
Abstract
Background:
Laryngocarcinoma (LC) is a common malignant tumor of the head and neck, accounting for 1% to 5% of human tumors. The primary objective of the present study was to evaluate the survival time of patients with LC at different sites.
Methods:
Information concerning patients with LC was extracted from the Surveillance, Epidemiology, and End Results (SEER) database between 1975 and 2016.
Results:
In total, 16 255 patients with LC were selected from the SEER database. Among all patients, 80.2% were male; males also predominated in each tumor site subgroup. Most of the patients were aged between 60 and 69 years, had white ethnicity, were single, and had American Joint Committee on Cancer (AJCC) stage I cancer with T1, N0, and M0. The present study investigated the role of interventions in all LCs at different AJCC stages. Across the whole population, regardless of the intervention used, survival increased in patients at any cancer site.
Conclusions:
The study found that male sex, age ≥80 years, black ethnicity, single status, T4, N4, M1, and AJCC stage IV were associated with higher mortality rates at all sites of LC. Aggressive interventions, especially surgery and radiotherapy, may improve survival in patients with LC at different sites and with different AJCC stages.
Background
Laryngocarcinoma (LC) is a common malignant tumor of the head and neck, accounting for 1% to 5% of human tumors. It is the third commonest malignant tumor in departments of otolaryngology and head and neck surgery. 1 Regarding pathological type, 98% of LCs are squamous cell carcinoma, while the glottis is the commonest site. 2
In recent years, the incidence of LC has risen due to social changes, serious environmental pollution, and other factors. As such, LC has seriously impacted the health of the world’s population. Difficulty breathing, hoarseness, blood in sputum, and enlargement of neck lymph nodes are all common symptoms of this disease that can have a serious impact on the life of patients. 1 The techniques used to treat LC have gradually improved; in most cases, surgery is performed to control disease progression and improve prognosis. Small tumors can be treated using surgery or radiation, while moderate tumors can be treated using partial laryngectomy and larger tumors using total laryngectomy. At present, the main treatment for patients with advanced LC is surgery followed by radiotherapy and chemotherapy. However, it remains unclear whether this approach is effective. 3 The primary objective of the present study was to evaluate the survival time of patients with LC at different sites. Determining survival differences among patients with LC treated using different methods has led to new challenges in therapeutic choice.
Material and Methods
Data Source
Data were obtained from the Surveillance, Epidemiology, and End Results (SEER) database, which contains the clinical characteristics of many patients with tumors and has contributed significantly to reducing the burden of cancer. SEER*Stat software version 8.3.5 (http://seer.cancer.gov/seerstat/) was used to select patients with LC registered between 1975 and 2016, extract relevant data, and analyze the variables. All cases were from the SEER 18 Registers Research Data plus the Hurricane Katrina Impacted Louisiana Cases, Nov 2018 Sub (1973-2016) database.
Patient Selection and Classification
Patients with a histological diagnosis of LC between 1975 and 2016 were selected for this study. Those who were diagnosed with LC at the stage of biological death or at autopsy were excluded, as were those with any of the following criteria: (1) unknown treatment modality, (2) unclear survival time, (3) unknown TNM stage according to American Joint Committee on Cancer (AJCC; seventh edition, 2010), (4) unclear summary stage, (5) unknown treatment status, and (6) unclear tumor size. Ultimately, 16 714 patients were eligible for enrolment.
The patients were categorized into 5 age groups: 0 to 39, 40 to 49, 50 to 59, 60 to 69, and 70+ years. Other subgroup analyses were carried out based on ethnicity (black, white, other), marital status (married or single), tumor grade according to the AJCC seventh edition (grade I, II, III, and IV), tumor stage (T1, T2, T3, and T4), node stage (N0 and N1), metastatic stage (M0 vs M1), surgery (yes/no/unknown), chemotherapy (yes/no/unknown), radiation (yes/no/unknown), and survival time.
Statistical Analysis
All statistical analyses were conducted using R (version 3.6.0; R Foundation) to depict survival curves. Chi-square analysis was used to analyze and evaluate the clinical characteristics of patients with LC who received various treatments, and the results were considered statistically significant when P value was <.01. 4 Hazard ratios and 95% CIs were calculated using univariate and multivariate Cox proportional risk models to assess each independent prognostic correlate. In the SEER database, extracted data, such as patient age, race, sex, grade, and prognostic value of the treatment, are commonly assessed using the Cox proportional hazards model and Kaplan-Meier curve to determine their relationship with overall survival (OS) in different cohorts. 5
Nomogram Construction
Nomograms play a major role in predicting patient survival. Using the R 3.1.1 package, which incorporates all individual prognostic factors, novel nomograms were constructed that could forecast OS in patients with LC.
Results
Baseline Characteristics
The 16 255 patients had LC in the following sites: 8454 glottic, 5893 supraglottic, 289 subglottic, and 1619 others. The basic characteristics of patients from the SEER database that met the eligibility criteria are shown in Table 1.
The Entire Cohort and Basic Characteristics of Laryngocarcinoma.
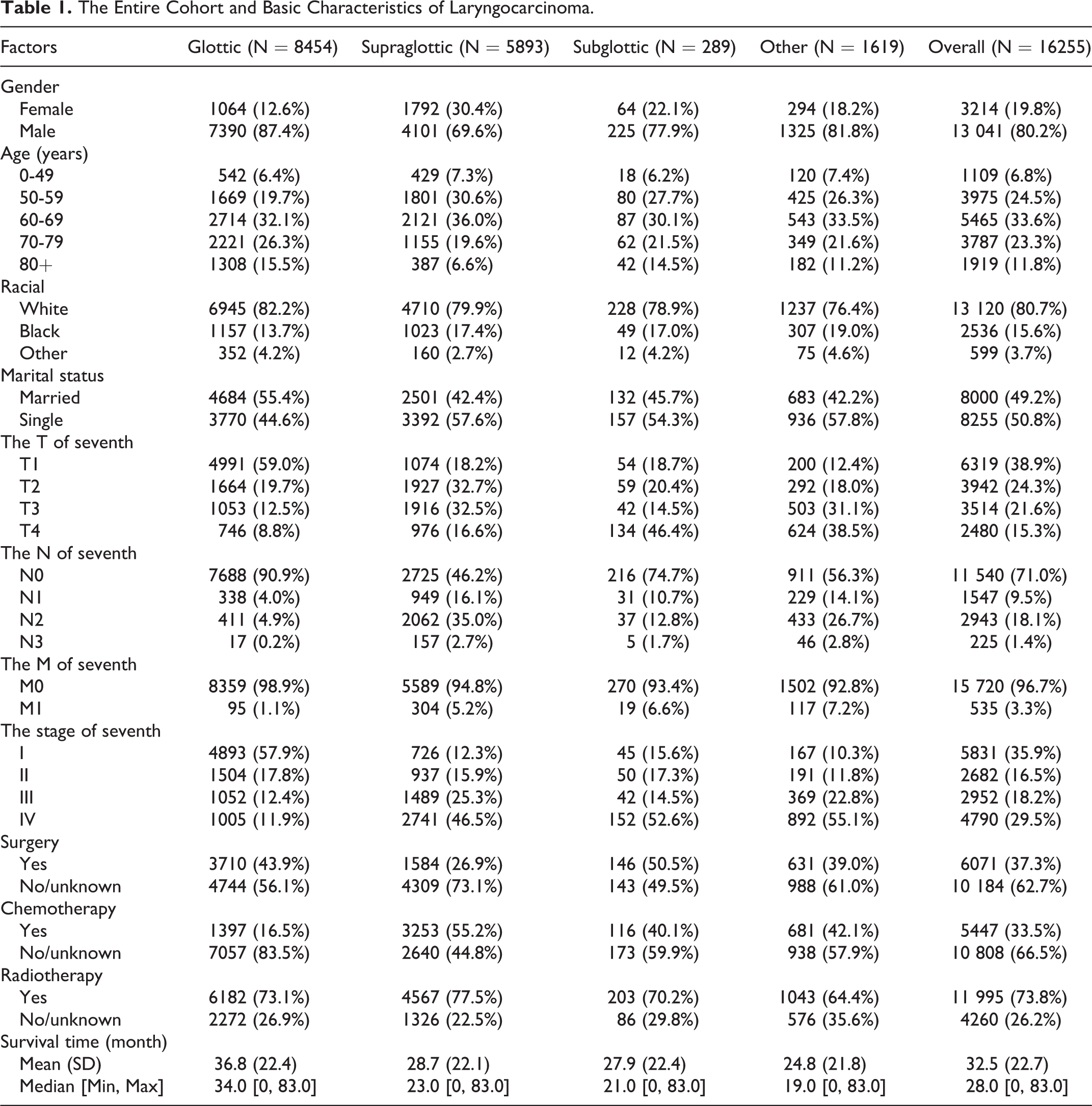
Among all patients, 80.2% were male; males also predominated in each tumor site subgroup. In terms of age, the highest proportion of patients were aged 60 to 69 years (33.6%), followed by those aged 50 to 59 years (24.5%), and those aged 70 to 79 years (23.3%), a relatively low proportion were aged ≥80 years (11.8%) and 0 to 49 years (6.8%). Most of the patients (80.7%) were white, and about half were married, while the other half were single. According to the tumor pathology report, the highest proportion of cancers was grade I (35.9%), followed by grade IV (29.5%). Regarding TNM stage, most patients were in the early stages of LC; that is stage I, T1 (38.9%), N0 (71.0%), and M0 (96.7%). In terms of treatment, radiotherapy was chosen in 73.8% of patients, whereas chemotherapy was used in 66.5% of patients in a no or unknown state, and 37.3% received radiotherapy, which was not performed or unknown in 97.5% of cases. For overall LC, the survival time was 32.7 months. Among all patients, those with glottic carcinoma had the longest survival time (36.8 months).
