
Abstract
Introduction
The number of women entering medical school has steadily increased since 2003. In 2021, 55.5% of medical school matriculants and 46.4% of resident physicians in the United States were women. 1 Despite this, few women reach top leadership positions in academic medicine. In 2019, women made up 41% of academic physicians in the United States but only accounted for 18% of medical school deans and department chairs. 2 Furthermore, a lack of women in leadership positions is more prevalent in general surgery and most surgical specialties.
In Otolaryngology-Head and Neck Surgery (OHNS), women represented 36% of residents as of 2019. 2 Although women also represented about 36% of full-time academic OHNS faculty at this time, multiple studies have demonstrated a decline in the proportion of women leaders as academic rank increases.3 -5 In 2020, women Otolaryngologists held 26% of residency program directorships, 14.7% of fellowship directorships, and less than 5% of department chair positions. 4 The only specialty with a lower representation of women in department chair positions in Orthopedic Surgery, with only 1 female department chair (0.8%) as of 2019. 2
Although improvements have been made in the number of women medical students and OHNS residents, the lower numbers of women OHNS faculty in leadership positions may indicate that the promotion of women in OHNS is lagging. Factors such as higher burnout rates, mistreatment of women surgeons, and lack of women mentors are frequently cited as reasons for suboptimal retainment and promotion in most surgical specialties.6 -8
The importance of women mentors has been well demonstrated in academic medicine.8,9 Women medical students are more likely to specialize in OHNS when their medical school has full-time OHNS women faculty. These students are also more likely to choose a residency program with a higher proportion of women residents across all specialties. 9 Another recent study demonstrated a significant correlation between plastic surgery faculty gender and plastic surgery resident gender. 10 Early career women faculty frequently cite a lack of female role models as a barrier to promotion and voice the importance of same-sex mentorship more frequently than their male counterparts.7,8 Despite this, to our knowledge, no study has comprehensively investigated trends in gender diversity and the correlation between leadership gender diversity and resident and faculty representation in OHNS. This study aims to examine the gender composition of residents and faculty in academic OHNS residency programs in the United States over the past decade and to investigate any association between female representation in leadership positions and gender diversity among faculty and residents.
Methods
Study Design and Data Collection
Exemption status was obtained from the Institutional Review Board at Vanderbilt University Medical Center. A comprehensive literature review of the PubMed, SCOPUS, and EMBASE online databases was performed in May of 2023 using variations of the terms “Otolaryngology-Head and Neck Surgery,” “Female Surgeon,” and “Internship and Residency” (Supplemental Appendix 1). There was no limitation on the initial years queried. Each search was run separately, and all references were uploaded to Endnote reference software, where duplicates were removed. Title and abstract screening were completed by a single reviewer (N.D.). All articles investigating the gender diversity of residents and faculty in OHNS residency programs within the past 10 years were included for final review. Full-text review and data extraction were performed by the same reviewer. Article inclusion was finalized by the senior author (S.Y.). Data on total numbers and percent representation of women OHNS department chairs and residency program directors, OHNS faculty, and OHNS residents was collected from each of the selected articles. These numbers were analyzed to determine trends among the number of women within different ranks in OHNS residency programs.
A cross-sectional study of the gender composition of residents and faculty in OHNS residency programs in the United States was performed in August 2022. Residency programs were identified using the Electronic Residency Application Service (ERAS) 2023 Participating Specialties and Programs website. The following data was collected for each residency program: gender of associated medical school dean, gender of OHNS department chair and residency program director, and total number and gender of fellowship directors, OHNS faculty, and OHNS residents. Data was collected from program websites, as the Accreditation Council for Graduate Medical Education (ACGME) and the Association of American Medical Colleges (AAMC) do not publicly release individual program data. The gender of each resident and faculty member was recorded based on pronouns used and provided photographs on each departmental website. The gender of the department chair and program director for each program were recorded in the same manner. If program websites were incomplete, social media accounts and other public listings for each program were explored. Program coordinators were also contacted to complete the data set if needed.
Data on total number and gender of OHNS fellows was not collected, as fellowship programs are typically limited to 1 to 2 years, not all fellows are part of programs accredited by the ACGME, and fellows are not consistently listed on department websites. In addition, fellowship director’s gender was only collected for OHNS fellowships associated with a residency program. When OHNS was not a department but a division of Surgery, the gender of the chair of the department of Surgery was included.
