
Abstract
Balloon sinus dilation (BSD) is a common method of relieving sinus outflow obstruction. With the rising utilization of BSD, increasing numbers of BSD-related complications have also been reported. Here, we report a case of pneumocephalus and cerebrospinal fluid leak following BSD of the frontal sinus. Additionally, a review of the literature regarding BSD complications was performed.
Introduction
Balloon sinus ostial dilation (BSD) is considered a minimally invasive technique for the treatment of chronic rhinosinusitis (CRS). 1 Balloon sinus dilation was approved by the United States Food and Drug Administration (US FDA) in 2005 and involves the use of navigation or transillumination to place the dilation device into the natural ostium of the sinus being treated in order to relieve the obstruction. 1 Potential benefits of BSD include the ability to perform the procedure under local anesthesia in the office setting, reduced need for postoperative debridement, and less mucosal trauma than traditional endoscopic sinus surgery. 2 As BSD became more popular reports of complications associated with BSD began to emerge. 3 Subsequently, a Manufacturer and User Facility Device Experience database review identified 211 total adverse events associated with BSD between 2008 and 2018. 4 Cerebrospinal fluid (CSF) leak, eye swelling, and epistaxis were the most commonly reported complications, and dilation of the frontal sinus was noted as the most common site associated with patient complications. 4 The purpose of this report is to describe a case of pneumocephalus and CSF leak following in-office BSD of the frontal sinus.
Case Report
A 76-year-old male with a history of CRS underwent BSD of the bilateral maxillary, sphenoid, and frontal sinuses at an outside facility. The procedure reportedly went well and transillumination was used to confirm proper placement in both the maxillary and frontal sinuses. Immediately following the BSD, the patient was noted to have a large amount of clear fluid draining from his left nostril. Computed tomography (CT) scan was obtained and demonstrated a large amount of pneumocephalus. The patient was subsequently transferred to University of California Los Angeles Ronald Reagan Medical Center for further evaluation and management of the suspected skull base injury. On arrival, the patient complained of mild headache and was noted to have altered mental status. On examination, there was copious clear rhinorrhea on the left side. A subsequent dedicated sinus CT scan showed worsening intracranial air with concern for tension pneumocephalus and a defect in the left cribriform (Figure 1). The frontal sinus anatomy included a large agger nasi and type I frontal cell with a narrow medial drainage pathway. Due to his worsening mental status and progression of pneumocephalus, the patient was prepared for emergent operative repair of the skull base.
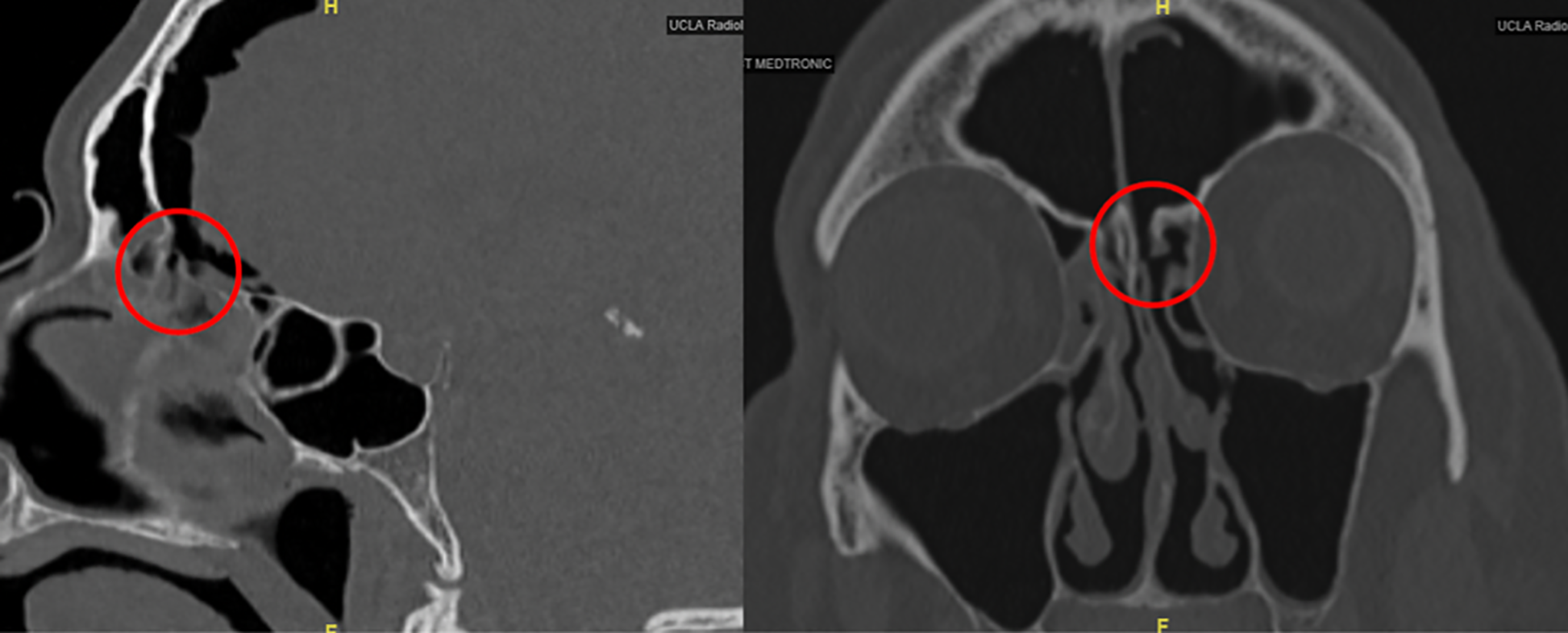
Progressive pneumocephalus with left cribriform skull base defect.
