
Abstract
Parathyroid carcinoma is a rare endocrine tumor. Parathyroid carcinoma in patients with secondary hyperparathyroidism due to chronic kidney disease is also rare. In addition, thyroid hemiagenesis is a rare congenital anomaly. We report an extremely rare case of parathyroid carcinoma in a patient with secondary hyperparathyroidism and thyroid hemiagenesis. We also present a review of the literature of this rare entity. We also discuss the surgical procedure performed for this patient. Our review of the literature found 34 case reports of parathyroid carcinoma in patients undergoing dialysis due to chronic renal failure; 14 reports of thyroid hemiagenesis with parathyroid disease; and no previous reports of thyroid hemiagenesis with secondary hyperparathyroidism and parathyroid carcinoma. Although surgical treatment of parathyroid carcinoma requires combined resection with the thyroid, peritracheal dissection with total parathyroidectomy, and monitoring intact parathyroid hormone as a tumor marker, our procedure preserved the patient’s thyroid function. There has been no evidence of recurrence for over 8 years.
Keywords
Introduction
Parathyroid carcinoma (PC) is a rare endocrine tumor of unknown cause. 1 Recent studies revealed some associations between the development of carcinoma and genetic mutations and end-stage renal disease. 1,2 However, PC in a patient with secondary hyperparathyroidism (SHPT) caused by chronic kidney disease is rare. 3,4 There have been very few cases reported. 5 -7
Thyroid hemiagenesis is a rare congenital anomaly that could be revealed a thorough examination for thyroid disease. 8 There have been several reports of thyroid hemiagenesis with conditions such as thyroid tumor, 9 Graves’ disease, 10 and primary hyperparathyroidism, 11 but there have been no reports of SHPT and PC. We report an extremely rare case of PC in a patient with SHPT and thyroid hemiagenesis as well as a review of the literature.
Case Report
History
A 48-year-old woman who had been on dialysis since age 33 years because of chronic glomerulonephritis complained of systemic joint pain. Calcification in the joints and elevated intact parathyroid hormone (iPTH) levels were detected. She was evaluated by the Department of Nephrology at Kyoto University Hospital and subsequently diagnosed with SHPT, and she was advised to have surgery. She was referred to the Department of Otolaryngology–Head and Neck Surgery at Kyoto University Hospital.