The following relationships were investigated: correlation between chair gender and program director gender, fellowship director gender, faculty gender, and resident gender; correlation between program director gender and resident gender; correlation between faculty gender and resident gender; correlation between medical school dean gender and department chair gender, faculty gender, and resident gender.
Statistical Analysis
Trends in gender diversity at the department chair, residency program director, faculty, and resident level were analyzed using the quick analysis and chart functions in Microsoft Excel. Analysis of the cross-sectional portion of this study involved stratification of program characteristics (percent women residents, percent women faculty, etc) by program chair gender. A Wilcoxon rank sum test was used to determine differences in categorical variables and a Fisher’s exact test for continuous variables within this stratification. Similar analysis was conducted after stratification between gender of medical school deans as well as gender of program directors. Pearson’s correlation was used to analyze the relationship between percent women faculty members and the percentage of women residents. All analysis was performed using R (R. Studio, Boston, MA) version 4.1.2.
Results
Three hundred thirteen unique references were identified. Of these, 20 studies included a description of gender composition of residents and faculty in OHNS residency programs with the earliest publication being from 1979. There was an overall trend of an increasing number of women within all ranks of OHNS. The total number of women chairs published in current literature increased from 3 in 2013 to 10 in 2022 (Figure 1).4,11-16 Similarly, over this timeframe, the percentage of women residency program directors reported increased from 16% to 30% (Figure 2).4,11-16 An increase in the reported number of women residents was seen with 19% of OHNS residents being women in 2001 compared to 42% in 2022 (Figure 3).12-16 A single article published in 1979 indicated that less than 1% of OHNS faculty were women. 17 This published number increased to 25% in 2019 and 27% in 2022.12,14,18
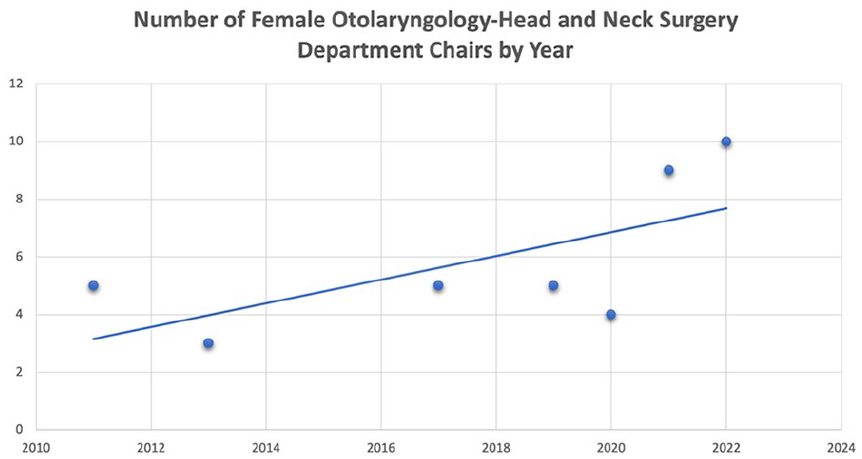
Published number of female Otolaryngology-Head and Neck Surgery department chairs by year.
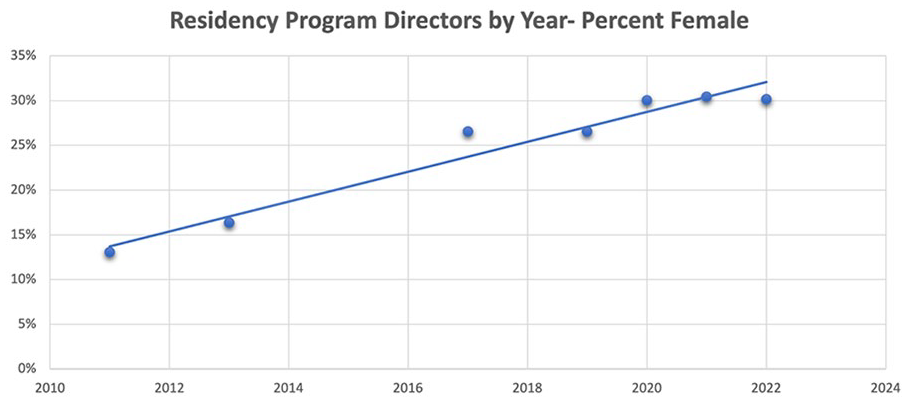
Published percentage of female Otolaryngology-Head and Neck Surgery residency program directors by year.
