
Abstract
Apocrine hidrocystoma is a cystic tumor originating from apocrine sweat glands. It is predominantly located in the eyelid margins. Here, we report a case of apocrine hidrocystoma of the parotid gland in a 19-year-old man who was referred to our outpatient clinic with a 5-year history of a gradual swelling in the left parotid region. The patient underwent left superficial parotidectomy. Histological examination confirmed the diagnosis of apocrine hidrocystoma. The case is original by the tumor’s location: to the best of our knowledge, this could be the first case in English and French literature reporting an apocrine hidrocystoma affecting the parotid gland. The purpose of this article is to report our case and discuss its clinical and anatomopathological features as well as its differential diagnoses.
Introduction
Hidrocystomas are cystic lesions that arise from sweat glands and they are classically categorized as apocrine or eccrine based on their histological features. 1 Apocrine hidrocystoma (AH) is described as an adenomatous cystic proliferation of the secretory coil of apocrine sweat glands. 2 These latter are mostly found in the axilla and perianal area, but AH generally occurs in the head and neck region. The typical localization is the periorbital area; however, other uncommon sites have been reported: oral mucosa, lips, ears, and trunk. 1 -3
In this article, we report a new case of AH but in an unusual anatomic site. To the best of our knowledge, this could be the first case in English and French literature reporting an AH affecting the parotid gland. The purpose of this article is to discuss through our case the clinical and anatomopathological features of AH of the parotid gland as well as its differential diagnoses.
Case Report
A 19-year-old man with no medical history was referred to our outpatient clinic with a 5-year history of gradual swelling in the left parotid region. There were no other complaints. Physical examination showed a soft, nontender, and well-limited mass located in left parotid region. It was not fixed to the underlying structures. The overlying skin was normal. The swelling measured 5 × 3 cm. There were no signs of facial nerve palsy and no palpable cervical lymph nodes.
Preoperative magnetic resonance imaging showed a cystic lesion located in the superficial and the deep lobes of the left parotid gland. The lesion was hyperintense on T1- and T2-weighted sequences (Figure 1). These features were consistent with a diagnosis of a parotid hemorrhagic cyst.
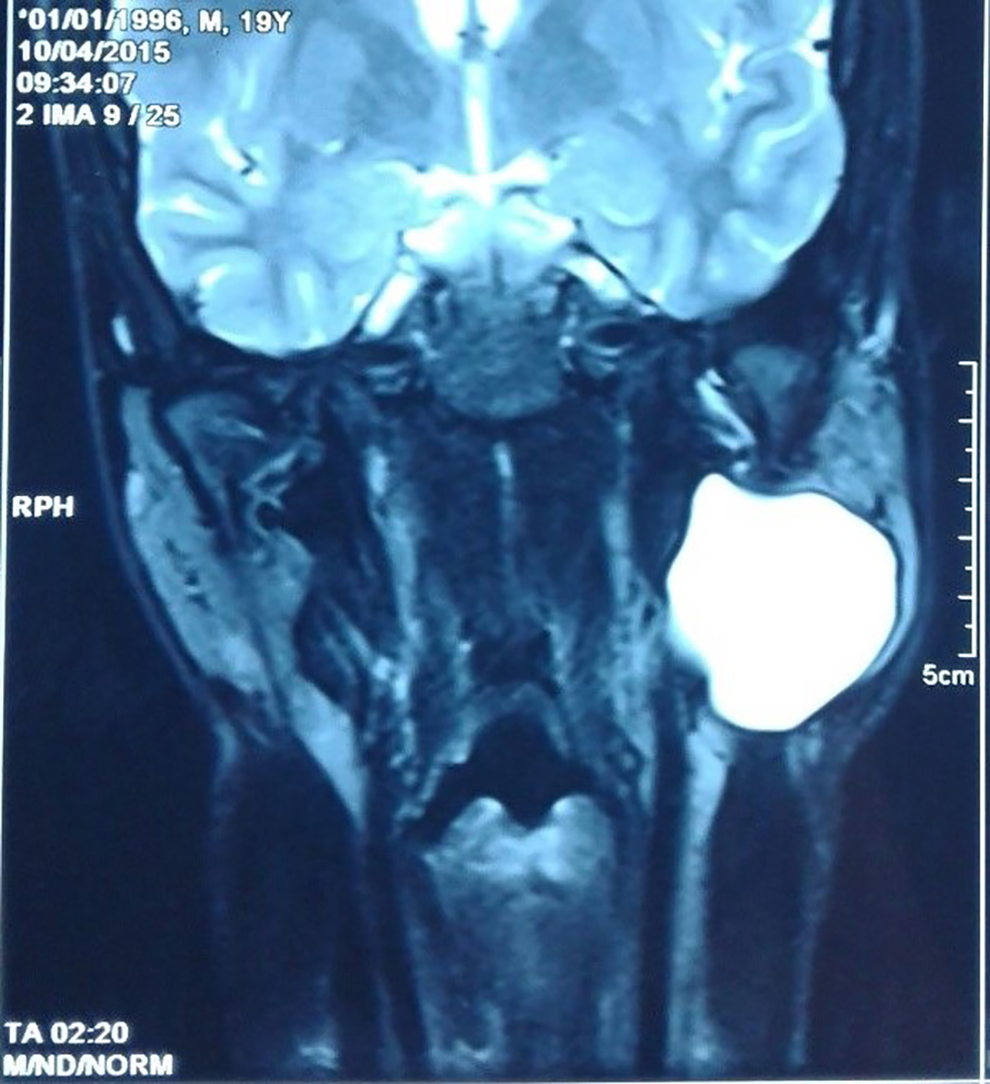
Coronal magnetic resonance imaging (MRI; T2-weighted sequence): cystic lesion located in the superficial and the deep lobes of the left parotid gland. The lesion was hyperintense and well-limited.
