line) was placed on the same day. The patient was discharged the next day on IV ceftriaxone 2 grams every 24 hours and IV metronidazole 500 mg every 8 hours via the PICC line for 6 weeks. The patient did very well at the 6-week follow-up time point, with complete resolution of symptoms.
Discussion
This patient was determined to have a Pott’s puffy tumor, first described by Sir Percivall Pott in 1760 as well as on several subsequent occasions. 5,6 It is a rare clinical entity characterized by subperiosteal abscess associated with osteomyelitis of frontal bone. It is usually seen as a complication of frontal sinusitis predominantly in the adolescent age group. It can be associated with cortical vein thrombosis, epidural abscess, subdural empyema, and brain abscess. The primary presenting feature is circumscribed, tender swelling of the forehead, often associated with fever, headache, nasal discharge, or elevated intracranial pressure. Most common etiologies include infection and trauma. Head CT and brain magnetic reonance imaging are appropriate imaging techniques utilized for diagnosis, and management usually consists of surgery and broad-spectrum antibiotic therapy. 7
The combination of ceftriaxone and clindamycin can be used to treat frontal sinusitis. In areas where methicillin-resistant Staphylococcus aureus (MRSA) isolates are typically resistant to clindamycin, vancomycin should be used in addition to ceftriaxone. Ampicillin/sulbactam is an acceptable alternative if MRSA is not suspected. Combination therapy with vancomycin, ceftriaxone, and metronidazole provides coverage for most intracranial pathogens complicating acute bacterial sinusitis. In the current case, metronidazole was chosen to be added to ceftriaxone as a first attempt in order to provide wide coverage. Also, supplementary saline nasal irrigation has previously been reported to serve as a beneficial adjunct for resolution of such abscesses. 8
Footnotes
Authors’ Note
This manuscript is original and has not been submitted elsewhere in part or in whole.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.