Cox Proportional Hazards Model
Table 2 presents univariate and multivariate regression analyses of patients with LC, with OS as the end point. In the univariate analysis of glottic and supraglottic sites, sex, age, race, AJCC stage, TNM stage, surgery, radiotherapy, chemotherapy, and marital status (P < .05) were significantly related to OS. In the univariate analysis of the subglottic site, age, AJCC stage, TNM stage, radiotherapy, and marital status (P < .05 in all cases) were significantly different from the OS distribution, while sex (P = .347), race (P = .842), surgery (P = .07), and chemotherapy (P = .75) were not. In the univariate analysis of the other sites, age, AJCC stage, TNM stage, surgery, chemotherapy, radiotherapy, and marital status were significantly different from the OS distribution (P < .05 in all cases), while sex (P = .777) and race (P = .142) were not. In the multivariate analyses, certain clinical traits were no longer independent prognostic factors, but there were still some variables with remarkable predictive value (P < .001).
Univariable Analyses of Overall Survival in the Whole Cohort of Laryngocarcinoma.
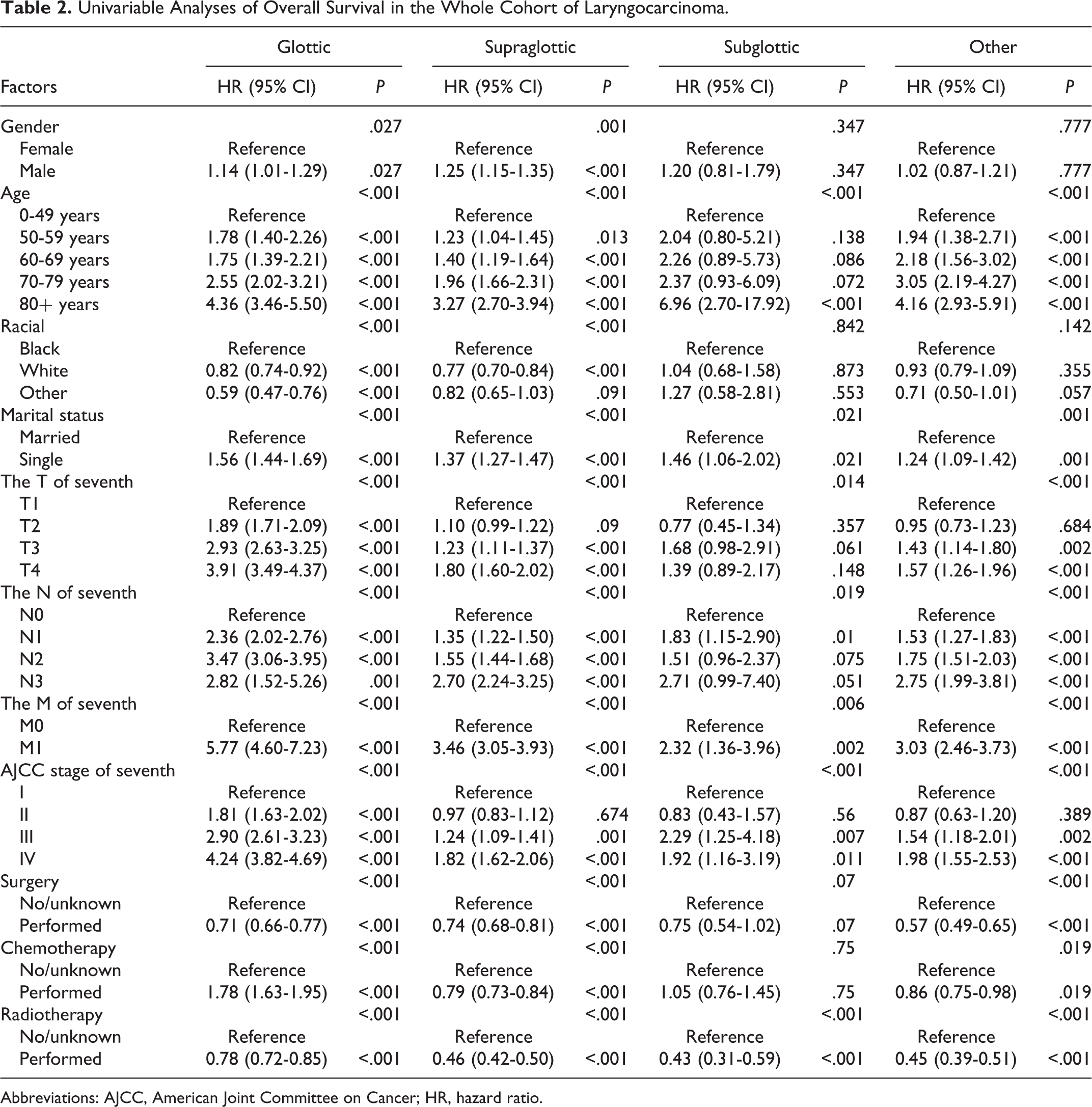
Abbreviations: AJCC, American Joint Committee on Cancer; HR, hazard ratio.
Data from multivariate analysis in Table 3 indicate that male were more likely to develop LC than female (glottic: hazard ratio [HR] = 1.17, 95% CI = 1.07-1.32, P = .014; supraglottic: HR = 1.27, 95% CI = 1.17-1.38, P < .001; other site: HR = 1.17, 95% CI = 1.03-1.62, P = .785), but there was no difference in the incidence of subglottic LCs between the sexes (HR = 1.06, 95% CI = 0.69-1.62, P = .785). Compared to patients in the 0 to 49 years age group, those in the other 3 age groups were more likely to develop LC, as follows: 50 to 59 years (glottic: HR = 1.66, 95% CI = 1.30-2.11, P < .001; supraglottic: HR = 1.21, 95% CI = 1.03-1.42, P = .024; other site: HR = 1.66, 95% CI = 1.30-2.11, P < .001; subglottic [not significant]: HR = 2.16, 95% CI = 0.82-5.65, P = .117), 60 to 69 years (glottic: HR = 1.90, 95% CI = 1.50-2.39, P < .001; supraglottic: HR = 1.40, 95% CI = 1.19-1.64, P = .002; other site: HR = 1.90, 95% CI = 1.50-2.39, P < .001; subglottic [not significant]: HR = 2.26, 95% CI = 0.87-5.87, P = .094), 70 to 79 years (glottic: HR = 3.13, 95% CI = 2.48-3.95, P < .001; supraglottic: HR = 1.92, 95% CI = 1.67-2.33, P < .001; subglottic: HR = 3.02, 95% CI = 1.14-8.01, P = .026; other site: HR = 3.13, 95% CI = 2.48-3.95, P < .001), and ≥80 years (glottic: HR = 5.32, 95% CI = 4.21-6.72, P < .001; supraglottic: HR = 3.17, 95% CI = 2.62-3.84, P < .001; subglottic: HR = 8.74, 95% CI = 3.22-23.68, P < .001; other site: HR = 5.32, 95% CI = 4.21-6.72, P < .001). In black patients, supraglottic LC was less likely than in white patients (HR = 0.86, 95% CI = 0.78-0.94, P < .001), glottic LC, supraglottic LC, and other sites were not significantly different among races. The risk of death was higher in single patients than in married patients (glottic: HR = 1.40, 95% CI = 1.29-1.52, P < .001; supraglottic: HR = 1.30, 95% CI = 1.21-1.40, P < .001; subglottic: HR = 1.66, 95% CI = 1.15-2.40, P = .007; other: HR = 1.40, 95% CI = 1.29-1.52, P < .001). Higher TNM stage denoted poorer tumor condition, enhanced risk of death, and shorter survival in all tumors except subglottic LC. Table 3 presents detailed results in this regard. There was a wide variation in survival between patients who underwent surgery and those who did not (glottic: HR = 0.61, 95% CI = 0.56-0.66, P < .001; supraglottic: HR = 0.56, 95% CI = 0.51-0.61, P < .001; subglottic: HR = 0.67, 95% CI = 0.46-0.97, P = .036; other site: HR = 0.61, 95% CI = 0.56-0.66, P < .001). In all patients except those with subglottic LC, those who underwent chemotherapy showed better survival than those who did not or whose chemotherapy history was unknown (glottic: HR = 0.86, 95% CI = 0.77-0.97, P = .013; supraglottic: HR = 0.67, 95% CI = 0.62-0.74, P < .001; other: HR = 0.86, 95% CI = 0.77-0.97, P = .013). Patients who underwent radiotherapy showed better survival than those who did not or whose radiotherapy history was unknown (glottic: HR = 0.57, 95% CI = 0.52-0.63, P < .001; supraglottic: HR = 0.44, 95% CI = 0.40-0.48, P < .001; subglottic: HR = 0.45, 95% CI = 0.30-0.67, P < .001; other: HR = 0.57, 95% CI = 0.52-0.63, P < .001).
Multivariate Analyses of Overall Survival in the Whole Cohort of Laryngocarcinoma.