The patient underwent left parotidectomy: a cystic mass located in the superficial and the deep lobes of the left parotid gland. The cyst was accidentally ruptured (containing clear fluid).
Intraoperative examination suggested a benign cyst. No complications, especially no facial nerve palsy, were noted after the surgery.
Grossly, the surgical piece measured 6.5 × 2 × 1 cm; the cut surface revealed a cyst emptied of its contents which measured 3 × 2.5 × 2 cm. The histological examination showed the presence of serous acini. At high magnification, the cystic cavity is lined with a double-layered epithelium: an outer layer of flattened myoepithelial cells and an inner layer of tall columnar cells. These latter showed decapitation secretion, indicating the presence of apocrine secretion (Figure 2). The epithelium presented some foci of squamous metaplasia as well as ulcerations. No histological signs of malignancy were found. A final diagnosis of AH was established.
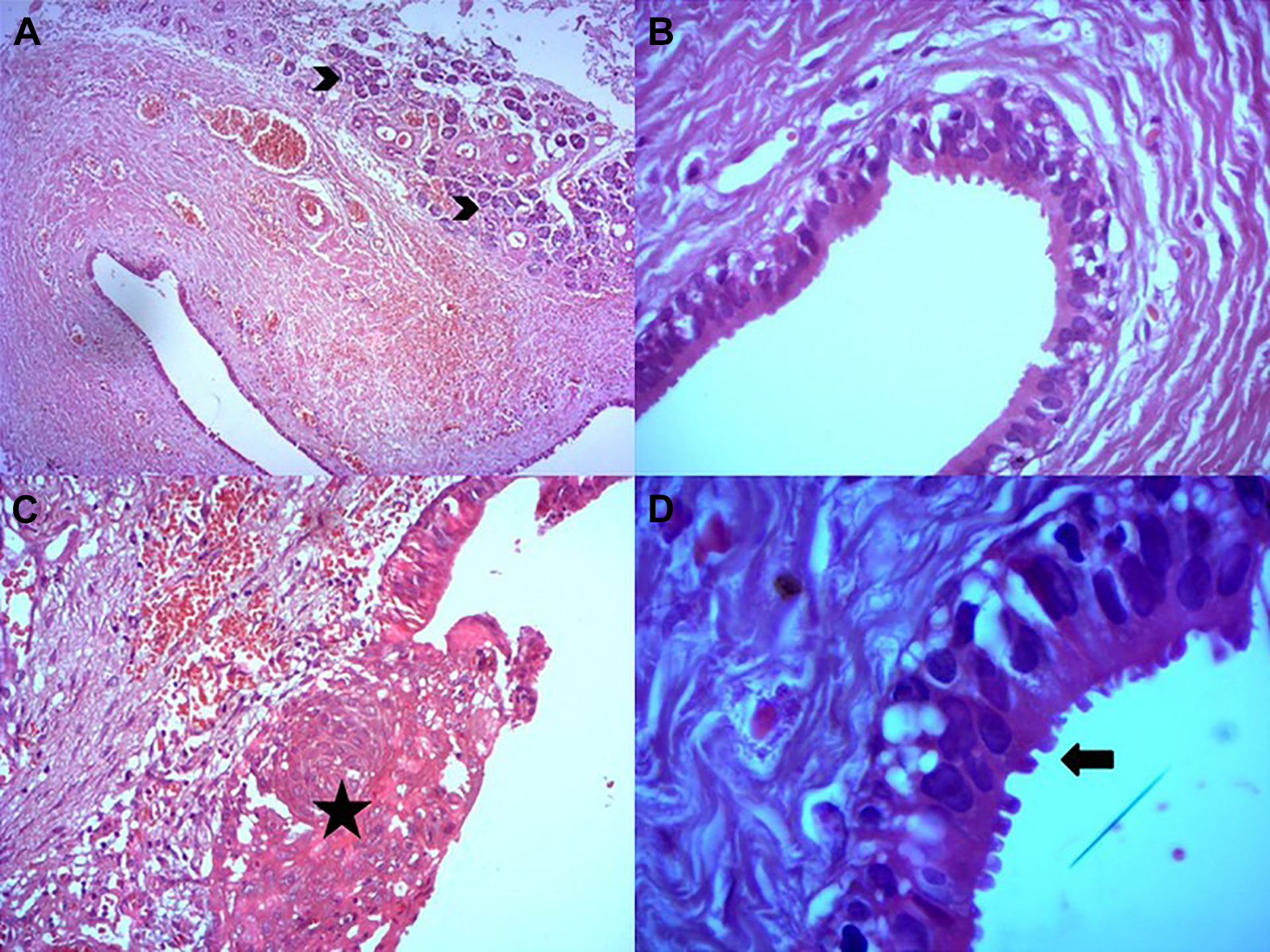
(A) Histological section of the cystic wall at low magnification: the presence of serous acini (arrowhead; hematoxylin-eosin ×4); (B) at high magnification, the fibrous wall is lined by an outer layer of flattened myoepithelial cells and an inner layer of tall columnar cells (hematoxylin-eosin ×40); (C) focal squamous metaplasia (asterisk; hematoxylin-eosin ×40); (D) decapitation secretion (arrow; hematoxylin-eosin ×100 oil).