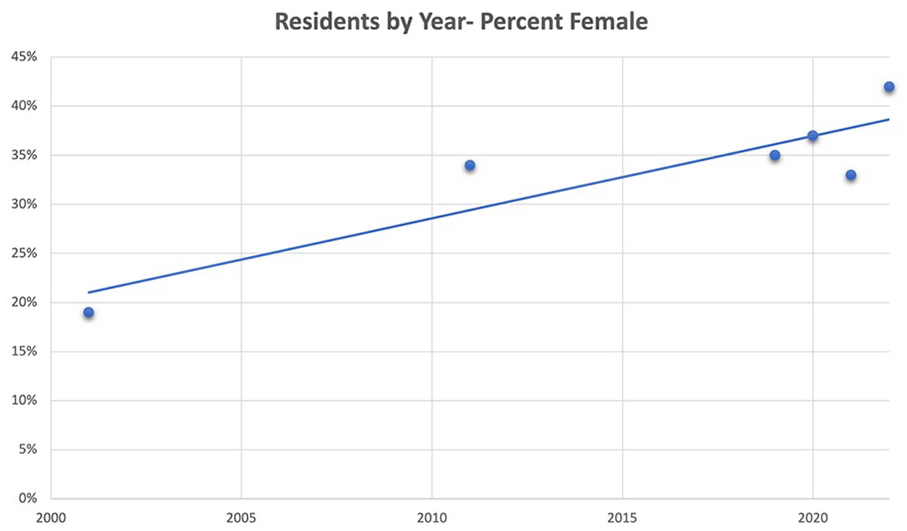
Published percentage of female Otolaryngology-Head and Neck Surgery resident physicians by year.
One hundred twenty-three academic OHNS residency programs were identified on cross-sectional analysis. No programs were excluded. The gender composition of residents, faculty, and academic leadership positions within OHNS residency programs is displayed in Table 1. As academic rank increases, the number of women in each position decreases. Forty-two percent of residents are women, whereas 26.6% and 8.1% of faculty and department chairs are women, respectively. Women accounted for 30% and 18% of residency program directors and fellowship directors, respectively. The fellowship director gender composition for all 8 recognized OHNS fellowships associated with academic residency programs may be found in Table 2. Ten women OHNS department chairs were identified, 1 of whom was in an interim position.
Academic Positions by Title and Gender (2022-2023 Academic Year).

Abbreviation: OHNS, Otolaryngology-Head and Neck Surgery.
OHNS Fellowship Directors Associated with Residency Program by Gender (2022-2023 Academic Year).

Abbreviation: OHNS, Otolaryngology-Head and Neck Surgery.
Gender of OHNS department chair was significantly correlated with proportion of women faculty. Of the programs with a female department chair, 33% of faculty were women and 67% were men compared to 27% women and 73% men for programs with a male OHNS or General Surgery department chair (P = .01). In fact, any woman in a leadership position (medical school dean, program director, fellowship director, and department chair) was correlated with a statistically significant increase in the percentage of women faculty. Programs with no women in leadership positions had a lower median percent of women faculty (23%) than programs with a woman in a leadership position (30%; P = .006).
Gender of OHNS department chair was not associated with the gender of OHNS residents or the gender of the fellowship director. There was also no association between the gender of the program director and the proportion of women residents or the percentage of women faculty and percent of women residents.
Discussion
The importance of women mentorship and role models in the recruitment, retention, and promotion of women in medicine has been well demonstrated in academic gastroenterology, urology, and plastic surgery.10,19,20 The findings in our study corroborate those of prior studies. There was a strong association between women in any academic leadership position, including OHNS department chair, and the number of women OHNS faculty. In contrast to other studies completed in surgical specialties, there was no association between OHNS chair gender and program director or fellowship director gender.10,19 There was also no association between the chair, program director, or faculty gender and the gender composition of current residents. These findings are consistent across recent publications that have investigated gender disparity across Otolaryngology leadership positions.12,14,16 This may be explained by the relatively low number of total woman chairs (8.1%) compared to a relatively higher number of woman residency program directors (37, 30.1%), fellowship directors (36, 18.8%), and residents (42%). The number of woman OHNS chairs has increased from less than 5% in 2019 to 8.1% in August 2022.4,12 It is possible that the growing number of women in leadership positions may contribute to the observed increase in the number of women in all levels of OHNS training and academic medicine.
