
Abstract
Objectives:
The aim of this research is to understand the importance of female career mentors, research mentors, co-residents, and program directors/chairs to current female otolaryngology residents when applying to residency. The importance of safety in the workplace was also investigated.
Methods:
Surveys were sent via electronic mail to 119 programs, and program directors were asked to distribute them to female residents. Using the Likert scale, participants ranked the importance of various factors when creating a rank list, in particular, importance of safety in the workplace and importance of female mentors in various leadership positions. Demographic information, geographic location, LGBTQ identification, and fellowship plans were also collected.
Results:
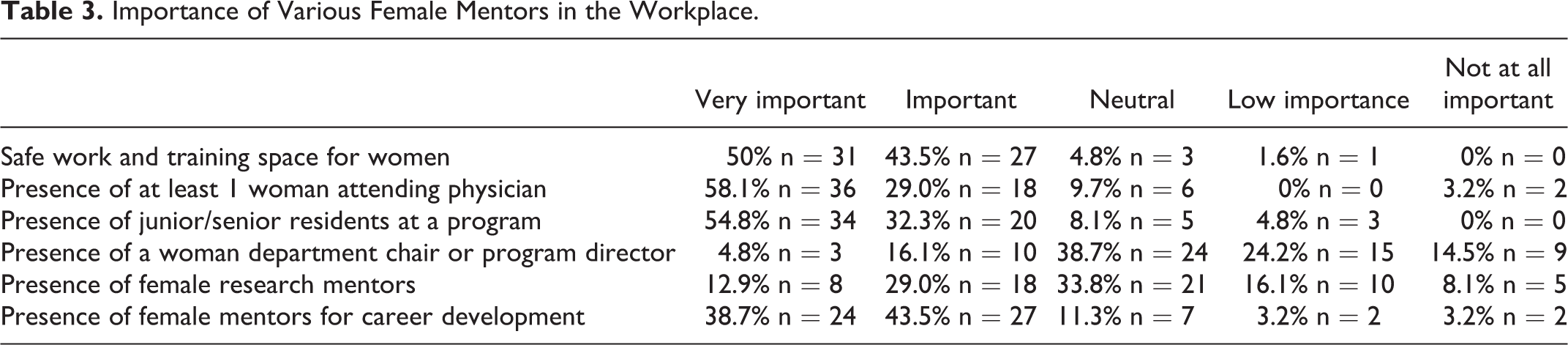
There were 62 participants nationally. Eighty-seven percent (n = 54) of participants stated that having at least 1 female attending and having female co-residents was “very important” or “important” when ranking programs. A number of respondents replied that having a female career development mentor (38.7% [n = 24] and 43.5% [n = 27]), female program director or chair (4.8% [n = 3] and 16.1% [n = 10]), and female research mentor (12.9% [n = 8] and 29% [n = 18]) was “very important” or “important,” respectively. Ninety-three percent (n = 58) replied that feeling safe in their training environment was “very important” or “important.”
Conclusion:
Having female mentors as well as safety in the workplace in residency is important to a vast majority of residents and applicants when creating a rank list. Programs with women in these roles may gain a disproportionate number of female residents because they may be more desirable places than those without women in these roles.
Introduction
Multiple factors are important when medical students rank programs for residency. Geographic location, reputation of program, interview day experience, and overall compatibility are noted to be important. 1 Female medical students may consider the presence or absence of female physician mentors in a specialty as a contributing factor to overall “fit” of a program. This is increasingly relevant as the American Academy of Medical Colleges announced that in 2019, for the first time in history, there was a 50.5% majority of female medical students nationally. 2
Several studies have evaluated factors for female applicants across specialties. Rohde et al 3 examined the presence of females in orthopedic surgery and found that 68% of female applicants eliminated residency programs from their rank list based on perceived sex biases. 3, 4 In ophthalmology female applicants, authors found the presence of gender and ethnic diversity was rated as more important to female applicants compared to their male counterparts. 5 Of physical medicine and rehabilitation applicants, females were more likely to consider “favorable environments for women and minorities” as important compared to male applicants. 6 Finally, Fairmont et al 7 found that otolaryngology applicants ranked the presence of female residents and faculty as 4.1 and 4.2 of 5, respectively, as important when considering a program; additionally, they noted that a small number of applicants cancelled interviews for lack of female residents (7.6%) and faculty (5.5%).