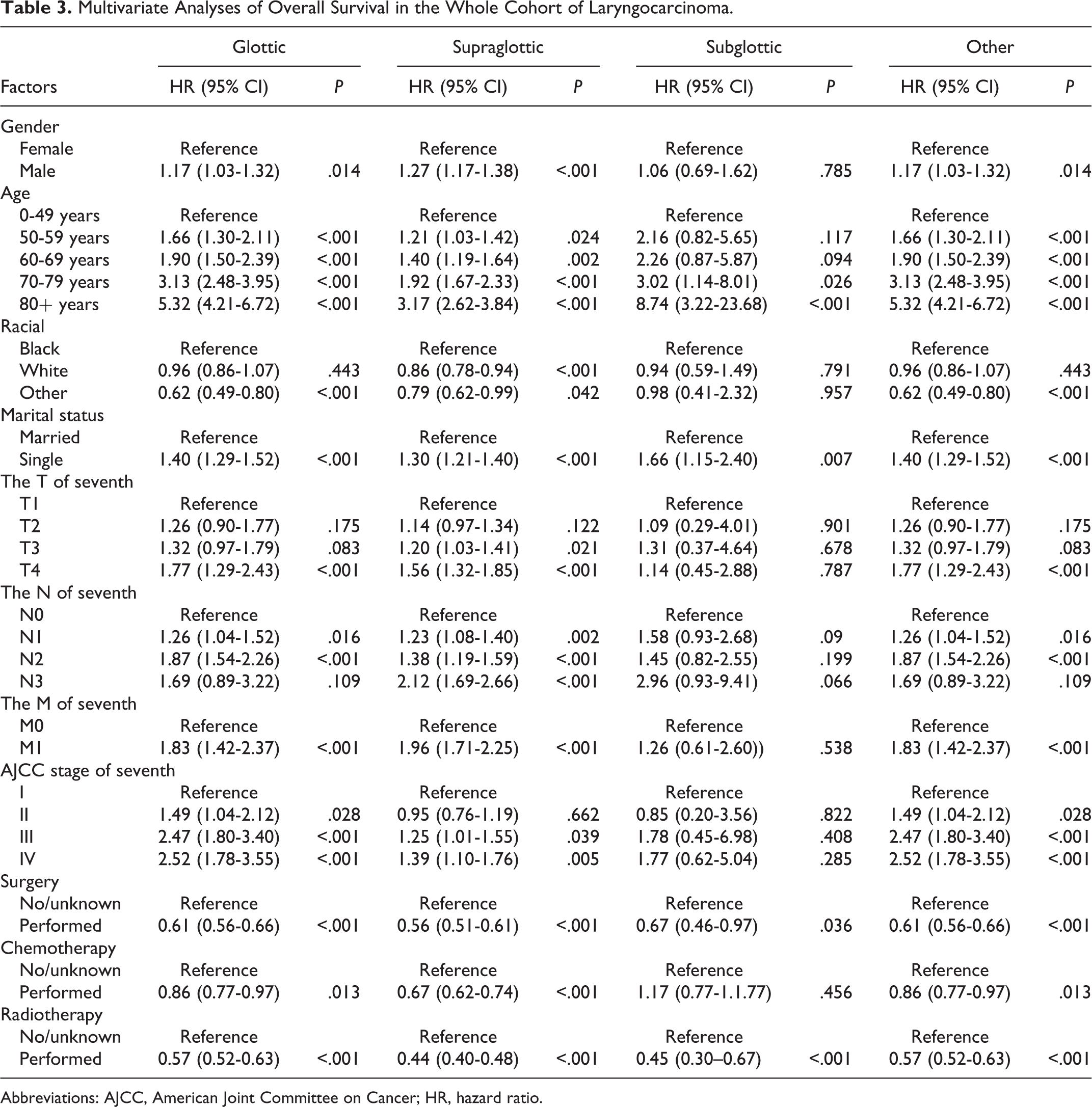
Abbreviations: AJCC, American Joint Committee on Cancer; HR, hazard ratio.
Kaplan-Meier Survival Analysis
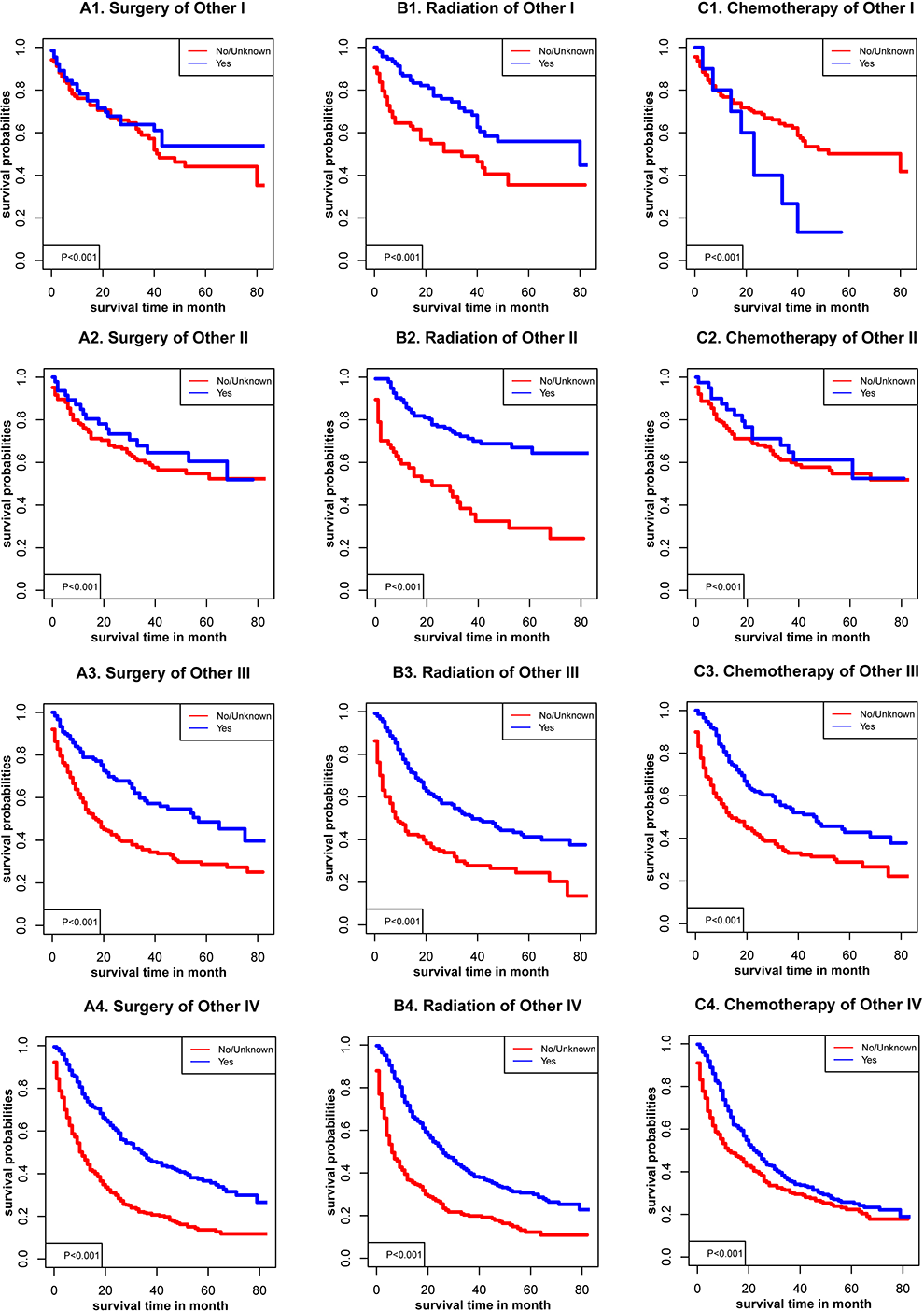
Sex, age, racial, AJCC stage, TNM stage, and marital status (P < .001) were significantly related to OS in glottic cancer (Figure 1), supraglottic cancer (Figure 2), subglottic cancer (Figure 3), and other cancer (Figure 4). Figure 5 showed the Kaplan-Meier survival curves, with or without interventions, at different LC sites. The curve shows that glottic cancer is highly survivable (P < .001), with or without intervention. Based on the different AJCC stages (Figure 6), there were differences in LC at different sites, regardless of whether any intervention was used (P < .001). Among patients with AJCC stage T1 to T3, survival was highest in those with glottic cancer and lowest in those with subglottic cancer. In patients with AJCC stage T4, the survival times of LCs at different locations were similar, but the survival rates of patients with supraglottic and glottic cancers were still higher than those of patients with other cancers. Figures 7 to 10 showed the role of interventions at different AJCC stages in all LCs. Among all patients, regardless of the intervention used, survival increased with intervention at any cancer site. Notably, chemotherapy did not improve survival in AJCC stage II glottic cancer (Figure 7), AJCC stage I and II supraglottic cancer (Figure 8), AJCC stage I and II subglottic cancer (Figure 9), and AJCC stage I other cancers (Figure 10).