Laboratory and Imaging
Although there was no history of thyroid disease or treatment, computed tomography (CT) and ultrasonography did not confirm the right lobe of the thyroid or ectopic thyroid tissue, suggesting right thyroid hemiagenesis (Figure 1A and B). Swollen parathyroid glands on the right side were found in an anatomically normal position with thyroid hemiagenesis (Figure 1C and D).
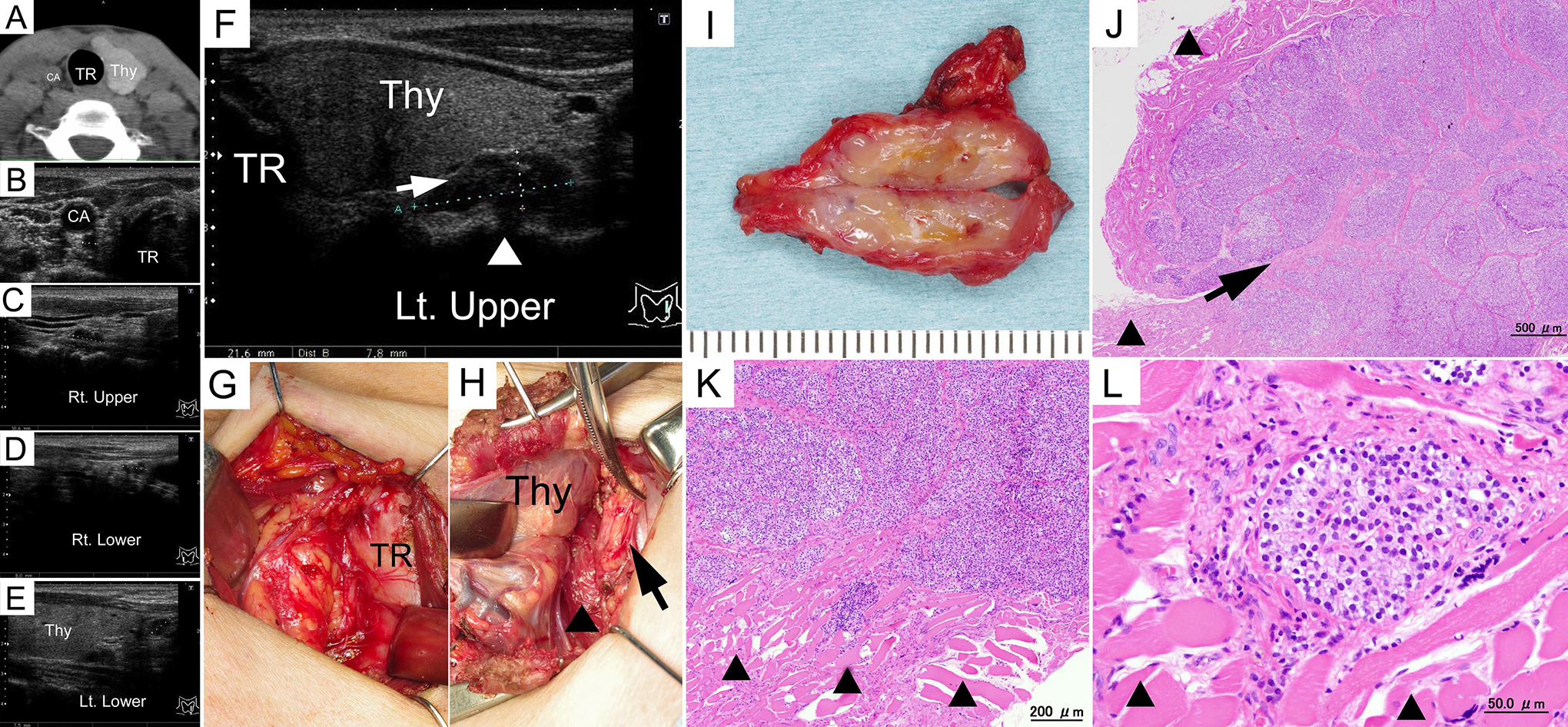
Computed tomography and ultrasonography revealed thyroid hemiagenesis of the right lobe (A and B). Ultrasonography showed swelling of all parathyroid glands (C-F) and a markedly swollen left upper parathyroid gland (F) with the esophageal muscularis posterior to the gland having an irregular edge (F, arrowhead) and fibrous bands (F, arrow). Intraoperative photographs demonstrate that the right lobe of thyroid was absent (G). The left upper parathyroid tumor was resected (H, arrow). The esophageal muscularis was partially resected (H, arrowhead). Macroscopic image of the left upper parathyroid gland (I) and permanent section of the left upper parathyroid specimen (J-L). The left upper parathyroid tumor was approximately 2 × 1 cm. The tumor infiltrated the surrounding muscle and was fibrous and sclerotic in the cross section (I). Permanent sections of the left upper parathyroid specimen demonstrate tumor invasion into surrounding muscular structure (J-L, arrowhead) with fibrous bands (J, arrow). CA indicates carotid artery; Lt., left; Rt., right; Thy, thyroid; TR, trachea.
Ultrasonography of the thyroid showed swelling of all parathyroid glands; a markedly swollen left upper parathyroid gland up to approximately 20 mm; and an irregular edge to the esophageal muscularis posterior to the gland (Figure 1F). However, the swollen left upper parathyroid gland was not palpable. Other parathyroid glands were less than 10 mm (Figure 1C-E).
Laboratory data (and reference ranges) were as follows: iPTH 830 pg/mL (10-65); calcium (Ca) 8.9 mg/dL (8.7-10.1); thyroid stimulating hormone 2.250 μIU/mL (0.5-5.0); and free T4 0.961 ng/dL (0.88-1.62).