Despite fewer women in the highest OHNS leadership positions, there has been increasing gender representation documented in the literature. In the 1980s, less than 1% of practicing Otolaryngologists were women with only 6 being represented in full-time academic positions. 17 In 2008, 29.8% of OHNS residents were women, a number that has steadily increased to 35% in 2019 and 42% in 2022.12,21 In fact, a recent analysis concluded that OHNS has the highest rate of women residents of any of the surgical specialties other than obstetrics and gynecology. 22 Despite these advances and the consistent rise in the number of woman residents, the proportion of women is smaller as academic rank increases. 3 Pereira et al found that women made up 37% of assistant and associate professors but only 10% of full professors in 2022 and male gender was a statistically significant predictor of full professorship (P < .001). 3 In 2013, 16% of program directors were women with a rise to 27% in 2019 and 30% in 2022.11,12,14,16 However, there remains a significant decline in gender representation at the highest academic rank with less than 5% of department chairs being women prior to 2021.12,14 Although our study demonstrates a rise in this number to 8.1%, there is still significant room for improvement.
Despite a discrepancy in gender diversity at the highest leadership levels, our study demonstrates an association between women in any academic leadership position and an increased percentage of women OHNS faculty at that institution. This highlights the need for improvement in gender diversity across leadership positions. However, it is important to consider factors that may impact the gender representation disparity seen at higher leadership levels. The number of women medical school matriculants has rapidly increased over the past several decades from 11% in 1970 to 56% in 2021.1,23 Similarly, the number of women OHNS residents has steadily increased. This increase has resulted in a greater total number of women OHNS faculty members, but discrepancy at the mid to late-career level remains. OHNS department chairs appointed within the past 6 years have an average of 18 years of post-residency/fellowship experience, resulting in a significant time lag between initial faculty membership and department chair appointment. 13 Consequently, the increase in the number of OHNS residents and faculty over the past decade should result in growth at the highest leadership levels in the coming years. It is also important to consider differences in attrition rates between male and female surgeons. Recent research has demonstrated that women are up to 2 times more likely to leave academic surgery departments compared to men. 24 Although this has not been explored in OHNS specifically, it is likely that increased attrition rates among women in OHNS may impact the gender diversity seen at higher academic leadership ranks. Future research on factors impacting the retention of women in OHNS is needed.
Gender diversity in OHNS subspecialties is also variable. A recent query of 1421 members of the American Academy of Facial Plastic Surgery (AAFPRS) found 13.0% of members to be female compared to 86.9% male. 25 A similar study demonstrated that women more frequently apply for pediatric otolaryngology fellowship positions and less frequently for head and neck fellowship positions, with women fellowship applicants outnumbering men only in pediatric otolaryngology. 26 In addition, women account for only 12% of society leaders and 17.7% of editorial board members for major Otolaryngology journals.3,27 However, despite some persistent discrepancies in the number of woman subspecialty surgeons, there has been an increase in gender diversity from 3% of Head and Neck fellowship graduates in 2008 to 33% in 2018. 28
Gender diversity and the availability of role models who are women may significantly impact diverse recruitment and overall organizational success in both medicine and business. Recent literature has demonstrated that women value and understand the importance of same-sex mentorship at a rate higher than their male counterparts. 7 Women medical students are more likely to specialize in OHNS when their medical school has at least some full-time women faculty and enter residency programs with higher proportions of women residents. 9 Data from the urology match confirms this finding, with there being a statistically significant correlation between the proportion of matched women applications and the proportion of women faculty. 20 The impact of female representation on organizational success has also been well demonstrated in the areas of finance and business. Women in C-suite positions catalyze fundamental shifts in tolerance, openness to change, and creation strategies, with companies having strong woman leadership generating a return on equity of 10.1% per year compared to 7.4% for those without.29,30 In fact, field experiments have found that teams with an equal gender mix perform better than male-dominated teams in both sales and profits. 30 The importance of gender diversity, women mentorship, and women representation cannot be understated, and academic medicine should continue to focus on strategies to improve gender diversity.