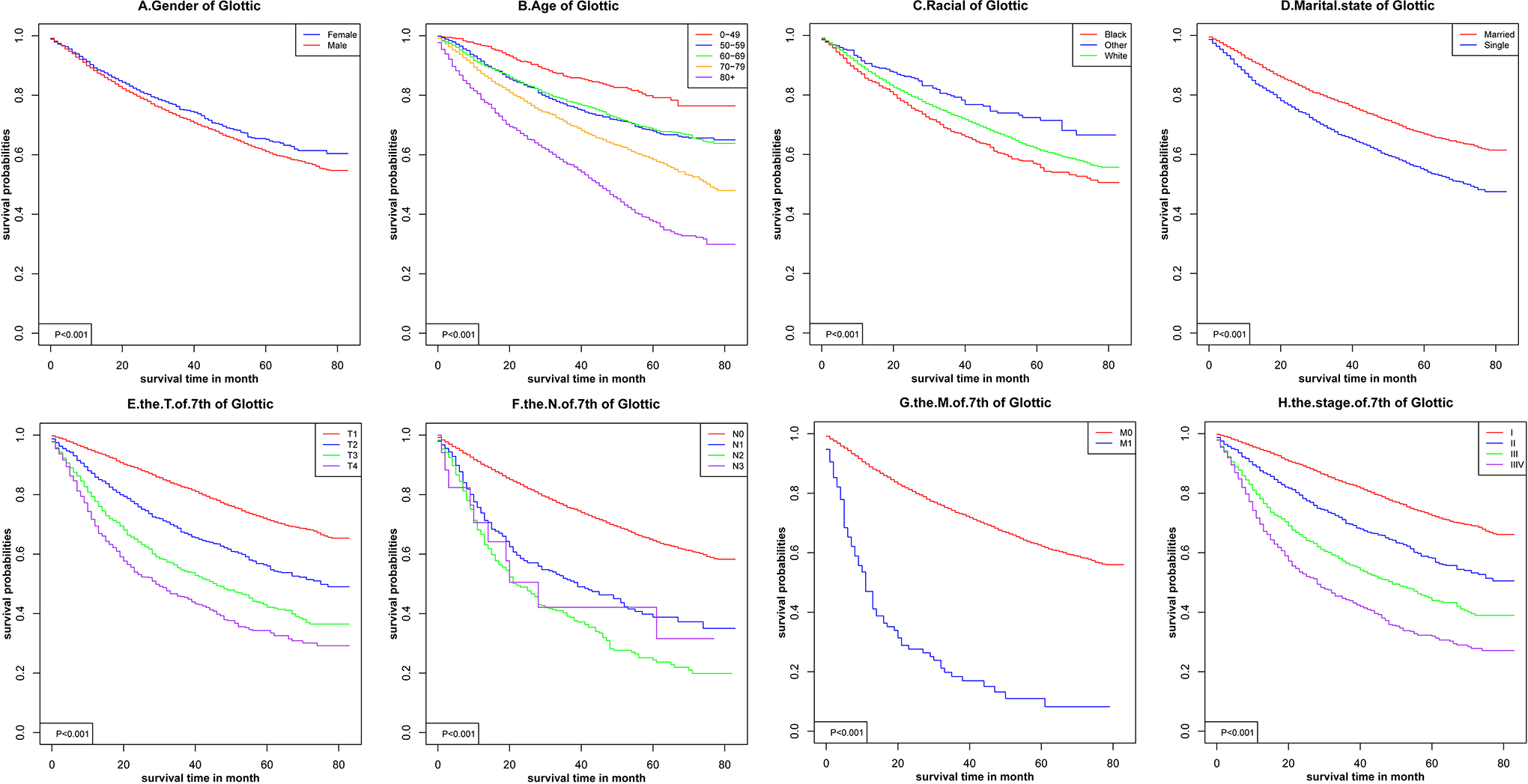
Kaplan-Meier survival curves for glottic cancer.
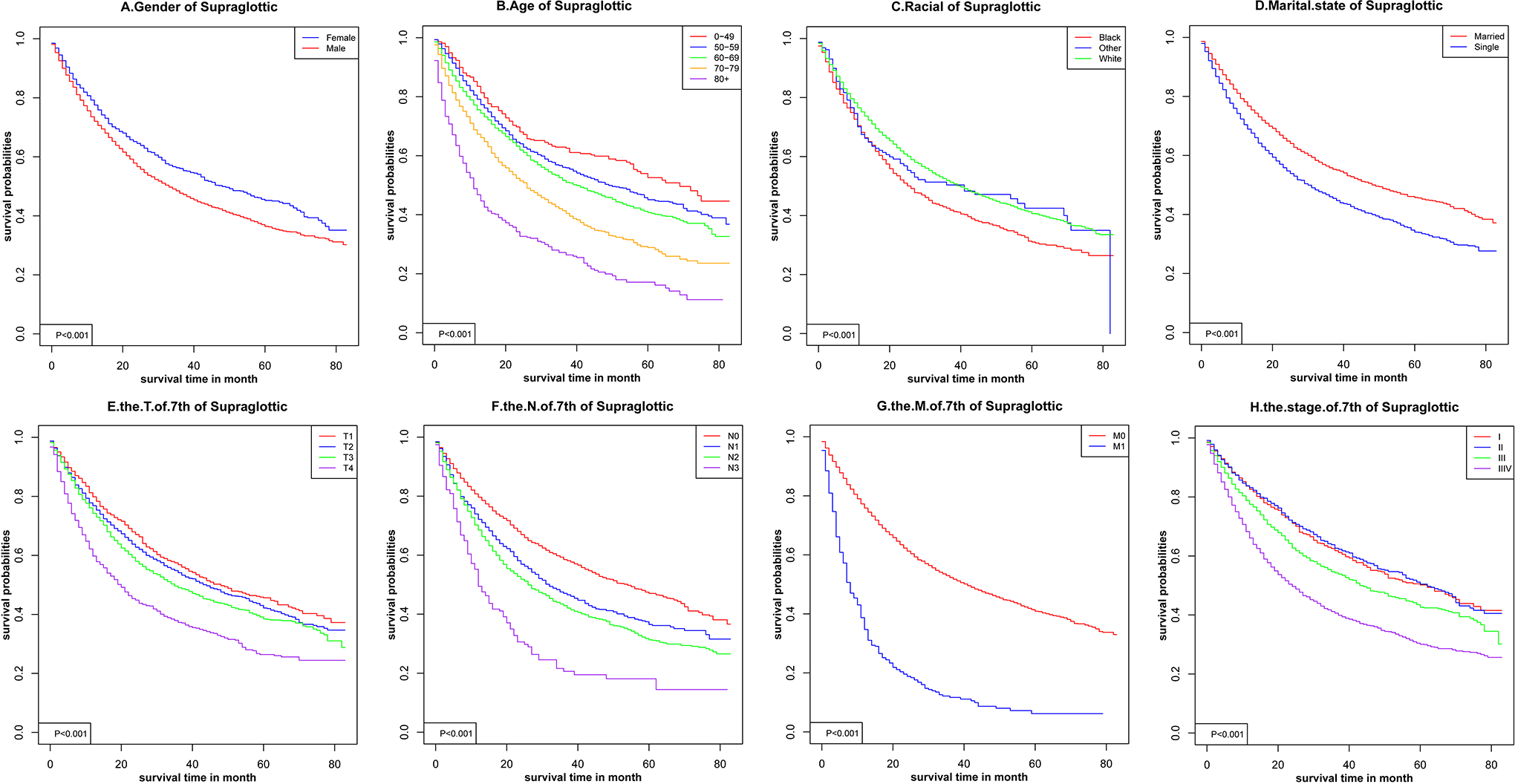
Kaplan-Meier survival curves for supraglottic cancer.
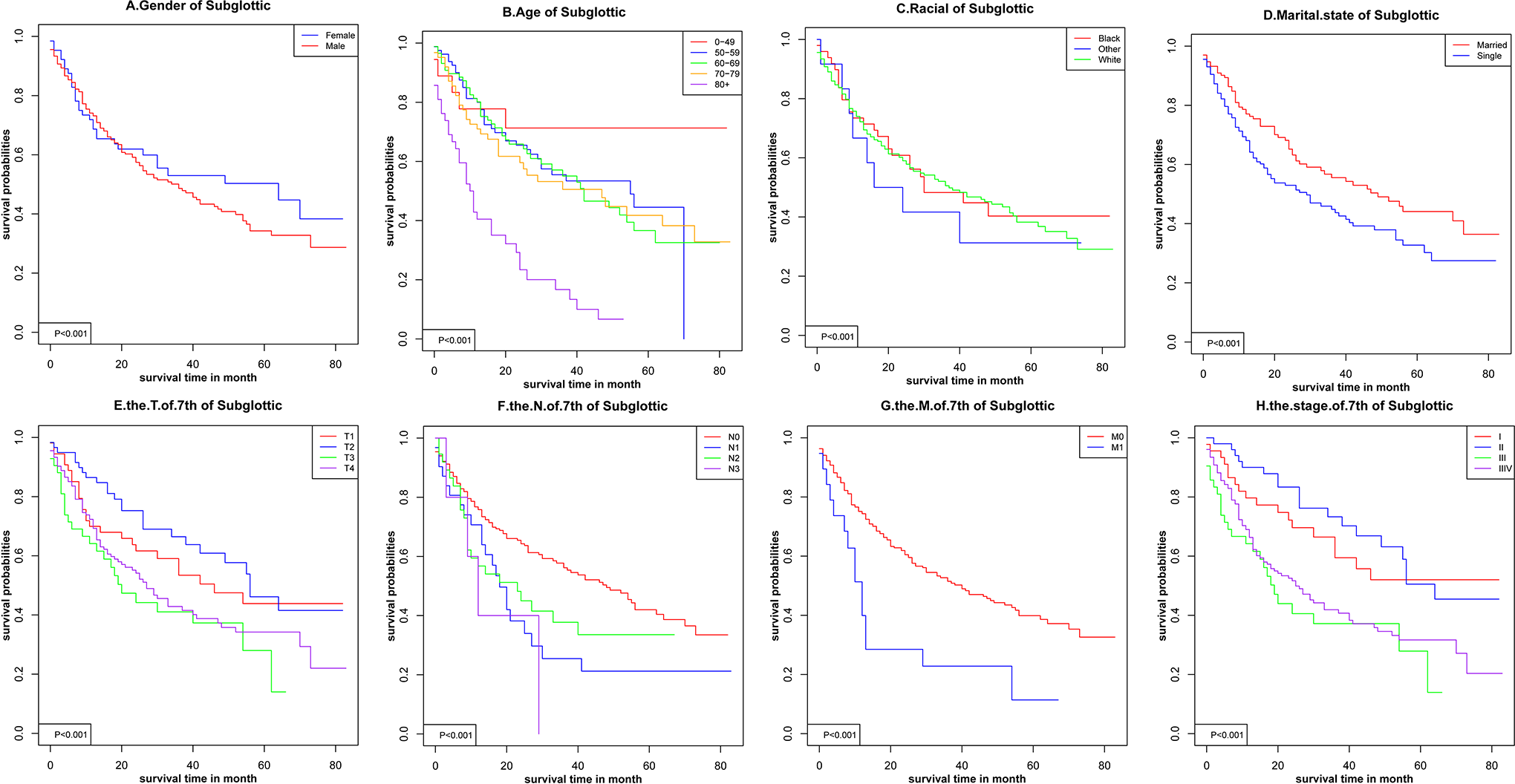
Kaplan-Meier survival curves for subglottic cancer.