Surgery
For en bloc parathyroidectomy, bilateral peritracheal lymph node dissections were performed because the border between the left upper parathyroid gland and the esophagus was unclear and there was a risk of carcinoma. Intraoperatively, the left upper parathyroid gland was found to be infiltrating the esophageal muscularis, suggesting carcinoma. We resected the muscularis together with the left upper parathyroid gland, but no esophageal mucosal defect occurred (Figure 1H). However, we preserved the left lobe of the thyroid because the right lobe was absent and no adhesions between the PC and the left lobe of the thyroid were observed. The recurrent laryngeal nerves on both sides were preserved. On the right side, the superior and inferior thyroid arteries were absent (Figure 1G). The other 3 parathyroid glands were found in the peritracheal dissection tissue. Autotransplantation of the parathyroid gland was not performed.
Histopathology
The postoperative pathological examination revealed hyperplasia of parathyroid tissue in all glands. Parathyroid cell infiltration into the surrounding muscle layer of the esophagus only occurred in the left upper parathyroid gland, which was diagnosed as PC (Figure 1I-L). The surgical margin of the PC in the left upper parathyroid gland was negative. No lymph node metastasis was observed.
Postoperative Course
The postoperative course was uneventful. No hoarseness occurred. The patient was discharged on postoperative day 8. Postoperative iPTH levels were undetectable.
In this case, additional resection of the remaining left lobe of the thyroid would have caused lifelong hypothyroidism because of thyroid hemiagenesis. The surgical margins of the resected PC were negative, so we decided not to perform additional thyroidectomy. Since there was a risk of local recurrence near the left lobe of the thyroid, we measured iPTH as a tumor marker regularly to detect recurrence at an early stage.
Due to the transfer of the surgeon, the patient received follow-up examinations at the Department of Otolaryngology–Head and Neck Surgery in the National Hospital Organization Kyoto Medical Center. In the 8 years since the operation, no increase in serum iPTH levels has been observed. There was no evidence of recurrence based on CT, magnetic resonance imaging, or ultrasonography of the thyroid.
Discussion
Parathyroid carcinoma is an extremely rare, malignant endocrine tumor. It reportedly accounts for 0.005% of all malignancies. 1 The incidence of PC among patients with primary hyperparathyroidism is 0.74% to 6.1%. 12,13 The pathological condition in which a tumor secreting parathyroid hormone occurs during the course of SHPT is called tertiary hyperparathyroidism. 14 In this patient, tertiary hyperparathyroidism was suspected because of parathyroid hyperplasia in all parathyroid glands, one of which had increased in size and became malignant. In addition, there were signs such as joint calcification.
Secondary hyperparathyroidism is a common complication in patients with chronic kidney disease. However, surgery for SHPT rarely reveals PC. There have been a few reports of PC in patients undergoing dialysis due to chronic renal failure in the past. The first case was reported by Berland et al. in 1982. 15 Bossola et al reported 20 cases in the literature in 2005. 5 In the English-language literature, there have been 34 reports to our knowledge (Table 1). 16 -27 Typically, each of the 4 parathyroid glands shows different pathological findings. 1 6 Bilateral PC has been reported. 1 9 In addition, PC has occurred in ectopic parathyroid glands of the mediastinum. 20,2 5 Parathyroid carcinoma arising from autotransplanted parathyroid tissue has also been reported. 26
Parathyroid Carcinoma in Patients Undergoing Dialysis Due to Chronic Renal Failure.