Similar to other surgical subspecialties, otolaryngology remains a male-dominated field. In past couple decades, however, the presence of females in clinical practice and in research is growing. In 1998, 6% of otolaryngologists were female; 8 in 2017, this grew to 14.5%. 9 In otolaryngology research, females as first and/or last author increased from 28% to 39% in 2000 to 2015. 10
Moreover, it is increasingly relevant to engage female applicants and residents to best address their needs and safety in training. Safety, specifically as an absence of verbal and physical harassment, has also been an increasing theme; Lawlor et al 11 showed that 31% of female otolaryngologists experienced “subtle undertones” of harassment, 8% experienced “noticeable tones” of harassment, and 2% experienced “significant harassment.”
The primary aim of this research was to understand the importance of safety in the workplace as well as the importance of female career mentors, research mentors, co-residents, and program directors/chairs to current otolaryngology residents when they were applying to otolaryngology residency. Secondary questions, such as plans for fellowship, plans for academic career, and the role of residency program geographic and demographic characteristics impacted participants’ rank lists decisions, were also investigated.
Methods
A survey was sent via electronic mail to 119 otolaryngology resident training programs. Medical school graduation years ranged from 2014 to 2020. Program directors were asked to distribute the survey to female residents. The survey collected demographic information such as graduation year, age, identification as a member of the LGBTQ community, geographic region of medical school, geographic region of residency, career aspirations (academic vs independent practice), and consideration of fellowship. The geographic regions were based on US Census regions and included New England, Middle Atlantic, East North Central/Midwest, West North Central/Midwest, South Atlantic, East South Central, West South Central, Mountain, and Pacific. Inclusion criteria included any current female residents enrolled in a US otolaryngology residency training program. Exclusion criteria included males and those who did not matched into a US residency program in otolaryngology. An institutional review board approved this study. Information about the study was provided upon distribution of the survey, and informed consent from participants was implied by participation in the survey. The following factors were surveyed in regard to importance when creating one’s rank list: safe workplace/training environment for females specifically as an absence of verbal and physical harassment, presence of at least 1 female attending physician, presence of junior and/or senior female residents in the program, presence of a female department chair or residency program director, presence of female research mentors, and presence of female mentors for career development. A Likert scale was used with options of very important, important, neutral, low importance, or not at all important. Statistical analysis was performed including means, proportions, correlation, and analysis of variance.