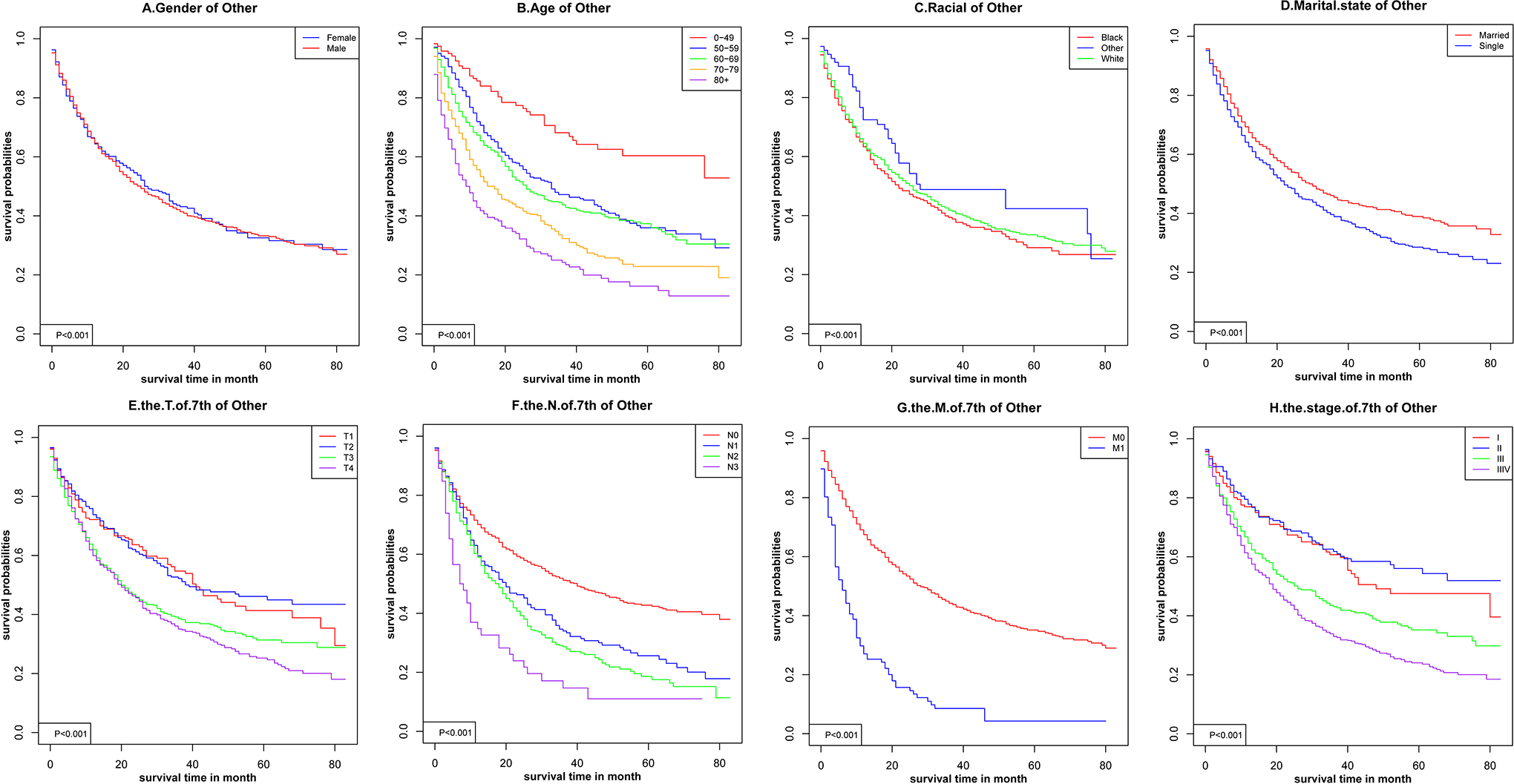
Kaplan-Meier survival curves for other cancer.
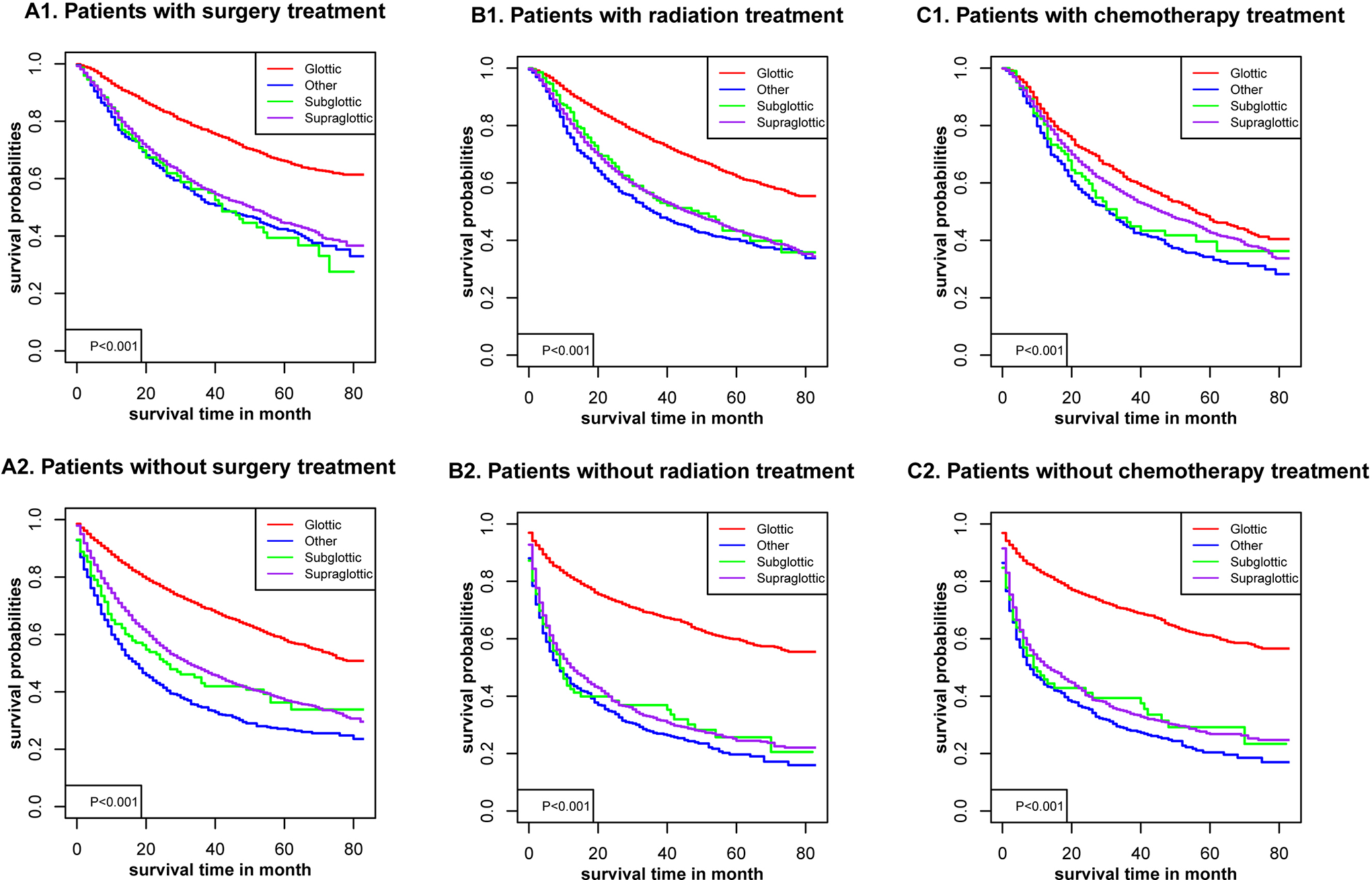
Kaplan-Meier survival curves with or without interventions for different sites of laryngocarcinoma.
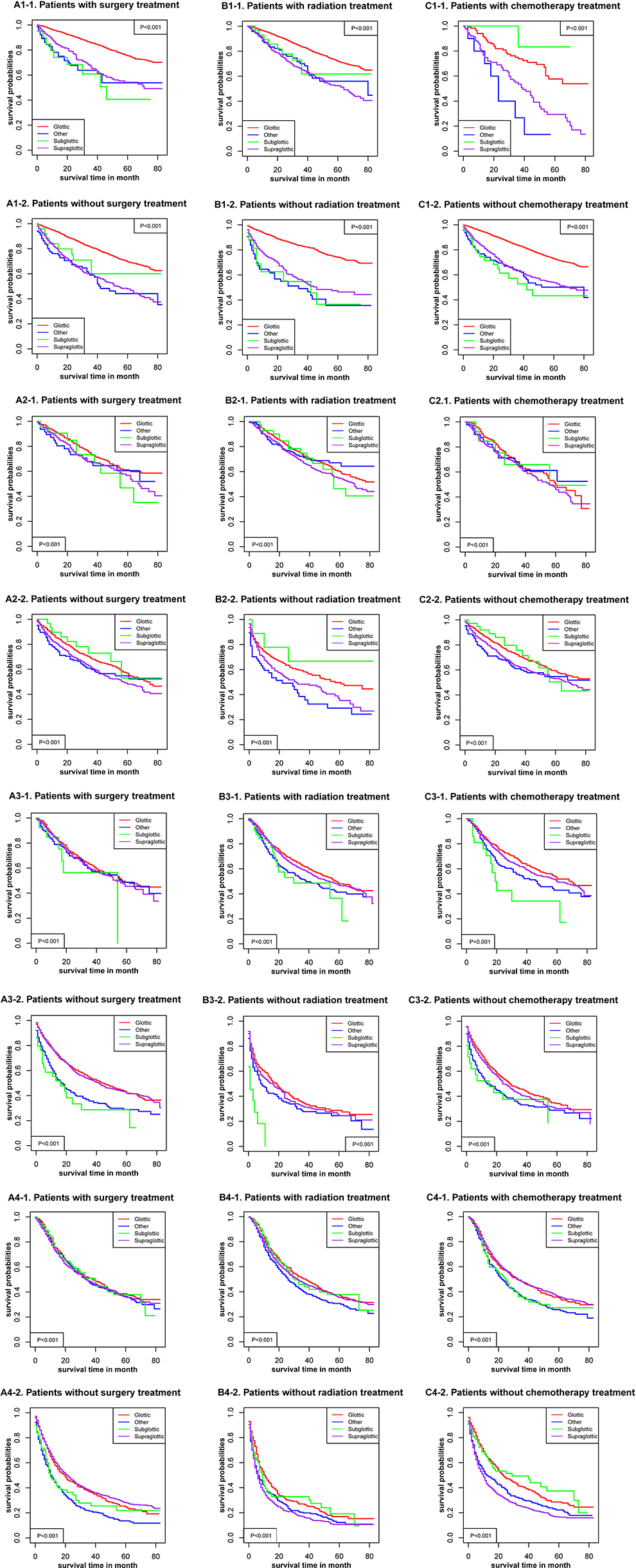
Kaplan-Meier survival curves with or without interventions for different sites of laryngocarcinoma with different American Joint Committee on Cancer (AJCC). 1—the stage at AJCC = I; 2—the stage at AJCC = II; 3—the stage at AJCC = III; and 4—the stage at AJCC = IV.