A complete bilateral endoscopic sinus surgery was conducted in order to examine the entire skull base. Upon inspection of the right skull base, there was no evidence of CSF leak. Inspection of the left skull base identified a defect in the left cribriform that corresponded to the area of concern on the CT scan and was verified with intraoperative navigation (Figure 2). The defect was circular and measured approximately 5 × 5 mm. The mucosa surrounding the defect was stripped circumferentially, and bipolar cautery was used to achieve hemostasis. A left-sided nasoseptal flap was then harvested and rotated to repair the skull base. Fibrin sealant, gelfoam, and finger cot were then placed to buttress the flap.
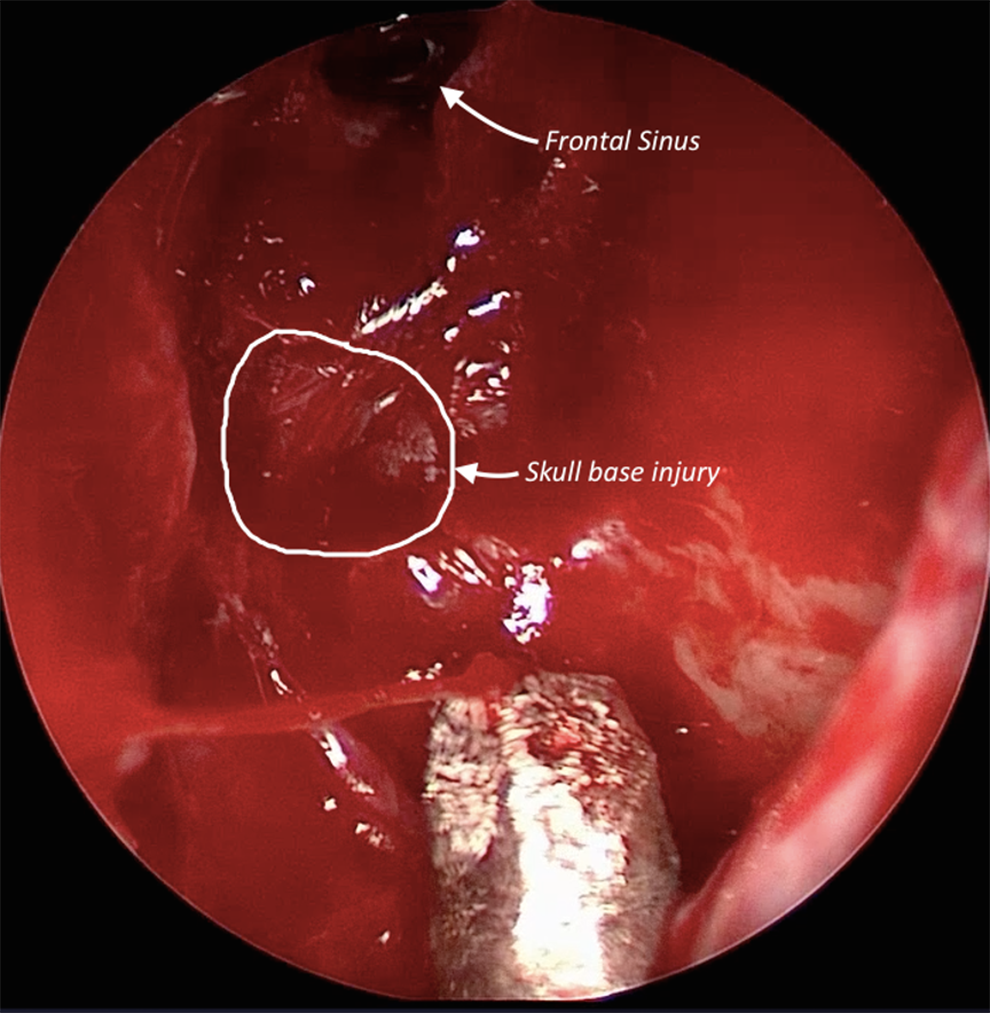
Endoscopic view of the skull base injury.