Results
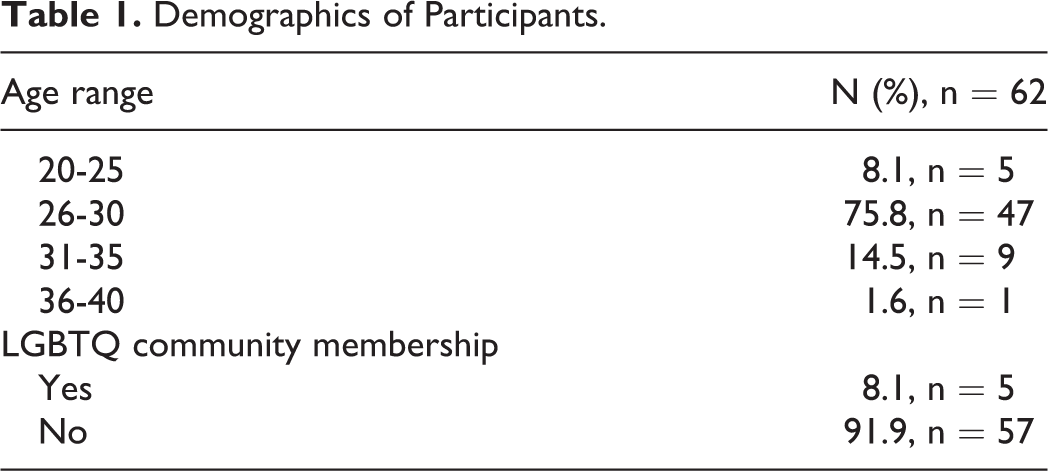
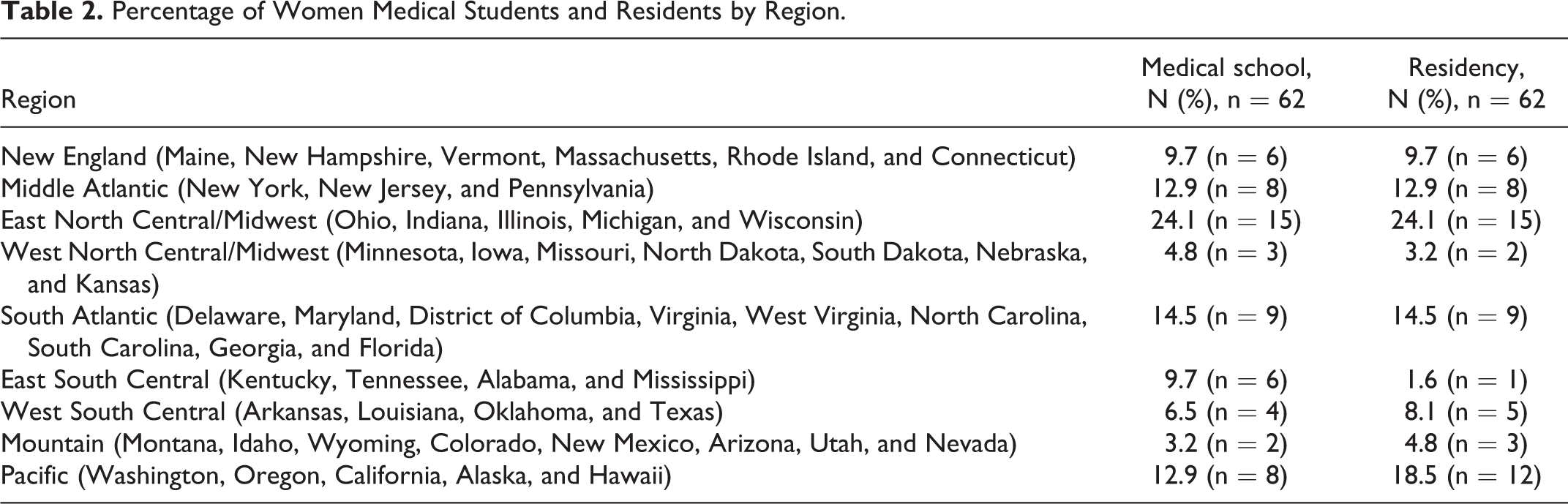
Survey responses were returned by 62 participants, which is about 12% of total female otolaryngology residents in the United States as determined from published program information. A majority of respondents were 26 to 30 years old (75.8% [n = 47]) and a minority identified as members of the LGBTQ community (8.1% [n = 5]; Table 1). Many respondents attended medical school or residency in the East North Central/Midwest (both 24.1% [n = 15]), followed by the Pacific (12.9% [n = 8] and 17.7% [n = 11]), South Atlantic (both 14.5% [n = 9]), Middle Atlantic (both 12.9% [n = 8]), New England (both 9.7% [n = 6]), West South Central (6.5% [n = 4] and 8.1% [n = 5]), East South Central (9.7% [n = 6] and 1.6% [n = 1]), West North Central/Midwest (4.8% [n = 3] and 3.2% [n = 2]), and Mountain (3.2% [n = 2] and 4.8% [n = 3]; Table 2). Of note, 40.3% (n = 25) of applicants attended residency in the same region as their medical school. Of the participants, 43.5% (n = 27) were planning a career in academic medicine, 16.1% (n = 10) were not, and 40.3% (n = 25) were unsure. Sixty-six percent (n = 41) of participants wanted to pursue fellowship and 19.4% (n = 12) were unsure. Further correlations noted were perceived importance of female research mentors and applicant desire for academic career and fellowship (r = 0.07, r = 0.14), importance of female career mentors, and desire for academic career and fellowship, respectively (r = 0.05, r = 0.04). There was no significant difference when stratifying these by postgraduate year.
Demographics of Participants.
Percentage of Women Medical Students and Residents by Region.
Almost 94% (n = 58) of respondents felt that safe work and training space for women was at least important with 50% rating this as very important (Table 3). Additionally, 58% (n = 36) of respondents felt that having at least 1 female attending on staff was very important to their rankings. Further, the presence of junior and/or senior residents and female mentors for career development was rated as very important (Table 3). Less important was the presence of a female chair or program director or the presence of female research mentors. There were no significant differences between those participants who identified as LGBTQ or not on importance of female mentors across all categories.
Importance of Various Female Mentors in the Workplace.