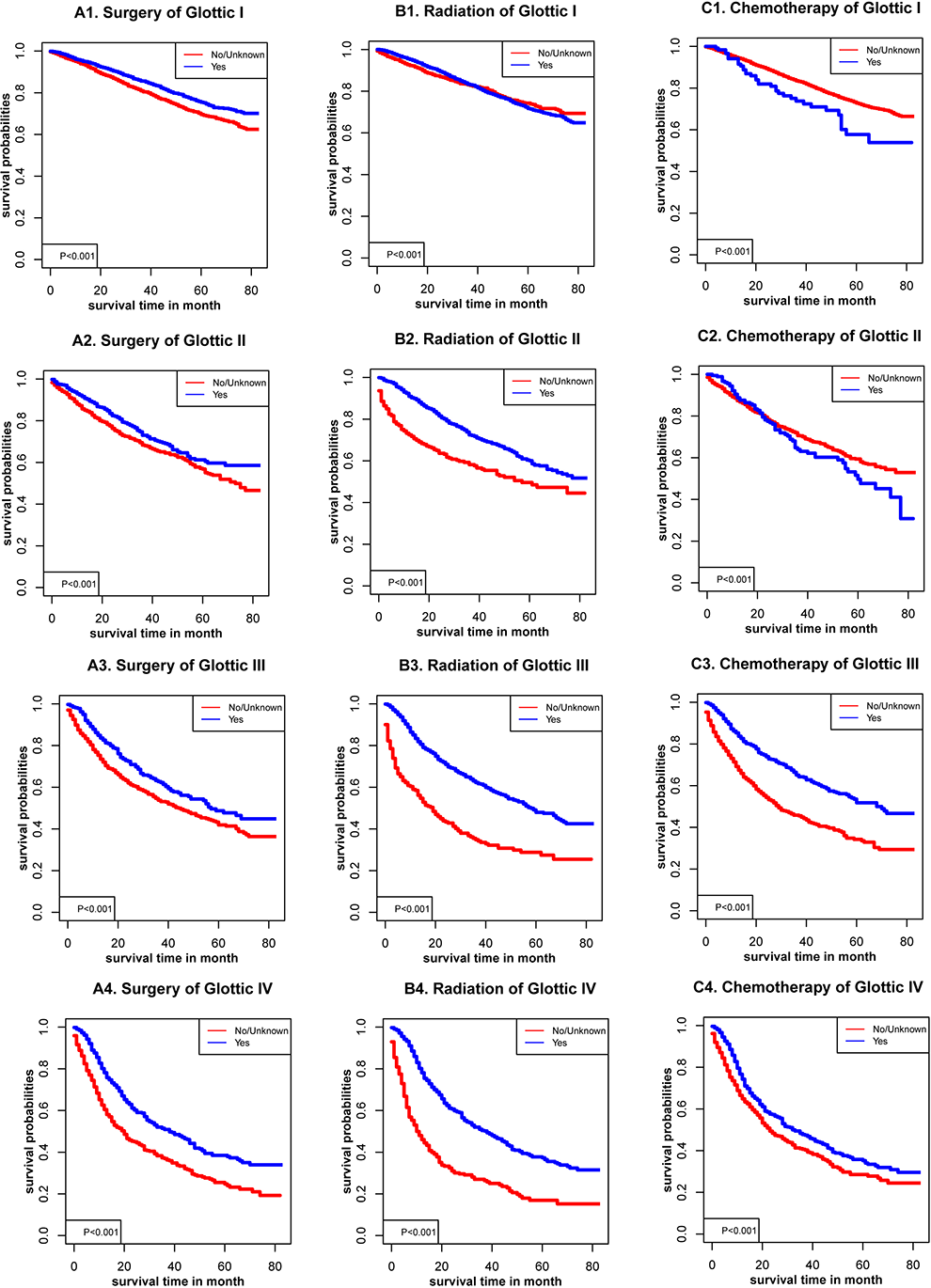
Kaplan-Meier survival curves with or without interventions for glottic cancer with different American Joint Committee on Cancer (AJCC).
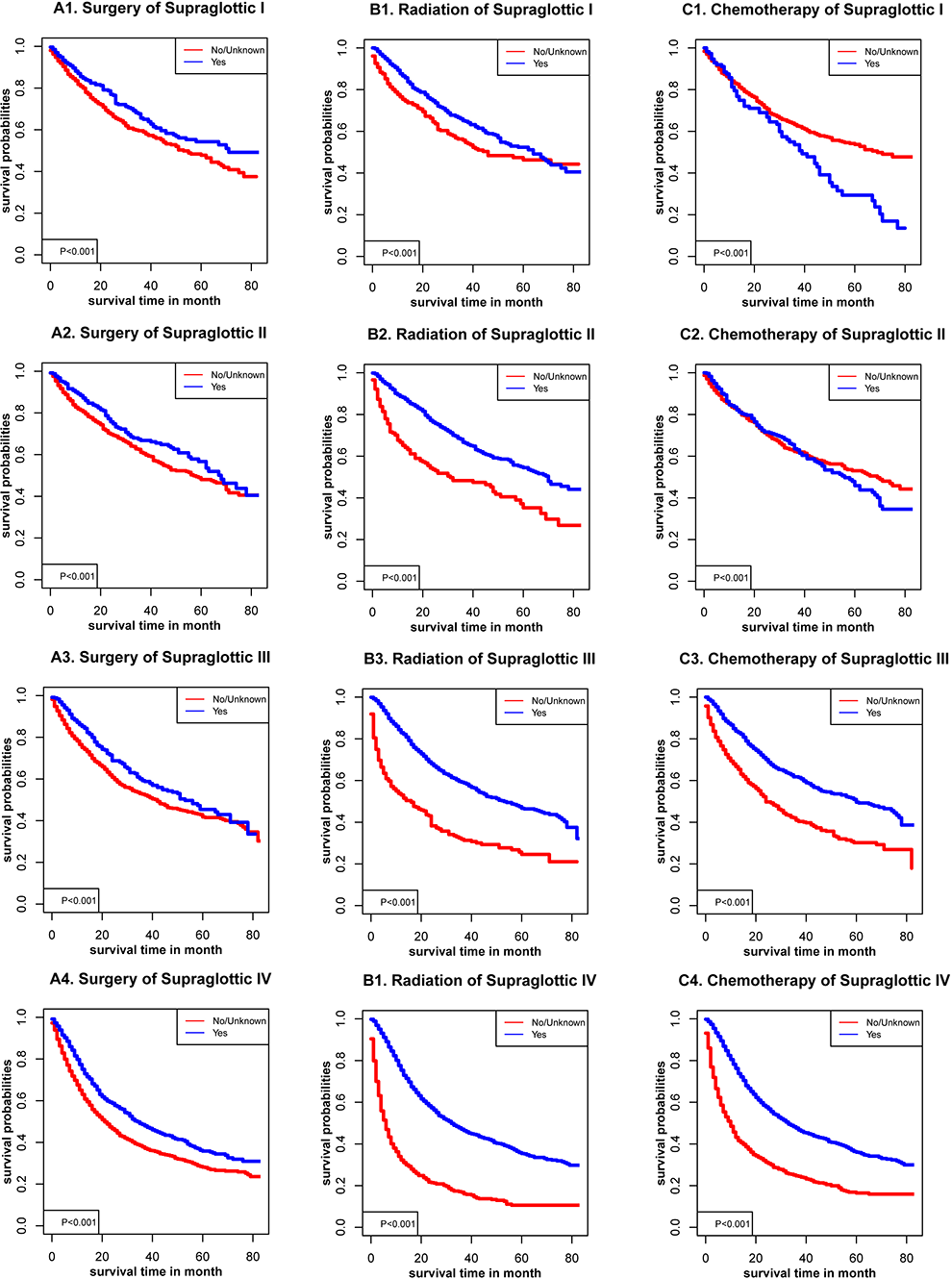
Kaplan-Meier survival curves with or without interventions for supraglottic cancer with different American Joint Committee on Cancer (AJCC).