Postoperatively, the patient was observed in the neurosurgical intensive care unit where his mental status returned to baseline over the first 48 hours. The patient had no recurrent CSF leak and developed no long-term sequelae as a result of the injury.
Discussion
The utilization of BSD has increased dramatically since the initial approval by the US FDA in 2005. Distinct Current Procedural Terminology codes were introduced for BSD in 2011, and between 2011 and 2015 BSD utilization increased more than 5-fold. 5 Small studies have demonstrated noninferiority of BSD when compared with traditional endoscopic sinus surgery techniques. 6 -8 However, successful BSD begins with appropriate patient selection. Balloon sinus dilation is most appropriate for patients who do not require tissue removal from the sinuses. 1,9 Patients with nasal polyps, fungal balls, or allergic fungal sinusitis have not been considered to be optimal candidates for BSD as it is unable to fully eradicate the disease. 1
As the number of BSD cases has increased, so have the number of BSD-related complications. 4 Initial studies reported that complication rates with balloon sinuplasty were as low as 0.01%. 10 Although rare, these complications are not insignificant. Alam et al 3 described 5 cases of patient-related complications from BSD. Two of these cases involved orbital complications (severe bilateral pneumo-orbita and extraocular muscle entrapment resulting in diplopia). The 3 other cases developed complications related to skull base injury and CSF leak. One patient ultimately succumbed to his injuries due to brain herniation after the placement of a lumbar drain. As such, care should be taken when evaluating patients for BSD-related complications, and if pneumocephalus is present, placement of a lumbar drain should be avoided as it may significantly exacerbate intracranial hypotension and lead to cerebral herniation. 11
Several large database studies have recently investigated the rates of BSD-related complications and have identified that BSD of the frontal sinus is particularly prone to increased risk of complications. 4,12,13 In the largest database study to date investigating BSD complications, Chaaban et al 13 identified a complication rate of 0.35% for skull base complications, 2.95% for orbital complications, and 2.03% for bleeding complications of 2851 total procedures studied. Another database study identified a total of 102 patient-related complications reported to the FDA between 2008 and 2018. 4 The most common patient-reported complications were CSF leak in 36.3%, orbital swelling in 29.4%, and epistaxis in 11.8%. Cerebrospinal fluid leak was more commonly associated with dilation of the frontal sinus (67.6%), and orbital swelling was most commonly associated with maxillary sinus dilation (56.7%). Nearly 50% of the most common complications occurred during dilation of the frontal sinus. 4 Variable anatomy of the frontal recess and necessity of using angled endoscopes and instruments may be reasons why frontal sinus BSD seems to have increased complication rates. Thus, the importance of appropriate patient selection, careful review of individual patient anatomy, proper training on the use of the device, interpretation of real-time navigation or transillumination cannot be underscored, and timely recognition and management of complications is critical to prevent any long-term adverse sequelae.
The management of BSD-related complications is dependent on several factors. Orbital complications can often be managed with watchful waiting; however, surgeons should be prepared to perform lateral canthotomy and cantholysis should retroorbital hematoma or increased orbital pressure place the eye at risk of permanent vision loss. In fact, in one study 26.7% of patients with orbital swelling required lateral a canthotomy. 4 Skull base complications and CSF leak should be repaired once identified to prevent potential complications (ie, pneumocephalus, meningitis, intracranial abscess). In most cases, CSF leak will occur in low-flow sites and patients will not be at risk of having elevated intracranial pressure, thus simple overlay repairs with free- or local-pedicled mucosal grafts are sufficient to repair the leak. Following repair, patients should be observed overnight in the hospital and CT scan should be obtained to rule out any intracranial complications and ensure resolution of any pneumocephalus.
Conclusion
Balloon sinus dilation is a useful procedure in a unique subset of CRS patients. Surgeons, however, must be aware of the potential complications, including skull base injury. Timely diagnosis and management of such complications are crucial to preventing long-term adverse sequelae. Lumbar drains should be avoided in cases where pneumocephalus is present due to risk of brain herniation.
Footnotes
Authors’ Note
This manuscript is original and has not been submitted elsewhere in part or in whole.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.