After 4 years of follow-up, he exhibited no evidence of recurrence.
Discussion
Apocrine hidrocystoma is a rare benign cystic tumor originating from the secretory portion of apocrine sweat glands. 2 So, it will be normally seen on the skin. It predominantly occurs in the eyelid margins. Other uncommon locations have been reported: oral mucosa, lips, ears, trunk, and intraorbital. 1 -3 Anavi et al 4 reported a case of a large AH deep in the preauricular region, contiguous to the parotid gland but it was located above the superficial temporal fascia, adherent to the dermis. To the authors’ knowledge, the parotid localization has not been reported, making this presentation, the first published case. What makes our case very unusual, is the extracutaneous site of the tumor. To explain the development of AH inside the parotid gland, we can consider the following hypotheses:
– The presence of ectopic sweat glands in the parotid gland.
– Metaplastic change of the salivary gland epithelium into an apocrine-like secretory epithelium.
Apocrine hidrocystoma is prevalent in adults between 30 and 75 years of age with equal sex incidence and rarely occurs during childhood. 2,3,5
The etiology and the pathogenesis of AH are not entirely known. 5 Apocrine hidrocystoma is considered to be a cystic proliferation of the secretary part of apocrine sweat glands rather than a simple retention cyst. 5 Apocrine hidrocystoma is generally a small solitary lesion. 1,3 Multiple lesions are rare.
Microscopically, AH has a double lining epithelium. The inner layer is made of tall columnar or cuboidal cells with eosinophilic cytoplasm and decapitation secretion, which is the pathognomonic histological sign. The outer layer consisting of myoepithelial cells. 2,3 Frequently, there is intracystic papillary proliferation. 4,5 Immunohistochemically, AH is positive for human milk fat globules, GCDFP-15, CK7, and CK18 in the inner layer of epithelium, and for alpha-smooth muscle actin (α-SMA) in the outer myoepithelial cells. 3
The other type of hidrocystoma is eccrine hidrocystoma (EH) is a retention cyst of the eccrine duct. 3 Apocrine hidrocystoma can be differentiated from EH by the presence of secretory cells showing decapitation secretion. 3 Besides, EH is lined by flat epithelium without myoepithelial cells or papillary projections into the lumen, and it is negative for human milk fat globules, GCDFP-15, CK7, CK18, and α-SMA. 3,4 Apocrine hidrocystoma expresses a secretory-type keratin pattern, whereas EH expresses an excretory-type keratin pattern. 3
The differential diagnosis with neoplastic or non-neoplastic cystic lesions of the parotid gland can pose a problem in this site: Sclerosing polycystic adenosis, salivary duct cyst (retention cyst), lymphoepithelial cyst (branchial cleft cyst), HIV-associated salivary gland disease (lymphoepithelial sialadenitis), dermoid cyst, lymphangioma, Warthin tumor, cystadenoma, pleomorphic adenoma, basal cell adenoma, acinic cell carcinoma (papillary cystic variant), mucoepidermoid carcinoma, cystadenocarcinoma, carcinoma ex pleomorphic adenoma, and epithelial–myoepithelial carcinoma. 3 The apocrine-like secretory epithelium is the principal feature to differentiate AH from these differential diagnoses. 3 The most important differentiating parotid gland lesion is sclerosing polycystic adenosis because apocrine-like epithelium (GCDFP-15 positive) is commonly observed, but the presence of nodular sclerosis, xanthomatous infiltrate, acinar-type cells, and foamy degeneration of cyst-lining epithelial cells, is in favor of sclerosing polycystic adenosis. 3
In other locations, several treatment options have been documented: simple needle puncture, hypertonic glucose sclerotherapy, trichloroacetic acid or botulinum toxin injection, electrodesiccation, radiofrequency ablation, carbon dioxide laser treatment, and cryotherapy. 5 However, the most common treatment is surgical excision whatever the site of AH. 5 Recurrence is rare after surgical removal. 5 No malignant transformation of AH has been reported. 5
Conclusion
Apocrine hidrocystoma is commonly located around the eyes. The parotid gland is a very unusual site of AH. This entity can mimic other cystic lesions that more often present at this site. Histological examination is an important tool to obtain a final diagnosis and differentiation from other possibilities. Decapitation secretion is a hallmark of AH. This condition is usually treated by surgical excision with a low rate of recurrence.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.