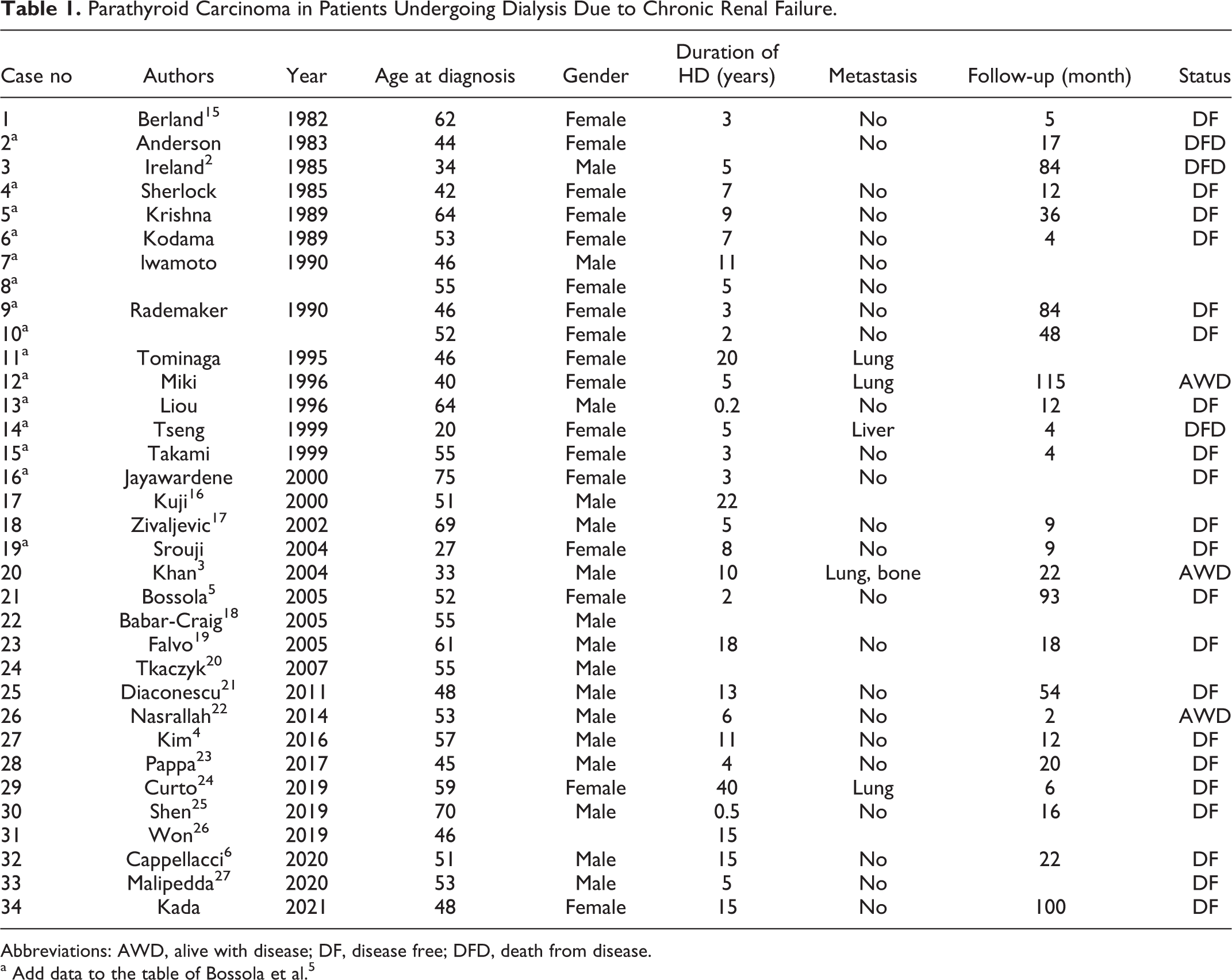
Abbreviations: AWD, alive with disease; DF, disease free; DFD, death from disease.
a Add data to the table of Bossola et al. 5
The ratio of men to women among patients with PC is roughly 1:1. 1 The average age is approximately 50 years, which was similar to previous reports. 1,6,13 The average duration of dialysis performed before the discovery of PC is 9 years, which was longer than previously reported. 6 Considering the possibility that hyperparathyroidism stimulation in long-term dialysis induces carcinoma, 1 it is important to consider the possibility of encountering PC in the context of SHPT, as in primary hyperparathyroidism.