Discussion
The presence of female career mentors, co-residents, and attendings as well as safety in the workplace was considered “very important” or “important” for the majority of female residents when they were creating their final residency rank list. Programs should be aware of these preferences in order to provide a better atmosphere and to meet the needs of female residents. Because female mentors are important to incoming female residents, female applicants are likely to flock to places with female co-residents, mentorship, and leadership, creating a “nesting” effect. This could lead to certain programs having a disproportionate number of female residents. However, applicants may not be thinking ahead during the application process about the presence or absence of female mentors because of the overwhelming theme to “match anywhere.” Noting how important having female co-residents is, as well as female faculty and mentorship in a residency, programs with no or few female staff or residents should consider creating a network to support female residents.
The growing role of diversity and inclusion in otolaryngology has been a prominent topic in the past several years. In just under 20 years, the percentage of women in otolaryngology has more than doubled. 8,9 Of graduating otolaryngology residents, there is an almost equal percentage of women pursuing academics and fellowships as men (35% women and 39% men and 54%, women vs 59% men). 12 The current study found that 66% (n = 41) of participants wanted to pursue fellowships and 43.5% (n = 27) wanted to purse academics; interestingly, 19.4% (n = 12) and 40.3% (n = 25) of participants were still unsure of what they wanted to do for fellowship and overall career, respectively.
As such a large percentage of women wanted to pursue academics or fellowship, it is important to note the disparities that still exist. There is still a difference when examining research funding even after controlling for rank and experience in academics. 13 Although funding is mostly pattered around degree (PhDs receiving the most regardless of gender) and subspecialty of the research, there is overall female underrepresentation. 14 When examining National Institutes of Health research funding, Lennon et al 14 found that while 31% of otolaryngology grant recipients were female, this proportion was not the case after stratifying for degree. Specifically, 18% were female MDs, 39% were female PhDs, and 21% were MD/PhDs. The importance of career and research mentorship for these female residents is essential. It is known that women are disproportionately represented in academic leadership positions such as chair positions and program directorships. 15 Career development and research mentorship are not limited from female to female; however, given how important these positions were to respondents, it should be something noted.
Optimizing the work environment to provide female applicants and residents with a safe and fruitful training environment will be important as the number of females in otolaryngology continues to increase. Despite the growing number of females in otolaryngology, there is still an imbalance between males and females in the field. There could be a number of factors to explain this, but a large component could be lack of other female mentors. When female medical students are rotating through otolaryngology, if they are the only females on the service, it can be more difficult to “fit in” or feel part of the team, and they may not consider otolaryngology as a specialty. Noting the presence of other females may increase feelings of inclusivity and to the ability to picture oneself in the field. Additionally, it is essential to recognize that despite an increasing presence in medicine, females still are the target of workplace and sexual harassment. Notably, it was surprising that “safety in the workplace,” specifically as an absence of verbal and physical harassment, was rated as “very important” by only half the participants when ranking a program. This number increased to an overwhelming majority when including “important” with that analysis. Whether the harassment is blatant or subtle, eliminating it is of the utmost importance in order to provide a safe and comfortable place to learn and work.
As for the secondary questions of this project, 40.3% of applicants matched in the same geographic region as their medical school. When constructing a comprehensive list of factors that influence female applicants, this is certainly a factor to consider as it was marked important by 88% of applicants. 1 Therefore, if programs are interested in matching more female residents, they should focus on those from their regions. A limitation of this study is the low response rate likely due to the volume of email received by residents, lack of reward filling out a survey, as well as the reliance of program directors for distribution of the questionnaire. Another limitation is that there were no data collected about how important these factors are when compared to each other. Are geographic locations, fellowship opportunities, or other factors more important than having women mentors to applicants? Future research should examine if women mentors had any influence on the participants’ desires or lack thereof to go into fellowships or academia. Additionally, it is interesting that having a female chair or program director was less important to applicants. Future studies may want to examine this as well, and whether or not this changes as residents transition into attendings.
Conclusion
It is important to consider the different factors that affect rank lists of female applicants for otolaryngology programs given the growing number of females in the field. This information will hopefully be beneficial to residency programs when highlighting what they can offer to applicants. Additionally, this information may also be useful to applicants when researching what others have considered when creating rank lists. Ultimately, the goal of this project is to emphasize that having female role models and mentors as well as safety in the workplace in residency is important to residents and applicants when creating a rank list.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.