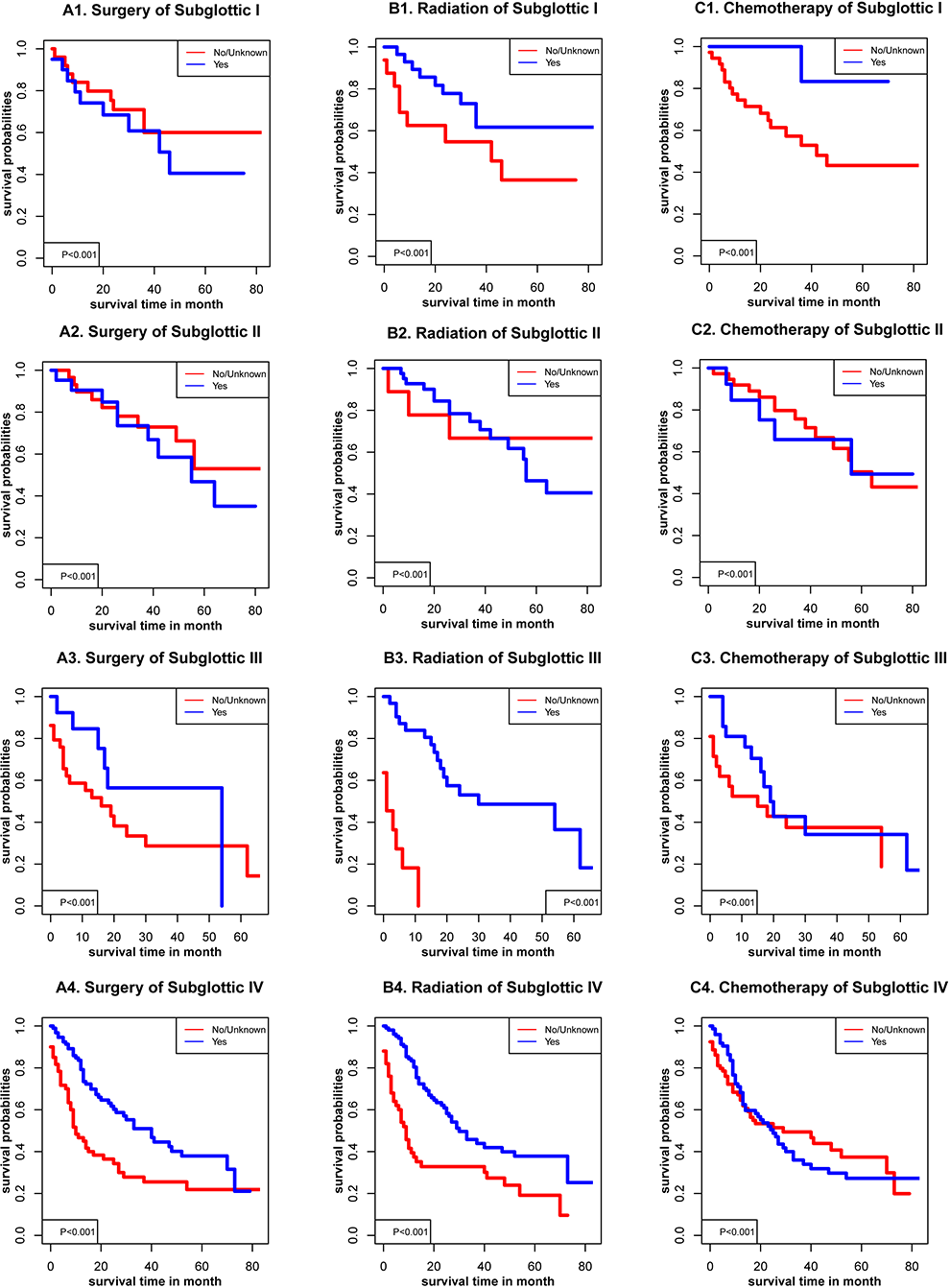
Kaplan-Meier survival curves with or without interventions for subglottic cancer with different American Joint Committee on Cancer (AJCC).
Kaplan-Meier survival curves with or without interventions for other cancer with different American Joint Committee on Cancer (AJCC).
Nomogram
In the construction of the nomogram, 11 independent factors were selected and modeled for prognosis in the present study, and univariate and multivariate Cox proportional risk models were used to calculate and detect the relationship between survival and each partner, as well as to derive prognostic maps for 3- and 5-year OS (Figure 11). Age, race, size, AJCC stage, TNM stage, surgery, radiotherapy, chemotherapy, and grade were the independent variables of interest for prediction (Figure 12). Figure 12 shows the C-index values of the glottic (0.732), supraglottic (0.700), subglottic (0.757), and other sites (0.735), suggesting that the nomogram is an accurate model for predicting OS. Overall, the nomogram was the dominant force to predict patient survival and has a strong reference value in clinical practice.
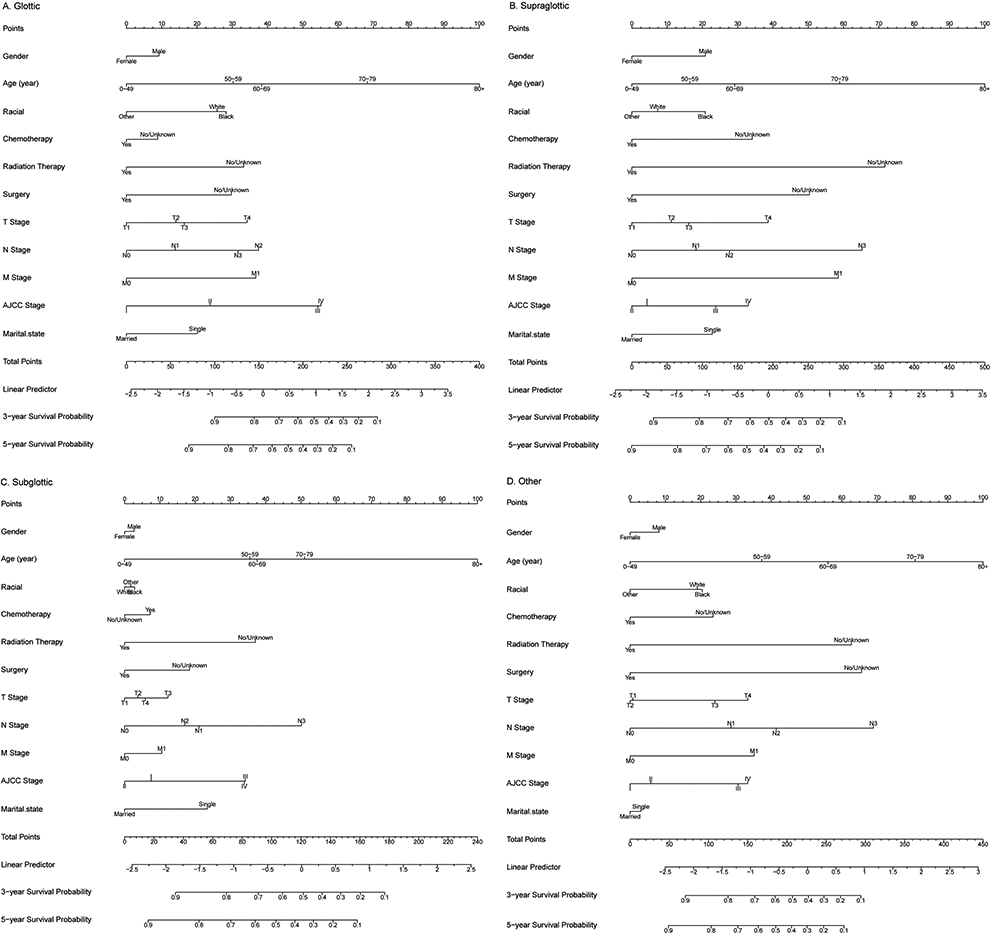
Nomogram of prediction for 3-year and 5-year overall survival of laryngocarcinoma.
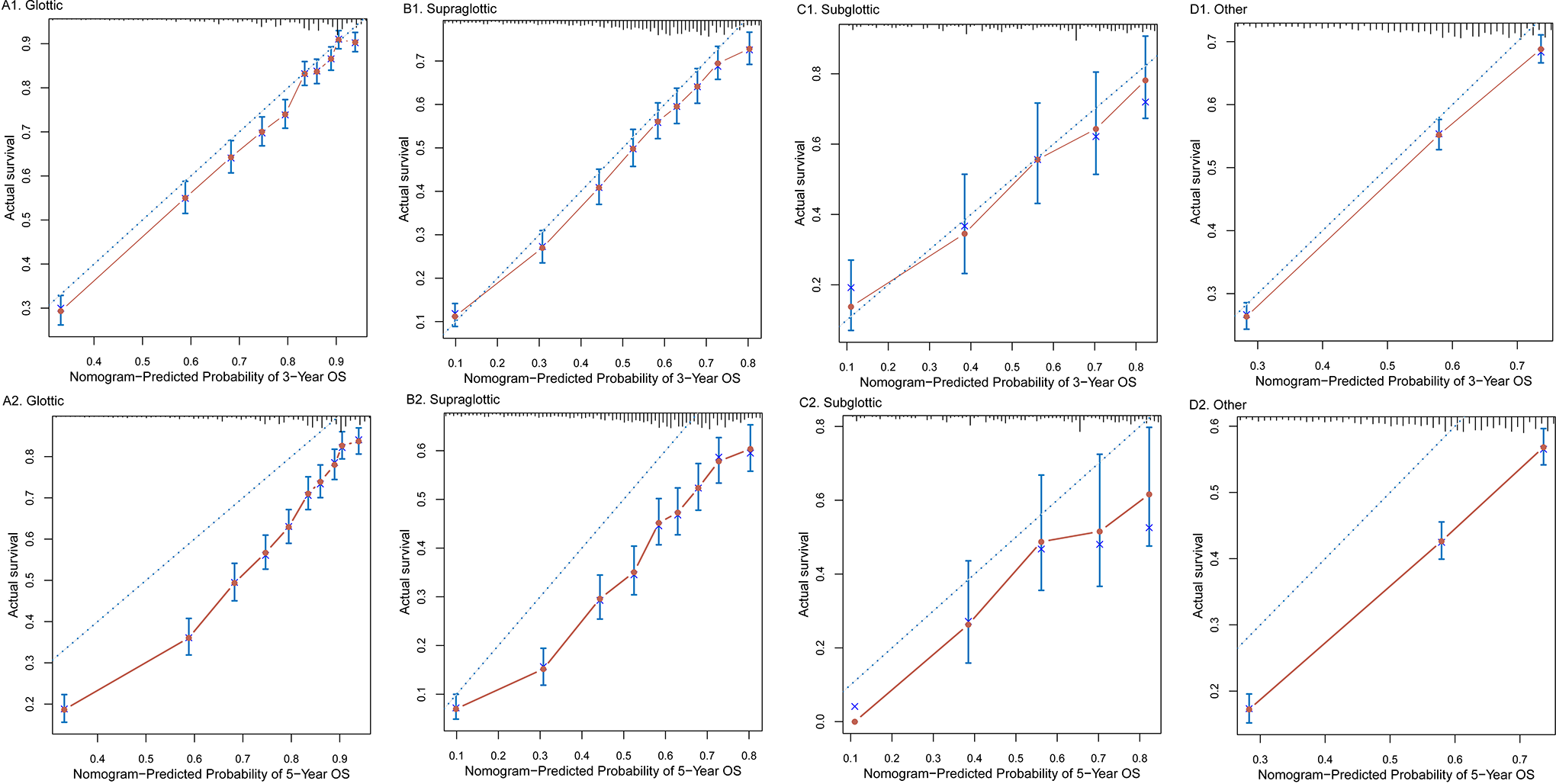
Calibration curves of the nomogram-predicted 3- and 5-year overall survival of laryngocarcinoma.