To diagnosis PC, a high serum Ca level, high iPTH level, and palpable tumor are findings suggestive of PC. 1 However, in the case of SHPT, it is difficult to judge based on serum Ca levels because of dialysis. 5 Since the hyperplastic lesions of the 4 glands have a tendency to produce high iPTH levels, it is difficult to suspect carcinoma based on laboratory data. In this case, it is probable that the tumor was not large and that it was difficult to palpate due to the compensatory development of the left thyroid because of thyroid hemiagenesis on the right. However, because ultrasonography revealed that the left upper parathyroid gland had infiltrated surrounding tissues and was larger than the other 3 glands, it was possible for us to approach this as a malignancy during the surgery. We reaffirmed the importance of diagnostic imaging before surgery for SHPT.
The standard treatment for resectable PC is surgery. 1 Complete en bloc resection of the tumor offers the best chance for cure. The standard surgical treatment is thyroid lobectomy and peritracheal dissection. 28 However, in this patient, the right lobe of the thyroid was absent, and combined resection of the remaining left lobe would inevitably result in lifelong hypothyroidism. As the surgical margins of the resected specimen were negative for carcinoma, we decided to preserve the left lobe of the thyroid.
We did not perform autologous parathyroid transplant for 2 reasons. First, autotransplantation may cause a relapse of hyperparathyroidism in the future in young patients. 29 Second, total removal of the parathyroid gland makes it possible to use iPTH as a marker for residual disease or recurrence. 16,29
Since there is a risk of recurrence near the left lobe of the thyroid, iPTH was measured as a tumor marker every 3 months for early detection. In this patient, the parathyroid was completely resected and iPTH levels did not increase. No evidence of recurrence was found during follow-up with iPTH monitoring or diagnostic imaging for over 8 years. On the basis of thyroid function preservation and no evidence of recurrence, our surgical treatment for this patient was considered appropriate.
Thyroid hemiagenesis is an extremely rare developmental disorder of the thyroid, 10 but it may become apparent during surveillance for thyroid diseases such as thyroid tumor, carcinoma, or Graves’ disease. 9 -11 Thyroid hemiagenesis is caused by one side of the thyroid not developing embryologically, rather than a failure of glandular tissue descent or migration, as seen in ectopic thyroid. 7,30 Regarding laterality, past reports have shown many cases of thyroid hemiagenesis are on the left side. Defects on the right side, as in this case, are rare. 10 The incidence of thyroid hemiagenesis is estimated to be approximately 0.02%. 30 It tends to be more common in women. 31 Since women are more likely to be affected by thyroid diseases in general and have more opportunities to undergo thyroid examination, women might be more likely to be found to have thyroid hemiagenesis. 7 Further research is required to determine why there is a gender difference in the incidence of thyroid hemiagenesis.
Parathyroid adenomas have been found in anatomically normal positions in patients with thyroid hemiagenesis. 32 In our patient with right thyroid hemiagenesis, swollen parathyroid glands on the ipsilateral side were found in an anatomically normal position. Thyroid function was reported to be normal in most patients with thyroid hemiagenesis. 11
Few reports have described an association between parathyroid disease and thyroid hemiagenesis. Alqahtani et al previously reported 13 cases of thyroid hemiagenesis in association with primary hyperparathyroidism in the English language literature. 11 This case is 14th case of thyroid hemiagenesis in association with hyperparathyroidism. Previous patients had primary hyperparathyroidism. No cases of SHPT and PC were have been previously reported, and this is the first case of thyroid hemiagenesis with SHPT and PC.
Conclusion
We encountered an extremely rare case of SHPT with PC and thyroid hemiagenesis. The patient was cured with peritracheal dissection and total parathyroidectomy. Thyroid function was preserved, and there has been no evidence of recurrence for over 8 years.
Footnotes
Authors’ Note
S.K. was the surgeon and wrote this paper. M.T. was an attending surgeon for this patient under the supervision of S.K. A.Y. helped S.K. draft the manuscript. All authors discussed the results and implications, commented on the manuscript at all stages, and approved the final manuscript. Records and data pertaining to this case are in the patient’s secure medical records at the Kyoto University Hospital and the National Hospital Organization Kyoto Medical Center. Written informed consent was obtained from the patient, to conduct the study and publish data and images associated with this case report.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.