There has been a significant amount of interest in the cause of inadequate promotion and retention of women. One hypothesis is the lack of adequate executive-level sponsorship, which inhibits high-achieving women from advancing into the highest leadership positions. 31 In medicine, lack of woman role models, decreased research productivity, harassment, and burnout have been cited as reasons for fewer women in these positions.4,6,32 -34 When women in academic leadership positions are asked to examine their own experience with tenure and promotion, the most common reasons for gender disparities are poorly defined goals, lack of standard promotion procedures, and vulnerability to discrimination. 34 Successful women also emphasize the perception that their male counterparts experience advancement differently. 34 Gender discrimination has been reported by 65.1% of women residents, who also report more frequent feelings of fatigue and burnout than men.6,34
Numerous organizations have aimed to improve upon these disparities with targeted mentorship and leadership programs. A recent systematic review of mentorship program implementation found these programs were consistently highly rated, with one program reporting an 85% retention rate for participating woman faculty. 35 Additional programs also report improvement in retention and recruitment into the department or specialty, highlighting the impact that formalized mentorship programs can have on women in academic medicine. 35 In 2017, the Society of General Internal Medicine successfully implemented the novel Career Advising Program, a longitudinal experience intended to foster the advancement of women in academic medicine by assisting woman faculty in the navigation of the academic promotion process. 36 The success of this and other mentorship programs highlights the impact of mentorship and sponsorship on increasing representation, retention, and promotion of women. Although we are aware of several mentorship programs within OHNS that aim to promote the advancement of women in the specialty, to our knowledge, no studies examining the impact of these initiatives have been published. We have recently implemented a Women in Otolaryngology leadership and mentorship curriculum for female residents within our institution and aim to publish on the effectiveness of this program. Future research on the impact of mentorship programs focused on women in OHNS is needed.
There are several limitations to our study. First, this is a cross-sectional study of current OHNS residency programs, which limits our analysis to a snapshot in time rather than an analysis of trends. The current study design also limits conclusions on causation and does not adequately assess the career motivations of residency program applicants and OHNS faculty. In addition, this study focuses on gender equity without considering the impact of other personal identities such as race and ethnicity. It is well known that gender, race, and ethnicity have a significant impact on pay equity and job promotion within academic medicine. Future research should investigate the impact of both gender and racial identity on the diversity of leadership positions as well as on resident and faculty cohorts within OHNS. Second, in this study, leadership is confined to academic rank. There are multiple leadership opportunities both in and out of academic medicine that should be considered when discussing leadership within OHNS. Women involved in quality improvement programs within their academic or private practice as well as those involved in national committees, editorial boards, and diversity, equity, and inclusion or wellness initiatives play significant roles in the advancement of women in the specialty. We also recognize the leadership value that funded women private investigators hold and commend them on their important contributions to the specialty. Inclusion of academic leadership positions alone is a significant limitation and future research should focus on the leadership endeavors of women across OHNS.
Third, data was obtained from program websites and social media, which has the potential to be inaccurate or outdated and may have influenced our results, although we consider this impact to be minor.
Finally, gender was assessed using personal pronouns and photographs available on departmental websites and does not conform to the gold standard of self-identified gender. In addition, this study focused on binary gender equity; however, a comprehensive evaluation of gender equity would include an analysis of those identifying as transgender and other gender minorities. Although no examined studies used nonbinary gender classifications, future research should aim to better confirm self-identified gender and should provide an inclusive analysis of nonbinary gender diversity.
Conclusion
Gender diversity and the availability of women mentorship and role models may have an impact on the promotion, retention, and recruitment of women in academic medicine. The proportion of women in Otolaryngology has increased over the past decade at the resident, faculty, program director, and department chair rank. Representation of women in any OHNS leadership position (medical school dean, program director, fellowship director, and department chair) is also correlated with an increase in OHNS women faculty. Although significant progress has been made, further understanding of how woman mentorship promotes gender equity is necessary to implement initiatives that promote the representation of women in Otolaryngology-Head and Neck Surgery.
Supplemental Material
sj-docx-1-ear-10.1177_01455613241282610 – Supplemental material for You Can’t Be What You Can’t See: The Progression of Women in Otolaryngology-Head and Neck Surgery
Supplemental material, sj-docx-1-ear-10.1177_01455613241282610 for You Can’t Be What You Can’t See: The Progression of Women in Otolaryngology-Head and Neck Surgery by Nicole G. DeSisto, Rahul K. Sharma, Elizabeth S. Longino, Alexandra S. Ortiz, Leslie R. Kim, Sarah L. Rohde and Shiayin F. Yang in Ear, Nose & Throat Journal
Footnotes
Data Availability Statement
The datasets generated during and/or analyzed during the current study are available from the corresponding author on reasonable request.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Considerations
Exemption status was obtained from the Institutional Review Board at Vanderbilt University Medical Center.
Consent to Participate
Not applicable.
Consent for Publication
Not applicable.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.