Discussion
In recent years, the incidence of LC has been increasing annually, with more males than females affected. Laryngocarcinoma is a heterogeneous disease. 6 The prognosis and choice of treatment are closely related to the anatomical site of the tumor, stage, and the patient’s desire to protect their larynx. 7 It is important to screen patients to determine who is eligible for larynx-preserving therapy. Studies have shown that LC is closely related to environmental pollution, smoking, drinking, and so on. 8 Clinically, most patients with LC have a long history of smoking. 8,9 In most patients with early LC at the time of diagnosis, the symptoms are not obvious, mostly involving throat pain, hoarseness, foreign body sensation, and so on. Early detection and active treatment can improve the survival rate after surgery. 10
At present, laryngectomy is recommended in cases of local LC, especially advanced T1-3 LC. The RTOG91-11 trial 11 included patients with mild cartilage erosion or tongue base involvement. Patients with T4 disease and cartilage penetration were not included in the present study. Therefore, we found no class I evidence to support nonsurgical organ preservation in these patients, and laryngectomy was generally chosen to treat patients with stage T4 LC, although some were unable or unwilling to undergo this procedure and opted for larynx-preserving therapy combined with radiotherapy and chemotherapy. Grover et al 12 analyzed the data of 6267 pathologically confirmed patients with stage T4 LC from 2003 to 2006 using the National Cancer Database of the United States. After matching the conditions, 969 patients were included in that study, including 353 who underwent total laryngectomy plus postoperative radiotherapy or chemoradiotherapy and 616 who underwent laryngectomy and chemoradiotherapy. The results showed that the median survival time of the operation group was 61 months, while that of the larynx-preserving radiotherapy and chemotherapy groups were 39 months. Therefore, patients with T4a stage disease should be cautious when opting for nonsurgical radiotherapy or chemotherapy, especially those with large tumor load and extensive tumor range.
Another study analyzed LC data from the US National Cancer Database to evaluate OS in stage T4 patients undergoing surgery and organ preservation therapy. Patients diagnosed with T4M0 LC between 2004 and 2012 were divided into 3 groups: surgery and postoperative adjuvant radiotherapy, induction chemotherapy combined with radiotherapy, and concurrent chemoradiotherapy. Multivariate analysis and propensity score matching were used to explore the association between different treatment modalities, and recursive zoning analysis was carried out to determine whether the groups benefited from the specific modalities. In the analysis, 1559 patients received surgery and adjuvant postoperative radiotherapy (547 patients received concurrent radiotherapy and chemotherapy after surgery), 1597 received concurrent radiotherapy and chemotherapy, and 386 patients received induction chemotherapy and radiotherapy. The results showed that the median OS of the 3 groups was 60.5, 43.3, and 32.5 months, respectively. The OS of the surgery and postoperative adjuvant radiotherapy group was significantly better than that of the concurrent chemoradiotherapy group, but it did not differ significantly from the OS of induction chemotherapy combined with radiotherapy. This suggests that surgery and postoperative adjuvant radiotherapy are better choices to treat stage T4 LC. However, organ preservation with induction chemotherapy combined with radiotherapy may be a reasonable choice for some patients, so the results are worthy of further stratification. Although clinical studies of nonsurgical larynx preservation have shown encouraging results using induction chemotherapy plus concurrent chemoradiotherapy, there has also been an increase in treatment-related toxicity, and treatment-related deaths due to severe toxic reactions have also occurred. In addition, some patients with locally advanced laryngeal and hypopharyngeal cancers are in poor physical condition and may not be able to tolerate treatment. Therefore, the cisplatin plus fluorouracil regimen induction chemotherapy combined with radiotherapy, with or without molecular targeted therapy, has been used to reduce treatment-related toxicity and increase treatment benefits. 13 Radiotherapy has a unique advantage over surgery in that it preserves speech. Huang et al 14 conducted a meta-analysis of 14 studies and found that radiotherapy is a better choice than compared laryngeal laser surgery to treat T1a glottic LC because it preserves maximum vocalization time and does not decrease fundamental frequency. Arias et al 15 evaluated 91 patients with early LC after treatment using the quality of life and Voice Handicap Index scale. They found that the voice quality, emotional character, and social relations of patients in the radiotherapy group were better than those in the surgery group. From the above clinical studies, it can be seen that, after more than 30 years of research into larynx-preserving therapies, the main ways to protect the laryngeal organs of patients with advanced LC are nonsurgical comprehensive treatments, such as synchronous radiotherapy and chemotherapy, synchronous radiotherapy after induction chemotherapy, radiotherapy, and simultaneous radiotherapy after induction chemotherapy combined with epidermal growth factor receptor molecular targeted therapy. 16
Currently, the National Comprehensive Cancer Network guidelines recommend cisplatin-based concurrent chemoradiotherapy in patients with middle-advanced LC, such as induction chemotherapy plus concurrent chemoradiotherapy/radical radiotherapy to treat supraglottic tumors. 17 The European Society for Medical Oncology guidelines recommend chemoradiotherapy with radiotherapy or concurrent chemoradiotherapy after induction chemotherapy. 18 Laryngocarcinoma treatment includes surgical resection and radiotherapy. Clinically, surgical treatment is mainly used, and other adjuvant drugs or radiotherapy are selected according to the condition of the patient. Although tumors can be completely removed by surgical resection, diseased cells in the patient’s body cannot be removed. Moreover, surgical resection of the tumor is very complicated, resulting in a longer postoperative recovery time and a higher probability of postoperative complications that seriously affect the quality of life of patients. Studies have shown that patients with LC who underwent surgical resection alone are prone to recurrence 3 to 5 years after surgery, and the probability of secondary cancer is high. 8
Radiotherapy to treat patients with LC before surgical resection can reduce the difficulty of surgery and improve the success rate of surgery. 19 At present, patients are usually treated with radiation before surgery when they can physically handle it. Radiotherapy can be regarded as an adjuvant treatment before surgery; it can inhibit the growth, proliferation, and metastasis of malignant cells. Moreover, radiotherapy can reduce the volume of the tumor, provide a good operating environment for subsequent surgical treatment, and improve the success rate of surgery. 20
There were several disadvantages in this research that must be accounted for. The primary restriction was the absence of information regarding patients with LC. The data were solely sourced from the SEER database, and the small sample size may cast doubt on the generalizability of the results. In addition, the lack of information regarding the details of treatment made it harder for the team to assess certain dispositions and behaviors during therapy.
Conclusions
The study found that male sex, age older than 80 years, black race, single status, T4, N4, M1, and AJCC stage IV were associated with higher mortality rates in LC at different sites. Survival rates were higher in patients with glottic cancer, especially early-stage patients of LC, regardless of the treatment regimes. Aggressive interventions, especially surgery and radiotherapy, may improve survival in patients with LC at different sites and at different AJCC stages. The present study emphasized that a combination of surgery and radiotherapy is the best approach and that therapy options may affect prognosis.
Footnotes
Authors’ Note
The datasets generated and/or analyzed during the current study are available in the Surveillance, Epidemiology and End Results (SEER) database repository, ![]() . Z-.M.Z. and Z.Z. had full access to all of the data in the study and took responsibility for the integrity of the data and the accuracy of the data analysis. Z-.M.Z. and Z-.X.C. designed the study. Z-.M.Z. and Z.Z. developed and tested the data collection forms. Z-.M.Z., Z.Z., and Z-.X.C. acquired the data. Z-.M.Z. conducted the analysis and interpreted the data. Z.Z. and Z-.X.C. drafted the manuscript. All authors critically revised the manuscript. Z-.M.Z. had guarantor. If necessary, we will store the code on a public platform and provide links to it.
. Z-.M.Z. and Z.Z. had full access to all of the data in the study and took responsibility for the integrity of the data and the accuracy of the data analysis. Z-.M.Z. and Z-.X.C. designed the study. Z-.M.Z. and Z.Z. developed and tested the data collection forms. Z-.M.Z., Z.Z., and Z-.X.C. acquired the data. Z-.M.Z. conducted the analysis and interpreted the data. Z.Z. and Z-.X.C. drafted the manuscript. All authors critically revised the manuscript. Z-.M.Z. had guarantor. If necessary, we will store the code on a public platform and provide links to it.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.